Radiotherapy regimens and concurrent Cabergoline use for non-functioning pituitary neuroendocrine tumors: a large, single-center cohort
Geovanne Pedro Mauro, Lucas Gonçalves Rebello, Leila Maria Da Róz, Vinicius de Carvalho Gico, Eduardo Weltman, Evandro César de Souza, Rafael Loch Batista, Malebranche Berardo Carneiro da Cunha Neto, Rosangela Correa Villar

TL;DR
This study examines the effectiveness of radiotherapy and cabergoline in treating non-functioning pituitary tumors, finding good control with low toxicity.
Contribution
The study provides new insights into the effectiveness of different radiotherapy regimens and cabergoline use in non-functioning pituitary tumors.
Findings
Radiotherapy provides good tumor control with low toxicity in non-functioning pituitary tumors.
Cabergoline use did not influence treatment outcomes.
No significant differences were found between single-dose and fractionated radiotherapy regimens.
Abstract
The standard treatment for non-functioning pituitary neuroendocrine tumors (PitNET) consists in transsphenoidal surgical resection, however when progression or recurrence happens, additional treatments like stereotactic radiotherapy (SRT) and dopaminergic agonists can be used. In this article we aim to describe and quantify the impact of SRT regimen and dose, as well as the use of concurrent cabergoline, on local tumor control and toxicities. This is a retrospective cohort of patients with non-functioning PitNET treated between 2008 and 2023 with LINAC-based SRT on different dose regimens with or without cabergoline, in a single university hospital. One-hundred twenty-six (126) patients were assessed. Median follow-up was 62.6 months (7.1 – 135.8 months). Most patients already had a visual deficit (65.1%) or hormonal dysfunction (52.4%) before SRT. Lesion size (median larger diameter…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
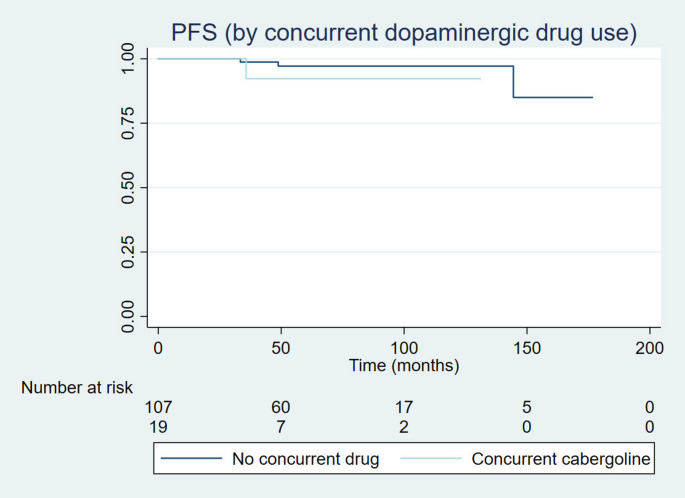 Figure 1
Figure 1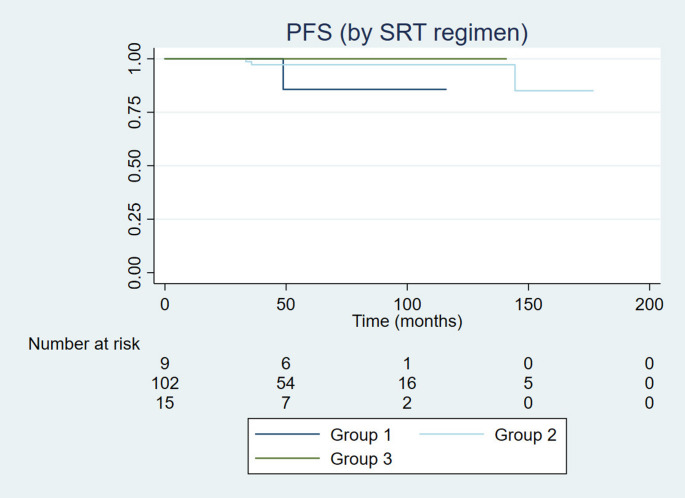 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPituitary Gland Disorders and Treatments · Neuroendocrine Tumor Research Advances · Meningioma and schwannoma management
Background
Non-functioning pituitary neuroendocrine tumors (PitNET) [1], formerly called non-functioning pituitary adenomas, are a large share of pituitary lesions, one that is often diagnosed latter than their secretive counterparts [2]. The standard treatment is focused on transsphenoidal surgical resection, but some patients may present residual tumors or progressive disease after one or more surgical approaches [3].
