Construction of prediction models for prolonged length of postoperative hospital stay in patients undergoing primary total hip arthroplasty via direct anterior approach
Linjie Hu, Guosong Xu, Weiyi Chen, Yiqun Chen, Qichao Ou, Zhibin Wu, Guoxian Chen

TL;DR
This study identifies risk factors for longer hospital stays after hip surgery and creates a model to help doctors manage patient recovery better.
Contribution
A new predictive model using LASSO regression to identify risk factors for prolonged hospital stays after hip arthroplasty.
Findings
Higher BMI, longer operation time, and postoperative complications were linked to longer hospital stays.
The model achieved an AUC of 0.766, showing good predictive accuracy.
The model's calibration and decision curve analysis confirmed its clinical usefulness.
Abstract
To investigate the risk factors associated with prolonged postoperative length of stay (PLOS) in patients undergoing primary total hip arthroplasty (THA) via direct anterior approach (DAA) and develop a perioperative dynamic prediction nomogram for optimizing the perioperative management of THA. This single-center, retrospective cohort study analyzed the perioperative clinical data of patients who underwent primary THA through DAA by a single surgical team at our institution between September 2022 to September 2024. Patients were divided into two groups based on postoperative hospital stay duration: the normal group (PLOS < 6 days) and the prolonged group (PLOS > 6 days). LASSO regression was used to screen variables, multivariate logistic regression was applied to establish the model and then a nomogram was developed. The area under the curve (AUC) of receiver operating characteristic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
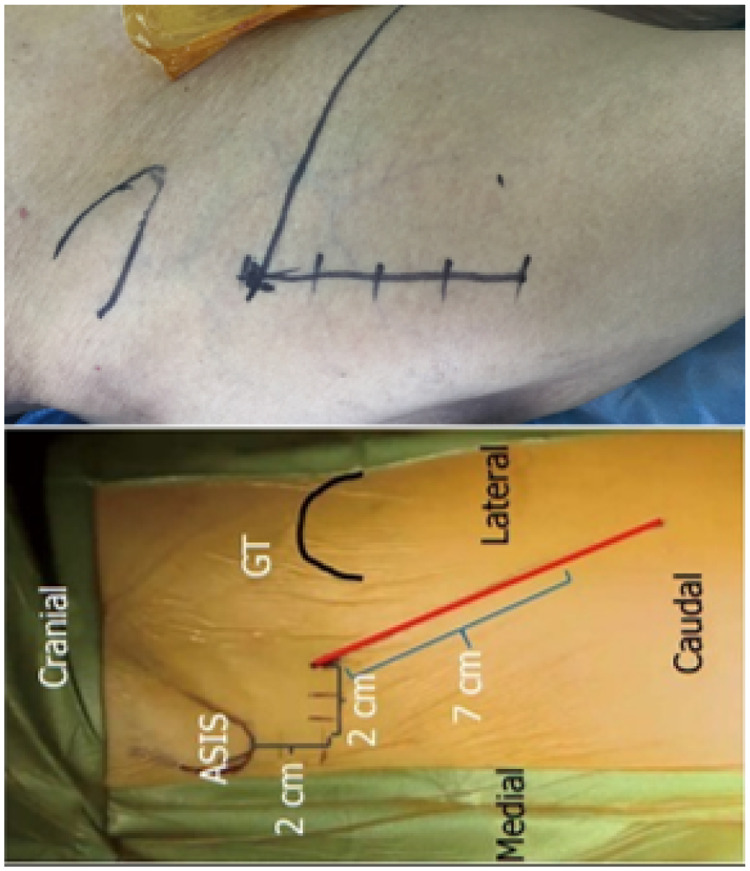 Figure 1
Figure 1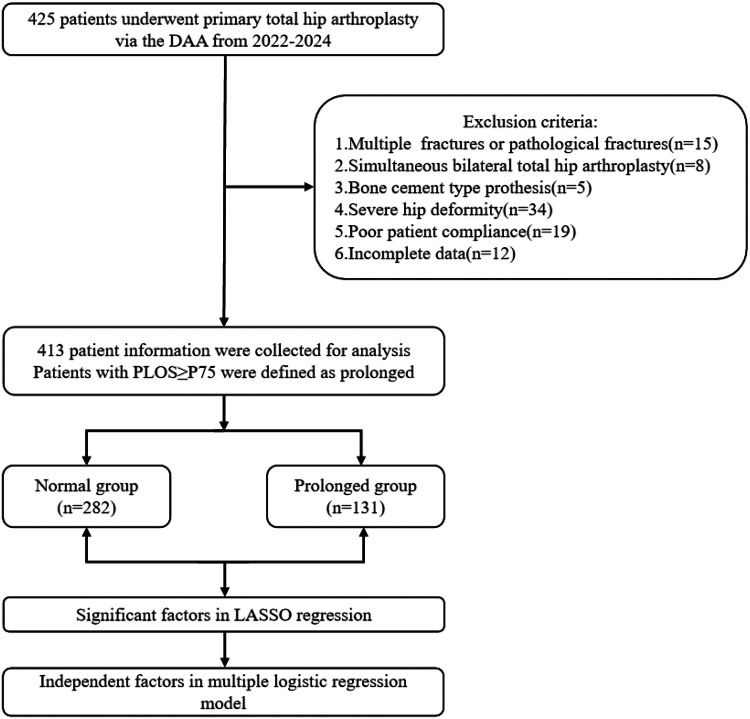 Figure 2
Figure 2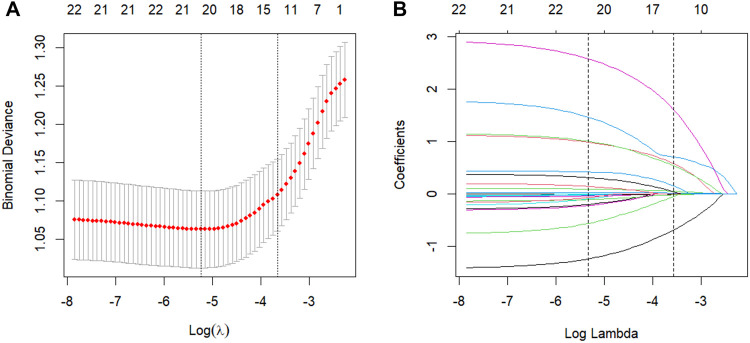 Figure 3
Figure 3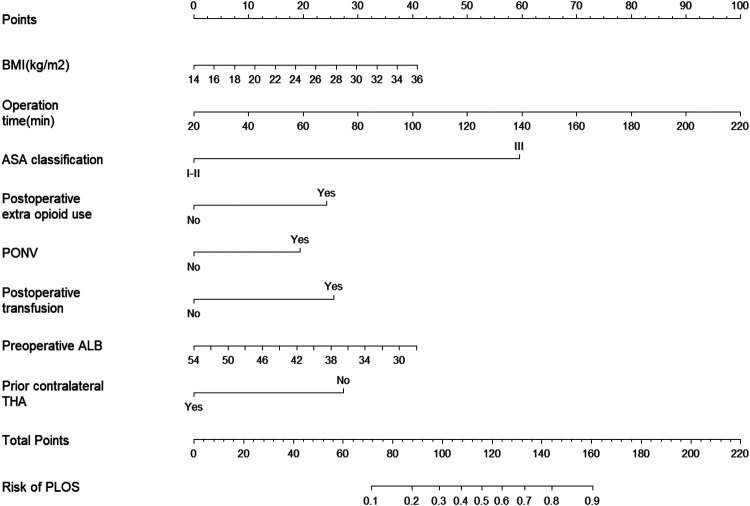 Figure 4
Figure 4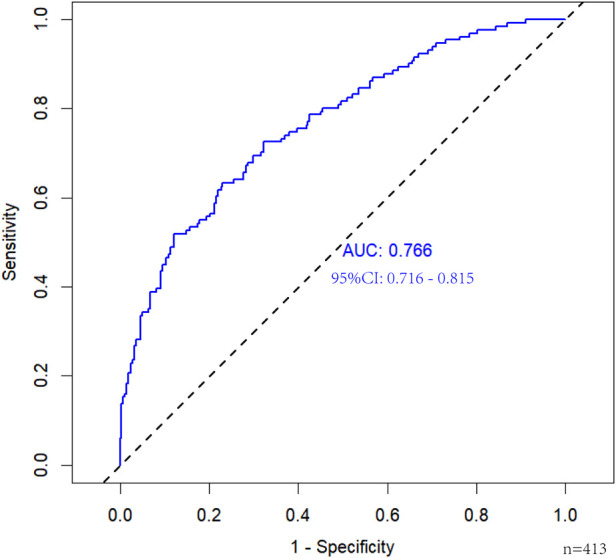 Figure 5
Figure 5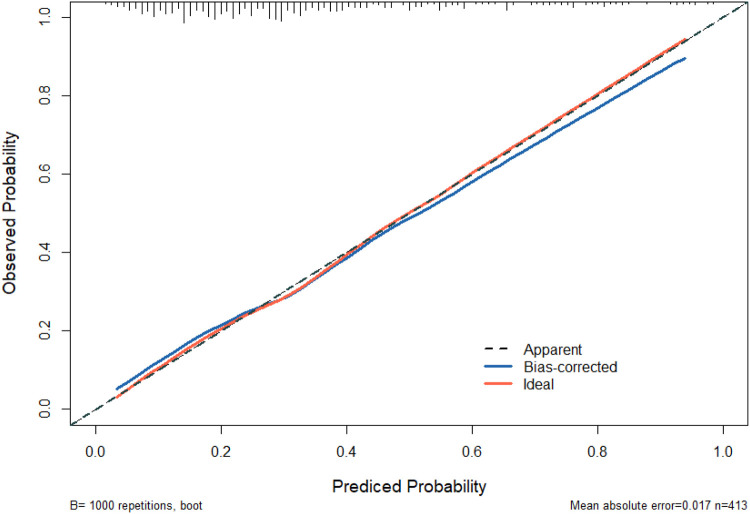 Figure 6
Figure 6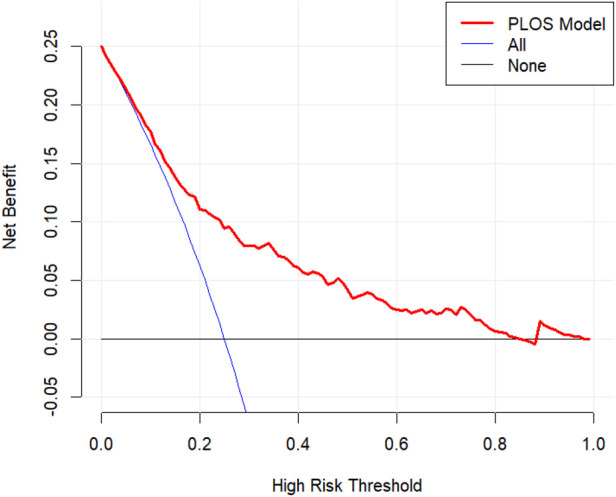 Figure 7
Figure 7| Characteristics | Total ( | Normal ( | Prolonged ( |
|
|---|---|---|---|---|
| Gender | 0.764 | |||
| Male | 162 (39.2%) | 112 (39.7%) | 50 (38.2%) | |
| Female | 251 (60.8%) | 170 (60.3%) | 81 (61.8%) | |
| Age (years) | 64.72 ± 11.21 | 64.47 ± 10.49 | 65.24 ± 12.65 | 0.515 |
