Post-pandemic increase of Group A streptococcal infections in adults: a retrospective cohort study from 2012 to 2024
Anne Kathrin Lösslein, Tessa Goerne, Roland Elling, Tobias Wengenmayer, Georg Häcker, Paul Marc Biever

TL;DR
This study shows that Group A streptococcal infections increased in adults after the pandemic, similar to what was seen in children.
Contribution
The study provides new evidence on the post-pandemic rise of GAS infections specifically in adult populations.
Findings
There was a significant increase in hospitalized adult patients with GAS infections post-pandemic (IRR 2.94).
ICU admissions for GAS infections also rose significantly (IRR 2.5) after pandemic restrictions were lifted.
The increase in GAS infections among adults persisted into 2024 without returning to pre-pandemic levels.
Abstract
After the COVID-19 pandemic an increase in Group A streptococcal (GAS) infections was reported mostly for children in several countries worldwide. However, data on infections in adults remain limited. Therefore, we focus on the pre- and post-pandemic incidence of GAS infections in adults, the need for intensive care treatment and the microbiological sampling patterns. We performed a retrospective cohort study of hospitalized adult patients from 2012 to 2024, based on a positive GAS detection in their routine microbiological sampling. We compared the post-pandemic phase after lifting the isolation measures in April 2022 to the pandemic and pre-pandemic phase. Additionally, we analysed positive rapid assessment tests in children, indicative of the prevalence of GAS tonsillitis in this population. In the post-pandemic months, we observed a significant increase in overall hospitalized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
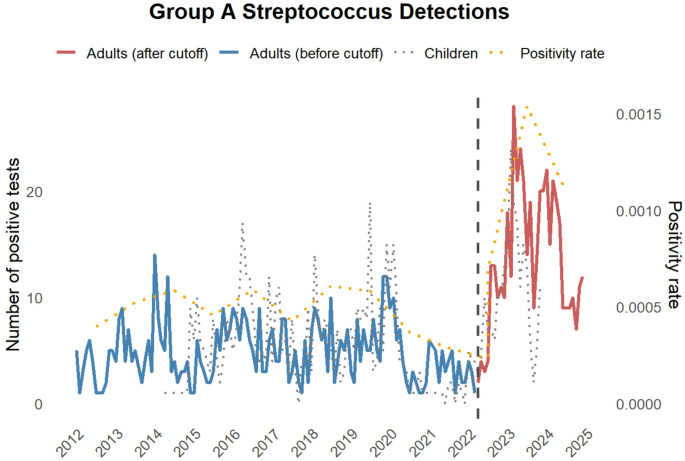 Figure 1
Figure 1- —Universitätsklinikum Freiburg (8975)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeonatal and Maternal Infections · Streptococcal Infections and Treatments · Infective Endocarditis Diagnosis and Management
Introduction
The COVID-19 pandemic due to SARS-CoV2 was accompanied by worldwide infection control measures, including wearing of masks and isolation measures. In Germany, several lockdowns starting from 2020 were an integral part of the public health measures. On April 3rd 2022, restrictions were lifted. The implemented measures had a long-term impact not only on the epidemiology of SARS-CoV2, but also on that of various other pathogens and diseases worldwide, some of which have become apparent only in retrospect. For instance, respiratory viruses showed atypical seasonality [1, 2], the tuberculosis incidence temporarily decreased during the pandemic [3] and Mycoplasma pneumoniae infections showed a delayed but significant re-appearance after the pandemic [4]. Group A streptococci (GAS) can cause a broad range of clinical symptoms, from pharyngitis to severe wound infections and toxic shock syndrome [5]. An increase in GAS infections has been reported after the pandemic, in particular in children [6, 7]. This increase is not limited to Scarlet fever but extends to invasive GAS (iGAS) infections [8]. Data on GAS infections in adult patients, in particular the incidence in the recent post-pandemic years, are limited [9]. We therefore conducted a retrospective analysis of pre- and post-pandemic GAS infections in adult patients receiving inpatient treatment at a tertiary-care hospital in southern Germany.
Methods
Study design and data collection
We conducted a retrospective cohort study of adult patients with detection of GAS in the routine microbiological diagnostics during their stay at the University Medical Center Freiburg from 2012 to 2024. The microbiological results with GAS detection per year including the time point of material collection and type of specimen were extracted from the laboratory software [M/lab] (DORNER Health IT Solutions). Patients who only received treatment in the outpatient clinics were excluded from the analysis. ICU/IMC (Intensive Care Unit/Intermediate Care Unit) treatments, length of hospital stay, outcome and epidemiological data (age and sex) were extracted from electronical health records. The microbiological specimens were categorized as invasive materials (blood culture, spinal fluid, tissue samples/biopsies, puncture material (aspirates), drain secrete, tracheal secretion, bronchoalveolar lavage, intraoperative swabs) and non-invasive materials (sputum, general swabs, urine). The local Data Integration Center (DIZ) provided the retrospective data of rapid antigen testing for GAS in children from suspected GAS tonsillitis cases, which were collected and analysed in house using Sofia^®^ Strep A + Fluorescent Immunoassay (FIA) (QuidelOrtho™) lateral-flow-assay with the Sofia^®^ 2 Analyzer (QuidelOrtho™) at the Center for Paediatrics at the University Medical Center Freiburg between April 2014 and November 2023. Data before April 2014 were not digitally available. Inconclusive test results were disregarded. In addition, we extracted the total number of microbiological test orders per year at the Institute of Medical Microbiology and Hygiene of the University Medical Center Freiburg.