However, after disease progression there are no current standard recommendations for residual tumors. In such cases, radiotherapy and medical treatments can be considered based on patient profile [3]. The optimal radiotherapy regimen is not known, and multiple different techniques can be used with varying results [4]. Regarding medical treatments, dopaminergic agonists (mostly cabergoline) have been proposed to prevent tumor progression [5], also with mixed results [6]. Cabergoline has also been proposed as the primary treatment of NF-PitNETs, but the medical literature on this topic is still incipient [7, 8]. Since cabergoline seems to be a safe option in the NF-PitNET management, it has been tried in some cases to avoid SRT [9, 10]. The synergy between SRT and cabergoline, as well as timing for each treatment, has not been described previously to our knowledge.
In this report, our primary objectives are to comprehensively describe and quantify the impact of stereotactic radiotherapy (SRT) regimen and dose, and if the use of concurrent cabergoline would impact on progression-free survival and SRT-related toxicities.
Patients and methods
All patients with a clinical and histopathological diagnosis of non-functioning PitNETs who were treated in the radiotherapy department of a large, academic hospital were assessed. All patients were treated between July 2008 and October 2023. Patients that were followed less than six months were excluded. All were treated in a LINAC-based setting.
Inclusion criteria were patients with no evidence of pituitary hormonal production and according to the immunohistochemistry (IHC) analysis.
SRT dose groups were divided between patients that were treated with single fraction and different doses of fractionated SRT. Group 1 was treated with single-dose stereotactic radiosurgery (SRS) with doses of 15 to 22 Gy; Group 2 received lower doses of RT (48.6 –50.4 Gy) in a hypofractionated regimen of at least 27 fractions of 180 cGy (FRT); and Group 3 received 54 Gy in a hypofractionated regimen of 30 fractions. The choice of method (SRS or FRT) was decided in a multidisciplinary tumor board consisting of radiation oncologists, radiologists, neurosurgeons, and medical physicists. The choice between methods was based on total volume and proximity to optic chiasm to respect dose constraints.
Concurrent cabergoline use was considered if patients had been using the medication for at least two weeks before the start of treatment and continued taking it throughout the SRT course. Its use, as altered hormone levels, were consistently assessed by the endocrinology team throughout follow-up.
Follow-up regarding tumor progression was done by MRI. This imaging study was requested twice a year for the first two years and annually afterwards. Survival was calculated from date of first RT treatment. Response was assessed by RECIST 1.1 guidelines.
Visual, nervous, and hormonal assessment were done every six months during follow-up. Campimetry was favored for all patients, but it was not mandatory. Endocrine function was assessed pre- and post-SRT using serum levels of free thyroxine (fT4), thyroid-stimulating hormone (TSH), cortisol, adrenocorticotropic hormone (ACTH), prolactin (PRL), growth hormone (GH), insulin-like growth factor-1 (IGF-1), follicle-stimulating hormone (FSH), luteinizing hormone (LH), testosterone, and estradiol. Hypopituitarism was characterized following criteria previously published [11].
Statistical analyses were conducted to evaluate survival outcomes and group differences. The Fisher’s exact test and chi-square test were applied to compare categorical variables across groups. Survival time was defined as the interval from the date of radiotherapy to the last follow-up or event and was assessed using the Kaplan-Meier method. The primary endpoints included overall survival (OS) and progression-free survival (PFS). Toxicity outcomes included survival free of new visual deficits (NVDFS), survival free of new hormonal deficits (NHDFS), and the incidence of radionecrosis, stroke, CNS bleeding, and second malignancies. Univariate comparisons of survival curves were performed using the log-rank test. Local ethics approved this retrospective study. This research was not founded by any funding agencies in the public, commercial, or not-for-profit sectors.