| BMI (kg/m2) | 23.20 ± 3.42 | 22.88 ± 3.18 | 23.89 ± 3.80 | 0.009 |
| Operation time (min) | 74.73 ± 19.92 | 72.30 ± 16.80 | 79.95 ± 24.64 | 0.002 |
| Type of anesthesia | 0.644 | |||
| CSEA | 371 (89.8%) | 252 (89.4%) | 119 (90.8%) | |
| GA | 42 (10.2%) | 30 (10.6%) | 12 (9.2%) | |
| ASA classification | <0.001 | |||
| I–II | 402 (97.3%) | 280 (99.3%) | 122 (93.1%) | |
| III | 11 (2.7%) | 2 (0.7%) | 9 (6.9%) | |
| Comorbidity | 0.051 | |||
| No | 243 (58.8%) | 175 (62.1%) | 68 (51.9%) | |
| Yes | 170 (41.2%) | 107 (37.9%) | 63 (48.1%) | |
| Indications | 0.174 | |||
| OA | 127 (30.8%) | 91 (32.3%) | 36 (27.5%) | |
| FNF | 68 (16.5%) | 52 (18.4%) | 16 (12.2%) | |
| DDH | 125 (30.3%) | 81 (28.7%) | 44 (33.6%) | |
| ONFH | 93 (22.5%) | 58 (20.6%) | 35 (26.7%) | |
| Postoperative extra opioid use | 0.005 | |||
| No | 384 (93.0%) | 269 (95.4%) | 115 (87.8%) | |
| Yes | 29 (7.0%) | 13 (4.6%) | 16 (12.2%) | |
| PONV | <0.001 | |||
| No | 322 (78.0%) | 233 (82.6%) | 89 (67.9%) | |
| Yes | 91 (22.0%) | 49 (17.4%) | 42 (32.1%) | |
| Postoperative transfusion | <0.001 | |||
| No | 358 (86.7%) | 259 (91.8%) | 99 (75.6%) | |
| Yes | 55 (13.3%) | 23 (8.2%) | 32 (24.4%) | |
| Preoperative Hb (g/L) | 130.55 ± 13.75 | 132.03 ± 13.19 | 127.38 ± 14.43 | 0.001 |
| Preoperative HCT (%) | 39.42 ± 3.95 | 39.86 ± 3.84 | 38.47 ± 4.02 | <0.001 |
| Preoperative ALB (g/L) | 41.78 ± 3.91 | 42.14 ± 4.00 | 41.01 ± 3.60 | 0.006 |
| Postoperative Hb (g/L) | 111.99 ± 14.92 | 112.96 ± 14.43 | 109.90 ± 15.78 | 0.052 |
| Postoperative HCT (%) | 33.71 ± 4.40 | 33.96 ± 4.28 | 33.16 ± 4.64 | 0.086 |
| Postoperative ALB (g/L) | 35.25 ± 3.12 | 35.60 ± 3.17 | 34.50 ± 2.90 | <0.001 |
| Osteoporosis | 0.975 | |||
| No | 195 (47.2%) | 133 (47.2%) | 62 (47.3%) | |
| Yes | 218 (52.8%) | 149 (52.8%) | 69 (52.7%) | |
| DVT | 0.488 | |||
| No | 345 (83.5%) | 238 (84.4%) | 107 (81.7%) | |
| Yes | 68 (16.5%) | 44 (15.6%) | 24 (18.3%) | |
| Type of prosthesis | 0.442 | |||
| Corail | 289 (70.0%) | 194 (68.8%) | 95 (72.5%) | |
| Tri-Lock BPS | 124 (30.0%) | 88 (31.2%) | 36 (27.5%) | |
| Prior contralateral THA | <0.001 | |||
| No | 340 (82.3%) | 220 (78.0%) | 120 (91.6%) | |
| Yes | 73 (17.7%) | 62 (22.0%) | 11 (8.4%) |
| Variables | Univariate logistic regression analysis | Multivariate logistic regression analysis | ||
|---|---|---|---|---|
| OR (95% CI) |
| OR (95% CI) |
| |
| BMI | 1.091 (1.026–1.162) | 0.006 | 1.096 (1.024–1.175) | 0.009 |