Statistical analysis
Statistical analyses were performed using RStudio (R version 4.3.3) and GraphPad Prism 10. Continuous variables were compared using unpaired two-tailed t-tests, and categorical variables using Fisher’s exact test. To account for differences in exposure time across periods, incidence rate ratios (IRRs) were calculated using Poisson regression. A piecewise linear regression analysis was performed to evaluate trend changes in positivity rates, referring to all requested microbiological analyses. A p-value < 0.05 was considered statistically significant; IRRs were reported with 95% confidence intervals.
Results
We included 1,034 case records of adult patients who received inpatient treatment at the University Medical Center Freiburg between 2012 and 2024, and in whom GAS had been detected by microbiological sampling in the course of normal care. There was a sharp increase in the incidence of GAS detection in 2023 and 2024 compared to previous years (Fig. 1). The GAS positivity rate remained stable from 2012 through early 2022 but showed a significant increase starting in April 2022. Piecewise regression revealed a statistically significant change in trend (p = 0.003), with a marked rise in positivity rates post cut-off. We compared our findings to the results of GAS rapid assessment tests (RAT) from oropharyngeal specimens performed in children. Here, a drop in 2021 became apparent. In this outpatient setting, an increase in positive RAT tests in children was seen in the post-pandemic phase (data available only till November 2023), which suggests uncomplicated GAS infections also increased. As most isolation measures in Germany were lifted on April 3rd, 2022 — with mask mandates remaining only in high-risk settings and public transportation — we defined this date as the beginning of the post-pandemic phase. We then compared the subsequent data to previous years, with a particular focus on cases requiring intensive care. Similar to a significantly increased incidence rate ratio of GAS infections in adults (2.94 fold, [2.56–3.33]), the need for ICU treatment among GAS patients increased (2.5 fold, [1.82–3.45]), (Table 1). Notably, there were no significant differences in median age, the rate of fatal outcomes or the median duration of the hospital stay (Table 1).
Fig. 1. Group A Streptococcus detections in hospitalized adult patients in the routine microbiological sampling before (blue) and after (red) the relaxation of isolation and contact measures (3rd April 2022, dashed line). The grey dotted line represents rapid assessment testing in children in the emergency department and the yellow dotted line represents the GAS positivity rate compared to all microbiological tests requested
Table 1. Overview of epidemiological characteristics and the hospital stay of all adult patients and the subgroup of ICU patients separately before and after relaxation of isolation measures (cut-off date 3rd April 2022). The percentages refer to the respective patient numbers. * Test positivity rate calculated by piecewise linear regression analysisTotalBefore cut-off dateAftercut-off dateP valueIncidence Rate Ratio (CI)P value Observation
period (d) 474837441003 all patient cases
1034
583
451 2.94(2.56–3.33) < 0.001 all patient cases/1000 observations days217.78155.72449.65 Sex (f)451 (43.6%)253(43.4%)176(39.2%)0.162 Age45.89(SD 17.46)45.98(SD 17.97)45.78(SD 16.8)0.8519 ICU162(15.67%)97(16.64%)65(14.41%)0.34372.5(1.82–3.45) < 0.001 Outcome (death)37(3.6%)20(3.43%)17(3.77%)> 0.999 Length of hospital stay (d)11.52(SD 14.31)11.7(SD 12.43)11.3(SD 16.46)0.6531 patient cases with proof of GAS in invasive sample581 (56.2%)345 (59.18%)236 (52.33%) 0.0316 2.56(2.17–3.03) < 0.001
subgroup ICU
162
97
65 2.50(1.82–3.45) < 0.001 ICU patient cases/1000 observations days34.125.964.8 Sex (f)63(38.9%)34(35.1%)29(44.6%)0.2515 Age56.36(SD 17.14)56.78(SD 16.89)55.74(SD 17.75)0.7058 Outcome (death)34(20.10)18(18.56%)16(24.6%)0.4317 Length of hospital stay (d)23.57(SD 22.76)21.77(SD 17.19)26.26(SD 28.96)0.2212 ICU patient cases with proof of GAS in invasive sample133 (82.1%)78 (80.41%)55 (84.62%)0.53722.63(1.85–3.7) < 0.001
Total number of microbiological test requests 1.617.0431.225.379391.664 Detection of GAS per tests (positivity rate)0.00063940.00047580.0011515 0.0032*
We stratified the microbiological samples as invasive and non-invasive samples as illustrated in the method section. Both in the entire patient collective (2.56 fold, [2.17–3.03]) and the ICU subgroup (2.63 fold, [1.85–3.7]), we found a significantly increased incidence rate ratio for the detection of GAS in invasive samples (Table 1) after the pandemic. Nevertheless, the percentage of invasive samples was stable or even decreased (Table 2), which suggests that the rise in GAS infections also extends to GAS detections in non-invasive samples, typically associated with milder infections. The percentage distribution of detections in specific materials remained largely constant, with the exception of a reduction in intraoperative swabs in the overall cohort (Table 2).