Results
One-hundred twenty-six (126) patients were included. Mean age at treatment was 51.7 years. Patients were well balanced between genders (male/ female: 49.2/ 50.8%). Most patients already complained of visual deficit by first visit to RT clinic (65.1%) and met criteria for hypopituitarism (52.4%). Only 45 (35.7%) had campimetry assessment before RT, of those only 9 (20.0%) did not report any visual fields deficits.
Demographic characteristics were assessed. Results for those can be seen in Table 1.
Table 1. Demographic featuresPatients’ characteristicsN = 126Age < 50 years52 (41.3%) > 50 years74 (58.7%)Gender Male62 (49.2%) Female64 (50.8%)Size < 3 cm80 (63.5%) > 3 cm46 (36.5%)Type Null cell105 (83.3%) Silent gonadotrophic21 (16.7%)Previous visual deficit No44 (34.9%) Yes82 (65.1%)Altered campimetry No36 (28.6%) Yes9 (7.1%) No previous campimetry81 (64.3%)Compressed chiasm (MRI) No50 (39.7%) Yes76 (60.3%)Previous hypopituitarism No60 (47.6%) Yes66 (52.4%)
Median lesion size was 2.8 cm (range 0.7 to 7.8 cm; interquartile interval 25% 1.8 cm to 75% 3.7 cm). All patients had undergone previous pituitary surgery. Median interval between first surgery and RT treatment was 27.7 month (3.0–231.9 months). Mean number of previous surgeries was 1.75 surgeries (1–5 surgeries) before referral to RT. Most patients were diagnosed with compressed or dislocated optic chiasm (76/ 60.3%) before RT. There were no re-irradiation patients.
We assessed the difference between RT groups. Group 1 consisted of nine (N = 9) patients with median dose of 18 Gy (15–22 Gy). Groups 2 (N = 102) and 3 (N = 15) were treated with a median dose of 50.7 Gy (45–54 Gy). Dose to optic chiasm were constrained to 54 Gy, nevertheless three patients received doses superior to 54 Gy to the structure. Mean maximum RT dose to chiasm was 48.5 Gy (range 41.8 to 57.4 Gy; interquartile interval 25% 50.1 Gy – 75% 52.6 Gy). Among RT groups, the biggest differences were that patients who were treated with single fraction SRS had lower rates of previous visual deficit (p = 0.001), lower rates of altered campimetry before treatment (p = 0.009), and lower rates of chiasmatic compression (p = 0.006). Different RT treatments did not impact outcomes.
We also assessed differences based on the concomitant use of cabergoline. Median dose of cabergoline prescribe was 0.55 mg/ week. Most patients (85/ 67.4%) did not receive dopaminergic agonist treatment during follow-up. However, approximately one-third of the participants used cabergoline concomitantly. No significant differences were observed between the cabergoline and non-cabergoline groups. Moreover, neither prior nor concurrent cabergoline use had an impact on clinical outcomes. The data regarding the comparison among groups are reported in Table 2.