| Operation time | 1.019 (1.009–1.031) | <0.001 | 1.025 (1.012–1.039) | <0.001 |
| ASA classification | 10.328 (2.614–68.397) | 0.003 | 18.895 (3.962–145.091) | <0.001 |
| Comorbidity | 1.515 (0.997–2.305) | 0.052 | NA | |
| Indications | ||||
| OA | — | — | — | — |
| FNF | 0.615 (0.328–1.103) | 0.115 | NA | |
| DDH | — | — | — | — |
| ONFH | 1.408 (0.864–2.274) | 0.165 | NA | |
| Postoperative extra opioid use | 2.879 (1.343–6.280) | 0.007 | 3.314 (1.420–7.876) | 0.006 |
| PONV | 2.244 (1.388–3.625) | <0.001 | 2.603 (1.504–4.524) | <0.001 |
| Postoperative transfusion | 3.640 (2.040–6.590) | <0.001 | 3.538 (1.821–6.987) | <0.001 |
| Preoperative Hb | 0.975 (0.959–0.990) | 0.002 | NA | |
| Preoperative HCT | 0.911 (0.860–0.962) | 0.001 | NA | |
| Preoperative ALB | 0.928 (0.878–0.979) | 0.007 | 0.926 (0.870–0.984) | 0.014 |
| Postoperative ALB | 0.889 (0.827–0.952) | <0.001 | NA | |
| Prior contralateral THA | 0.325 (0.157–0.618) | 0.001 | 0.259 (0.116–0.530) | <0.001 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTotal Knee Arthroplasty Outcomes · Anesthesia and Pain Management · Cardiac, Anesthesia and Surgical Outcomes
Introduction
1
Total hip arthroplasty (THA) is considered one of the most successful surgical innovations of the twentieth century (1). Owing to its excellent clinical outcomes and high patient satisfaction, it remains the gold standard treatment for end-stage hip disease. The direct anterior approach (DAA) utilizes the natural intermuscular plane between the tensor fasciae latae and sartorius muscles (the Hueter interval) to access the hip joint (2). This technique minimizes soft tissue trauma, facilitates early postoperative mobilization, enhances recovery, and can reduce the length of hospital stay (3). Over the past decade, the adoption of minimally invasive surgical (MIS) techniques and the principles of Enhanced Recovery After Surgery (ERAS) in arthroplasty have facilitated a substantial increase in the performance of same-day joint replacement procedures. It is projected that by 2026, over half of all primary THA procedures in the United States will be performed in an outpatient setting (4). Same-day discharge management for selected patients undergoing primary THA has been demonstrated to be a safe, efficient, and cost-effective approach (5–7). Consequently, the utilization of same-day THA programs has shown a steady annual increase (8). However, same-day discharge hip arthroplasty has not yet been widely adopted in China. Currently limited to a few large medical institutions, its implementation lacks standardized protocols, which hinders quality control and widespread dissemination of this practice.