Table 2. Details on the microbiological sampling with proof of GAS of the cohort in Table 1. The percentages refer to the patient numbers in Table 1Microbiological sampling with proof of GASTotalBefore cut-off dateAfter cut-off dateP value all patient cases (Table 1) 1034
583
451 Invasive sample numbers in all patient cases6994012980.1147 Blood culture83 (8%)45 (7.72%)38 (8.43%)0.7295 Tissue sample/ biopsy152 (14.7%)80 (13.72%)72 (15.96%)0.3306 Aspirate93 (8.99%)44 (7.55%)49 (10.86%)0.0791 Intraoperative swab315 (30.46%)199 (34.13%)115 (25.50%) 0.0027 Deep respiratory specimen47 (4.55%)29 (4.97%)18 (3.99%)0.5475 Spinal fluid2 (0.19%)02 (0.44%)0.1900 Drainage fluid7 (0.68%)3 (0.51%)4 (0.89%)0.4776 subgroup ICU (Table 1) 162
97
65 Invasive sample numbers in ICU-subgroup188105830.4209 Blood culture41 (25.31%)22 (22.68%)19 (29.23%)0.3623 Tissue sample/ biopsy48 (29.63%)30 (30.93%)18 (27.69%)0.7270 Aspirate24 (14.81%)13 (13.4%)11 (16.92%)0.6526 Intraoperative swab39 (24.07%)20 (20.62%)19 (29.23%)0.1950 Deep respiratory specimen31 (19.14%)18 (18.56%)13 (20.0%)0.8407 Spinal fluid1 (0.62%)01 (1.54%)0.4012 Drainage fluid4 (2.47%)2 (2.06%)2 (3.08%)> 0.999
Discussion
Our retrospective analysis highlights the increase of detected GAS infections after the COVID-19 pandemic not only in children but also in adult patients, similar to other reports, and with a particular focus on ICU admissions and the type of microbiological sampling. Interestingly, this increase in incidence was remained through 2024, with possibly a return to pre-pandemic patterns in 2025 (Fig. 1). We found an increase in GAS detections in both invasively and non-invasively collected microbiological samples. Although we detected an absolute increase in associated ICU admissions per 1,000 days after lifting the isolation measures, the relative proportion of ICU admissions was stable. This indicates that we do not only observe an increase of invasive and severe GAS infections in adults, but a general increase also of milder infections [10]. Higher virulence of the now circulating strains seems unlikely. The higher number of RAT tests in children in 2023 also suggests higher GAS circulation rates in the population. Orieux et al. [11] analysed the GAS-associated ICU admissions to several hospitals in France, where they found a higher proportion of influenza co-infections. Therefore, a possible explanation might be that the recurrence of viral infections, for which protection was also previously provided by masks and contact restrictions, also favours a rise in GAS infections [11, 12]. However, this would most likely not explain the increase in non-respiratory infections, such as wound infections caused by GAS. In addition, the exposure to GAS was reduced during the pandemic, in particular in children, which might be associated with decreased immunity to GAS in the overall population and consequently higher susceptibility after relaxation of isolation measures [13]. Moreover, there is evidence for an emergence of specific emm-types [14]. Whole-genome sequencing of GAS isolates from a hospital in northern Germany also revealed the presence of the hypervirulent M1_UK_ lineage in invasive GAS infections [15]. Interestingly, the increase in GAS detection was observed across all sampled materials and apparent infection severity (invasive vs. non-invasive, ICU vs. non-ICU), indicating that the range of clinical manifestations has not changed and that a sampling bias can unlikely explain the increase of cases. Our study emphasizes the need for awareness of the ongoing increased incidence of (i)GAS in adults, as a return to pre-pandemic levels is not yet certain. Follow-up studies will be required to understand the development in coming years and to evaluate long-term effects of the pandemic.
Limitations of the study
We performed a monocentric retrospective study with a focus on microbiologic GAS detections. Moreover, clinical details such as infection focus, comorbidities, or severity scores were not available in a structured digital format. To mitigate this limitation, we carefully assessed microbiological materials, distinguishing invasive from non-invasive samples, Additionally, transferred patients with external GAS confirmation may have been missed, potentially underestimating incidence. The analysis of positivity rates supports a genuine rise in GAS detections; however, potential shifts in clinical sampling practices over time cannot be fully ruled out. In addition, the isolates were not available for systematic serotyping.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Holdstock V, Heppenstall E, Corrigan D, Eccleston A, Jones L, Kalima P, et al. National 10-year cohort study of Life-threatening invasive group A Streptococcal infection in Children, 2013–2023. Pediatr Infect Dis J. n.d. 10.1097/INF.0000000000004855. 10.1097/INF.0000000000004855.PMC 1242261040359236 · doi ↗ · pubmed ↗