Table 2. Baseline characteristics of patients stratified by concurrent Cabergoline use and radiotherapy regimensN = 115Concurrent cabergolineRadiotherapyNoN = 107 (84.9%)YesN = 19(15.1%) p Group 1N = 9 (7.1%)Group 2N = 102(81.0%)Group 3N = 15(11.9%) p Age < 50 years45 (42.1%)7 (36.8%)0.674 (44.4%)42 (41.2%)6 (40.0%)0.97 > 50 years62 (57.9%)12 (63.2%)5 (55.6%)60 (58.8%)9 (60.0%)Gender Male56 (52.3%)13 (68.4%)0.094 (44.4%)50 (49.0%)10 (66.7%)0.41 Female51 (47.7%)6 (31.6%)5 (55.6%)52 (51.0%)5 (33.3%)Size < 3 cm66 (61.7%)14 (73.7%)0.318 (89.9%)63 (61.8%)9 (60.0%)0.29 > 3 cm41 (38.3%)5 (26.3%)1 (11.1%)39 (38.2%)6 (40.0%)Type Null cell90 (84.1%)15 (79.0%)0.528 (88.9%)84 (82.4%)13 (86.7%)1.00 Silent gonadotrophic17 (15.9%)4 (21.0%)1 (11.1%)8 (17.6%)2 (13.3%)Previous visual deficit No39 (36.4%)5 (26.3%)0.398 (88.9%)33 (32.3%)3 (20.0%) 0.001 Yes68 (63.6%)14 (73.7%)1 (11.1%)69 (67.7%)12 (80.0%)Altered campimetry No8 (21.6%)1 (12.5%)0.483 (100%)5 (13.5%)1 (20.0%) 0.009 Yes29 (78.4%)7 (87.5%)032 (86.5%)4 (80.0%) No previous campimetry70116659Compressed chiasm (MRI) No43 (40.2%)7 (36.8%)0.788 (88.9%)36 (35.3%)6 (40.0%) 0.006 Yes64 (59.8%)12 (63.2%)1 (11.1%)66 (64.7%)9 (60.0%)Previous hypopituitarism No54 (50.5%)6 (31.5%)0.126 (66.7%)50 (49.0%)4 (26.7%)0.14 Yes53 (49.5%)13 (68.5%)3 (33.3%)52 (51.0%)11 (73.3%)Concurrent cabergoline No---9 (100%)86 (84.3%)12 (80.0%)0.44 Yes016 (15.7%)3 (20.0%)RT groups I9 (8.4%)00.44---- II86 (80.4%)16 (84.2%) III12 (11.2%)3 (15.8%)
Median follow-up was 62.4 months (6.6–176.6 months). There were two reported deaths. Median OS, PFS, and NVDFS were not reached. Median NHDFS was 89.6 months. Rates at 5 years for OS, PFS, NVDFS and NHDFS were 98.4%, 96.8%, 94.4%, and 80.9%, respectively. There was no difference in OS ([HR], 0.89; 95% CI, 0.33–23.5; p = 0.94), PFS ([HR], 0.20; 95% CI, 0.22–1.95; p = 0.17) (Figs. 1 and 2), NVDFS ([HR], 0.89; 95% CI, 0.17–4.45; p = 0.88), and NHDFS ([HR], 0.69; 95% CI, 0.33–1.46; p = 0.33) between SRT regimen groups. There was neither for the use of concurrent cabergoline, as in OS ([HR], 0.45; 95% CI, 0.0–77.5; p = 0.50), PFS ([HR], 3.34; 95% CI, 0.30–37.3; p = 0.32) (Figs. 1 and 2), NVDFS ([HR], 12.0; 95% CI, 0.0–81.1; p = 0.12), and NHDFS ([HR], 0.80; 95% CI, 0.28–2.27; p = 0.67). Regarding new hormonal deficits, 38 patients developed new pituitary hormonal deficit. Five developed only glucocorticoid deficiency, five only thyrotropic deficiency, ten only growth hormone deficiency. A total of 18 developed multiple pituitary hormonal deficiencies. Two patients were submitted to treatment with temozolomide, one before and one after SRT, both in Group 2, without the use of concurrent cabergoline.
Fig. 1. Progression-free survival according to dopaminergic medication (cabergoline) use. Median PFS for both groups were not reached
Fig. 2. Progression-free survival according to RT technique and dose. Median PFS for all groups were not reached. Groups 1 was treated with SRS, Group 2 with low dose (< 54 Gy FRT, and Group 3 FRT with doses ≥ 54 Gy
Symptomatic radionecrosis was reported in only one patient, six years after SRT (dose to PTV was 50.4 Gy and to the chiasm was 49.9 Gy). Strokes and CNS bleeding were reported in three patients. The latency period between treatment and CNS bleeding/ strokes for those patients were 40.0, 49.4, and 105.3 months. There were no secondary malignancies reported.
Disease control was reported in 96.8% of patients by RECIST 1.1 criteria. All progression happened before 60 months of follow-up. There were one (0.7%) reported complete responses, partial responses were 30 (23.8%), stable disease were 91 (72.2%) and disease progression occurred in 4 (3.2%). No variable correlated to local control rate.