Our institution performed its first same-day discharge DAA-THA in January 2020. While minimizing surgical invasion, reducing pain, and accelerating recovery are central to our department's clinical objectives, a subset of patients continues to experience a significantly prolonged postoperative length of stay (PLOS). A prolonged postoperative hospital stay is frequently associated with the occurrence of perioperative adverse events. This not only increases the utilization of healthcare resources but may also adversely affect the patient's rehabilitation process (9). Currently, a validated tool for assessing the risk of extended hospitalization following primary DAA-THA is lacking. We developed a pragmatic predictive model by analyzing clinical data from our institution. This study aims to identify the key risk factors for prolonged stay after DAA-THA, with the goal of optimizing perioperative management and informing the development of same-day THA programs in China.
Materials and methods
2
Study population
2.1
This single-center retrospective study analyzed data from the Orthopedic Department records of Putian First Hospital. The cohort included patients who underwent primary DAA-THA between September 2022 and September 2024. Exclusion criteria were: (1) multiple or pathological hip fractures; (2) simultaneous bilateral procedures; (3) use of cemented prostheses; (4) severe hip deformity; (5) poor patient compliance; and (6) incomplete clinical data.
Surgical methods
2.2
All procedures were performed with the patient in the supine position on a standard folding orthopedic table, with the symphysis pubis aligned to the table's pivot point. A 6 cm–8 cm incision was made along the midline of the tensor fasciae latae muscle, beginning approximately 2 cm distal and 2 cm lateral to the anterior superior iliac spine (Figure 1). All primary THA operations were performed by the same surgical team. The lead surgeon was a senior attending physician with experience in over 300 DAA procedures. The same set of minimally invasive instruments was used for all cases, and a cementless prosthesis (DePuy Synthes, USA) was implanted in every patient.
Surgical incision for total hip arthroplasty through the direct anterior approach.
Perioperative management
2.3
A standardized multimodal analgesia protocol was employed. Preoperative administration of non-steroidal anti-inflammatory drugs (NSAIDs) was used for preemptive analgesia. Postoperative pain management consisted of patient-controlled analgesia pumps, scheduled NSAIDs (e.g., celecoxib), and ice therapy. Supplemental opioid analgesics were administered as needed based on individual patient pain assessment. Our perioperative transfusion protocol was initiated on postoperative day 1. Routine blood and biochemical tests were monitored serially. Transfusion was indicated for patients with a hemoglobin level below 80 g/L accompanied by symptoms of anemia, such as palpitations or chest tightness. For asymptomatic patients with similar hemoglobin levels, close observation and serial blood tests were maintained. Patients with hemoglobin levels between 80 and 100 g/L were considered for transfusion if they exhibited unstable vital signs or significant clinical symptoms, including tachycardia (heart rate > 100 bpm), hypotension (systolic blood pressure < 90 mmHg), cardiac chest pain, congestive heart failure, unexplained tachycardia, or hypotension refractory to fluid resuscitation. Patients were deemed ready for discharge upon meeting the following criteria: the ability to ambulate independently and safely on level ground with a walking aid; demonstrated understanding and correct performance of prescribed home exercises (e.g., ankle pumps, quadriceps isometric contractions, straight leg raises) by both the patient and their caregiver; stable vital signs; laboratory values within acceptable limits; a clean, dry surgical incision without signs of infection; adequate pain control; and the absence of other complications.
Data collection
2.4
Patient demographic and perioperative data (encompassing preoperative baseline characteristics, intraoperative events, and early postoperative outcomes) were collected from the electronic medical record system. Demographic variables included sex, age, body mass index (BMI), surgical indication (osteoarthritis [OA], femoral neck fracture [FNF], developmental dysplasia of the hip [DDH], osteonecrosis of the femoral head [ONFN]), comorbidities (including hypertension and diabetes), osteoporosis, and history of contralateral THA. Perioperative variables encompassed operation time, anesthesia type (general or combined spinal-epidural), American Society of Anesthesiologists (ASA) physical status classification, postoperative extra opioid use, occurrence of postoperative nausea and vomiting (PONV), postoperative blood transfusion, preoperative and postoperative hemoglobin (Hb) and hematocrit (Hct) levels, preoperative and postoperative albumin (Alb) levels, occurrence of deep vein thrombosis (DVT), femoral stem type (Corail or Tri-Lock BPS), and length of postoperative hospital stay.
Statistical analysis
2.5
Statistical analyses were performed using IBM SPSS (version 25.0) and R software (version 4.4.1). Continuous variables are presented as mean ± standard deviation (X ± SD), while categorical variables are expressed as proportions or percentages. Group comparisons for continuous variables were conducted using independent samples t-tests or Mann–Whitney U tests, as appropriate. For categorical variables, Chi-square or Fisher's exact tests were employed. Variables were selected from multiple potential predictors using the Least Absolute Shrinkage and Selection Operator (LASSO) regression method. The model was fitted using the “glmnet” package in R. Prior to analysis, all continuous variables were standardized using Z-scores to ensure comparability of regression coefficients. We assessed multicollinearity by calculating the variance inflation factor (VIF < 5) for all candidate predictors. To maintain model simplicity and interpretability, our final model focuses on main effects and does not include interaction terms. Factors identified by LASSO regression were subsequently included in univariate and multivariate logistic regression analyses to control for potential confounding effects. A backward stepwise selection process, guided by minimizing the Akaike Information Criterion (AIC), was employed to identify independent risk factors significantly associated with prolonged postoperative hospital stay. These factors were incorporated into a nomogram based on the multivariate regression analysis. The performance of the predictive model was evaluated using several metrics, including the concordance index (C-index), area under the receiver operating characteristic curve (AUC), calibration curves, and decision curve analysis (DCA). Internal validation was performed using bootstrapping with 1,000 replicates to calculate a corrected concordance index (C-index), ensuring model accuracy and reliability (10). Calibration was assessed by comparing predicted probabilities against observed outcomes, where closer alignment indicated better performance. Finally, DCA was employed to quantify the net benefit across various threshold probabilities, evaluating the clinical utility of the nomogram. A P-value of less than 0.05 was considered statistically significant.
Result
3
Patient cohort
3.1
Based on the predefined inclusion and exclusion criteria, 413 patients were included in the final analysis. The PLOS, the primary outcome measure, was not normally distributed and was therefore described using median and interquartile range (IQR). In the absence of a standard national or international definition for a prolonged hospital stay after DAA-THA, and given the variability in discharge criteria across institutions, we defined prolonged length of stay (PLOS) as a postoperative stay greater than or equal to the 75th percentile of our cohort's distribution. Patients with a PLOS greater than or equal to the 75th percentile of the distribution were defined as the prolonged group (11). Accordingly, 282 patients with a PLOS of less than 6 days (the 75th percentile, P75) were classified into the normal group, while the remaining 131 patients with a PLOS of 6 days or longer comprised the prolonged group (Figure 2). The two groups' perioperative characteristics and complete patient data, including demographics, are shown in Table 1. Between the two groups, statistically significant variations were detected in ASA classification, PONV, postoperative transfusion, prior contralateral THA, preoperative HCT and postoperative ALB (all P < 0.001). Compared to patients with normal PLOS, patients with prolonged PLOS were more likely to present higher BMI (P = 0.009), longer operative time (P = 0.002), postoperative extra opioid use (P = 0.005), lower preoperative Hb (P = 0.001), and lower preoperative ALB (P = 0.006). No significant differences were observed between the two groups in terms of gender, age, type of anesthesia, indications, osteoporosis, DVT, type of prosthesis, postoperative Hb or postoperative HCT (all P > 0.05).
The flowchart.
Variables selection
3.2
Fourteen variables with non-zero coefficients were selected from 24 initial candidates using LASSO regression with the one-standard-error (1-SE) criterion (Figure 3). These predictors included: BMI, operation time, ASA classification, comorbidity, FNF, ONFH, postoperative extra opioid use, PONV, postoperative transfusion, preoperative Hb and Hct levels, preoperative and postoperative ALB levels, and history of contralateral THA. Univariate analysis was first performed on these 14 predictors, followed by multivariate logistic regression analysis. Ultimately, eight independent risk factors for prolonged PLOS were identified, as presented in Table 2: BMI, operation time, ASA classification, postoperative extra opioid use, PONV, postoperative transfusion, preoperative ALB level, and prior contralateral THA.
Demographic and clinical feature selection using the LASSO binary logistic regression model. (A) Parameter selection in the LASSO model used ten-fold cross-validation via minimum criteria. Partial likelihood deviance (binomial deviance) curves and logarithmic (lambda) curves were plotted. Dotted vertical lines were drawn at the optimal values by using the minimum standard and the 1 SE of the minimum standard (1-SE standard). (B) LASSO coefficient profiles of the 24 features. In the present study, predictor's selection was according to the 1-SE standard (right dotted line). LASSO, least absolute shrinkage and selection operator; SE, standard error.
Nomogram construction and validation for PLOS
3.3
The independent risk factors identified through multivariate analysis were incorporated into a predictive model. A nomogram was subsequently developed to visually represent the results of the logistic regression analysis (Figure 4). The nomogram demonstrated good discriminatory ability, with an AUC of 0.766 (95% CI: 0.716–0.815) in the primary cohort. Internal validation using 1,000 bootstrap replicates yielded a corrected AUC of 0.745, confirming the model's robust performance (Figure 5). The calibration curve demonstrated strong agreement between the observed prolonged PLOS and the predicted probabilities (Figure 6).
Nomogram for predicting the risk of prolonged postoperative length of stay for primary total hip arthroplasty via DAA.
The ROC analysis for the predictive model.
Calibration curve comparing predicted probabilities of prolonged PLOS against observed outcomes. The dashed diagonal line represents the ideal perfect calibration, where predictions exactly match observations. The solid line represents the performance of the nomogram, with closer alignment indicating better predictive accuracy.
Clinical application
3.4
DCA was performed to evaluate the clinical utility of the predictive model. This method quantifies the net benefit of using the nomogram across various threshold probabilities. The analysis demonstrated that the model provides a superior net benefit for predicting prolonged PLOS risk at threshold probabilities between 2% and 85% (Figure 7), indicating its clinical value for both clinicians and patients within this range.
Analysis of the decision curve for the prolonged PLOS prediction model.
Discussion
4
Over one million THA procedures are performed globally each year, and this number continues to rise due to an aging population (12). THA has become a highly standardized procedure. With the implementation of Enhanced Recovery After Surgery (ERAS) protocols, the average length of hospital stay for THA has decreased, reducing healthcare costs and accelerating patient recovery (13). Shortening the hospital stay following hip arthroplasty is safe, as current evidence indicates it does not increase the risk of complications or readmission (14–17). For a major procedure like THA, the extent of soft tissue injury significantly influences the pace of recovery. In the early development of same-day THA, minimally invasive surgical approaches were proposed to reduce postoperative complications, with the two-incision technique being one example (18). As minimally invasive techniques have gained popularity, many patients specifically seek surgeons proficient in the DAA (19). The DAA minimizes soft tissue damage and has become the most common technique for same-day THA in recent studies (20). The average length of stay (LOS) is widely used as a composite metric to evaluate healthcare resource utilization, quality of care, and hospital management efficiency (21). The total length of the perioperative hospital stay is influenced by numerous factors. Therefore, the PLOS serves as a more precise indicator of a patient's rate of recovery following surgery. A prolonged PLOS is generally associated with higher costs, increased readmission rates, and more complications (22, 23). Therefore, efforts to reduce the LOS should be pursued, provided that the standard of care is not compromised. This study focuses on identifying risk factors for a prolonged hospital stay following primary DAA-THA. The aim is to optimize perioperative management, facilitate faster recovery, and guide patient selection for same-day THA procedures.
To our knowledge, this is the first study to develop and validate a nomogram for predicting prolonged PLOS following DAA-THA. A meta-analysis by Ramadanov et al. compared DAA-THA outcomes across different surgical table setups. While it found no significant differences in functional scores, radiographic outcomes, or complication rates, it did not evaluate differences in postoperative length of stay (24). The PLOS is influenced by multiple factors, including patient-specific characteristics, surgical variables, and institutional perioperative management protocols. These variations result in significant differences in PLOS across healthcare facilities, thereby limiting direct comparability. In this study, the prolonged postoperative length of stay (PLOS) was defined as a duration greater than or equal to the 75th percentile of the distribution for the included cases, corresponding to ≥6 days. This retrospective study of 413 patients undergoing DAA-THA identified the following independent risk factors for prolonged PLOS: BMI, operation time, ASA classification, postoperative extra opioid use, PONV, postoperative transfusion, preoperative ALB levels, and prior contralateral THA. Based on these eight factors, we developed a visual nomogram that provides an intuitive and accurate prediction of the probability of extended hospitalization following primary DAA-THA. A recent meta-analysis compared the mid- and short-term outcomes of different surgical approaches for total hip arthroplasty, indicating that the SuperPATH approach is associated with superior short-term results. Future work should focus on quantifying differences in predictive models across these various approaches (25).
The association between BMI and outcomes following THA has been extensively studied, yet remains controversial (26–30). Several studies have reported that obesity is associated with higher rates of adverse events, including wound complications, dislocation, revision surgery, and readmission (27, 31). The prolonged hospital stay observed in patients with obesity may be attributable to this increased risk of complications. A retrospective analysis by Hilal et al. of 8,973 patients who underwent THA at the Mayo Clinic between 2000 and 2008 demonstrated that obesity significantly increased both the length of hospitalization and costs, even in the absence of postoperative complications (28). Our study also identified elevated BMI as an independent risk factor for prolonged LOS following primary DAA-THA. Furthermore, it is evident that excess adipose tissue in the surgical field can obscure anatomical landmarks and complicate exposure, thereby increasing procedural difficulty. Consequently, particularly careful perioperative management is warranted for patients with obesity.
THA has become a highly standardized procedure. Operation time and intraoperative blood loss are commonly used as indicators of surgical complexity. Prolonged operative duration has been consistently associated with an increased risk of short-term complications following THA, including surgical site infection, periprosthetic joint infection, and the need for postoperative transfusion (32). Our study similarly found that extended operation time was associated with a higher risk of prolonged PLOS. Therefore, without compromising the quality of the procedure, efforts should be made to minimize operation time to facilitate patient recovery. The ASA Physical Status classification system is widely used to assess a patient's preoperative health and surgical risk. Previous studies have established that patients with more significant comorbidities require a longer postoperative recovery period (26, 33–35). Consistent with this, our study identifies an ASA classification greater than II as an independent factor significantly associated with a prolonged postoperative hospital stay. Therefore, surgeons should prioritize the management of patients with a high ASA classification. Implementing multidisciplinary interventions for these patients can reduce perioperative stress and complications, thereby enhancing recovery.
Effective postoperative pain management is a critical component of perioperative care for THA and a key criterion for patient discharge (36). Multimodal analgesic protocols, which minimize reliance on opioids, have been consistently associated with a reduced length of hospital stay (37–40). This is significant, as opioid use is linked to adverse events that can impede recovery. Evidence suggests that discontinuing opioid use prior to surgery can significantly enhance functional recovery after THA (41). Corroborating this, our study found that additional postoperative opioid requirement was independently associated with a longer hospital stay. Consequently, minimizing perioperative opioid use is recommended to reduce the risk of adverse events and facilitate patient recovery (42). A potential limitation of our model is the reliance on “additional postoperative opioid requirement” as the sole pain-related metric. By not incorporating pain intensity scores or differences in regional analgesic techniques, this measure may not fully capture the impact of postoperative pain on discharge readiness. PONV is a common complication following joint arthroplasty, with reported incidence rates as high as 83% after major orthopedic surgery (43). Beyond patient discomfort, PONV can lead to serious sequelae such as dehydration, electrolyte imbalance, wound dehiscence, and aspiration pneumonia (44). These complications may prolong hospitalization, increase healthcare costs, and ultimately impede recovery. In line with these findings, our study identified PONV as an independent risk factor for delayed discharge following DAA-THA. At our institution, PONV prophylaxis and management are primarily achieved pharmacologically, utilizing agents such as metoclopramide and ondansetron. Patients undergoing THA face a considerable risk of perioperative blood transfusion, with reported rates ranging from 15.9% to 29.8% (45). Perioperative transfusion increases the risk of surgical site infection, thromboembolic events, cardiopulmonary complications, longer hospital stays, higher costs, and even mortality (46, 47). In a retrospective study of 2,104 primary THA patients, Monsef et al. found that allogeneic blood transfusion was associated with prolonged hospitalization, regardless of the number of units transfused (48). Our study further identifies perioperative transfusion as an independent risk factor for extended length of stay following THA, perioperative blood management represents a critical component of enhanced recovery protocols following THA. In our study, preoperative Hb and Hct were significant in univariate analysis but not in the multivariate model. We hypothesize that this may be because postoperative blood transfusion demonstrated a stronger association with prolonged length of stay. Therefore, the primary clinical goal in managing preoperative anemia is to prevent the need for postoperative transfusion.
Furthermore, our analysis identified low preoperative albumin as an independent risk factor for prolonged postoperative hospitalization. Reduced serum albumin decreases colloid osmotic pressure, leading to fluid accumulation in the interstitial space. This may manifest as wound exudate at the surgical site, impairing healing and increasing the risk of perioperative complications. In a retrospective study of 19,975 patients undergoing primary THA, Daniel reported that hypoalbuminemia was associated with a higher incidence of surgical site infection, pneumonia, prolonged LOS, and readmission (49). Therefore, preoperative assessment of serum albumin levels is essential, and nutritional support should be optimized for patients with hypoalbuminemia.
Notably, our study found that patients with a history of contralateral THA had a lower risk of delayed discharge. This may be attributed to differences in patient-specific factors and prior perioperative experience. These patients likely have more realistic expectations, better compliance with perioperative management protocols, and greater familiarity with the rehabilitation process. To leverage this effect, we recommend developing center-specific patient education materials that systematically outline the entire perioperative journey. Such resources would empower patients by optimizing their cognitive, behavioral, and psychological preparedness, thereby facilitating recovery.
Limitations
5
This study has several limitations. First, as a single-center retrospective analysis conducted exclusively in a Chinese population with a relatively small sample size, the findings may be subject to selection bias. Second, complete data on perioperative complications were unavailable; some non-mandatory complications, such as transient hypotension, were not systematically recorded. These omissions were primarily random, attributable to variations in documentation practices. Nonetheless, their potential association with PLOS cannot be ruled out. Finally, the use of 6 days as the threshold for prolonged PLOS may limit generalizability, as average hospital stay durations can vary substantially across institutions. Future prospective, multi-center studies with larger sample sizes are needed to validate these results and refine the predictive model.
Conclusion
6
This study identified BMI, operation time, ASA classification, postoperative extra opioid use, PONV, postoperative transfusion, preoperative ALB levels, and history of contralateral THA as independent factors associated with delayed discharge following DAA-THA. Based on a comprehensive set of perioperative variables, we developed a nomogram to predict prolonged LOS after primary DAA-THA that demonstrated good predictive accuracy. This tool may assist clinicians in stratifying patient risk, optimizing perioperative management, enhancing surgical safety, facilitating recovery, and informing patient selection for same-day THA procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Learmonth ID Young C Rorabeck C. The operation of the century: total hip replacement. Lancet. (2007) 370(9597):1508–19. 10.1016/s 0140-6736(07)60457-717964352 · doi ↗ · pubmed ↗
- 2Spina M Luppi V Chiappi J Bagnis F Balsano M. Direct anterior approach versus direct lateral approach in total hip arthroplasty and bipolar hemiarthroplasty for femoral neck fractures: a retrospective comparative study. Aging Clin Exp Res. (2021) 33(6):1635–44. 10.1007/s 40520-020-01696-932910422 · doi ↗ · pubmed ↗
- 3Bourget-Murray J Horton I Meniawy SE Papp S Kim PR Grammatopoulos G. The direct anterior approach is safe and shortens hospital length of stay following hemiarthroplasty for neck of femur fracture. Injury. (2023) 54(4):1186–90. 10.1016/j.injury.2023.02.01636775793 · doi ↗ · pubmed ↗
- 4De Cook CA. Outpatient joint arthroplasty: transitioning to the ambulatory surgery center. J Arthroplasty. (2019) 34(7s):S 48–50. 10.1016/j.arth.2019.01.00630773355 · doi ↗ · pubmed ↗
- 5Debbi EM Mosich GM Bendich I Kapadia M Ast MP Westrich GH. Same-day discharge total hip and knee arthroplasty: trends, complications, and readmission rates. J Arthroplasty. (2022) 37(3):444–8.e 1. 10.1016/j.arth.2021.11.02334808278 · doi ↗ · pubmed ↗
- 6Goyal N Chen AF Padgett SE Tan TL Kheir MM Hopper RH Jr Otto aufranc award: a multicenter, randomized study of outpatient versus inpatient total hip arthroplasty. Clin Orthop Relat Res. (2017) 475(2):364–72. 10.1007/s 11999-016-4915-z 27287858 PMC 5213925 · doi ↗ · pubmed ↗
- 7Weiser MC Kim KY Anoushiravani AA Iorio R Davidovitch RI. Outpatient total hip arthroplasty has minimal short-term complications with the use of institutional protocols. J Arthroplasty. (2018) 33(11):3502–7. 10.1016/j.arth.2018.07.01530107958 · doi ↗ · pubmed ↗
- 8Vega AN Ziemba-Davis M Hicks SA Meneghini RM Buller LT. Time required for planned and unplanned episodes of care in primary total joint arthroplasty: has anything changed with a growth in outpatient arthroplasty? J Arthroplasty. (2021) 36(4):1195–203. 10.1016/j.arth.2020.10.01533218843 · doi ↗ · pubmed ↗