No variable impact neither OS nor NHDFS in the univariate analysis. The only variable to impact PFS was prior visual deficit (p = 0.02). Regarding NVDFS, previous symptomatic vision deficits correlated to new deficits after treatment, even asymptomatic ones (p = 0.01). No multivariate analysis was conducted based on these results. Results for univariate analysis can be seen in Table 3.
Table 3. Univariate analysis; performed using the log-rank test. No survival median values were reached N OSPFSNVDFSNHDFS5 year rate (%) p 5 year rate (%) p 5 year rate (%) p 5 year rate (%) p Concurrent cabergoline No10799.10.6298.10.2994.40.2580.40.67 Yes1910094.710094.7RT groups I91000.8088.90.321000.8877.70.62 II10299.198.095.180.4 III1510010093.393.3Age < 50 years521000.2298.10.771000.0884.60.78 > 50 years7498.697.391.979.7Gender Male621000.8996.70.2795.20.8279.00.32 Female6498.498.495.384.3Size < 3 cm801000.7397.50.4896.30.4886.30.94 > 3 cm4697.897.893.573.9Type Null cell10599.00.0898.10.7695.20.9482.90.65 Silent gonadotrophic2110095.295.276.2Previous visual deficit No441000.3193.1 0.02 97.70.6775.00.08 Yes8298.810093.985.4Altered campimetry No3694.4-1001.0097.2 0.01 83.30.22 Yes910010088.877.8 No previous campimetry8198.796.395.181.5Compressed chiasm (MRI) No501000.3096.00.2498.00.5580.00.40 Yes7698.798.793.483.0Previous panhypopituitarism No6098.30.9196.70.4198.30.1275.00.06 Yes6610098.592.489.4
Discussion
To our knowledge, this is the largest, retrospective cohort of exclusively non-functioning PitNET to be treated exclusively in a LINAC-setting to date. Retrospective analyses are always at risk of selection and register biases, but the size of this report makes it robust, and its data may be generalized. Amongst the novelties of our report are the exclusive use of LINAC-based and the comprehensive description of the prescription of cabergoline to patients undergoing SRT and the assessment of its timing. Although it is a large sample, most patients were treated with FRT. There was a limited number of patients that were submitted to single-fraction SRS and that may increase the risk of bias when comparing smaller groups.
Surgery is the cornerstone of the treatment of PitNETs. Most large publications on non-functioning PitNET describe surgical patients. The use of SRT after surgery is often reserved for progressive disease [12], as most patients may not require further treatment after first surgery [13]. SRT may improve local control, but there is no reported benefit of immediate adjuvant SRT over active surveillance after surgery, which could raise the number of patients submitted to SRT [14]. The necessity for SRT is very low, and most reports are under 20% [15–19], but can be higher in larger lesions or aggressive PitNETs [20]. Nevertheless, it which may not translate into more toxicities after treatment [21]. It is important to highlight that all patients reported here had their surgical options exhausted before SRT.
Regarding SRT techniques, most reports on PitNETs come from the experience with Gamma-Knife radiosurgery (GK). Historical and paramount publications on the matter are with the exclusive use of GK, reporting disease control of 87.3% [22] to 100% [23] with large follow-up [24–29]. Toxicities are also reported, most commonly new hormonal deficits of around 18–32% [30, 31]. Visual and neurological complications are less frequent, varying around 0% [32] to 13% [33]. The direct comparison between techniques cannot be compared outside a clinical trial. Our results of local control of 96.8%, new hormonal deficits of 29.4% and new visual deficits of 6.3% are compatible with previous GK publications. There are differences between both techniques, mostly regarding hot spots and planning techniques. Nevertheless, the results can be considered at least comparable.
One of our primary objectives was to determine the best SRT regimen in a LINAC-based setting. We compared the results of singe-dose SRS, and FRT with lower dose (40–50.4 Gy) or higher dose (54–56 Gy). We could not demonstrate superiority of any of those regimens in a LINAC-based setting for non-functioning PitNETs. Previous publications of smaller cohorts exclusively of non-functioning PitNETs and cohorts of patients with non-functioning and secretive lesions have shown similar results for LINAC-based SRT than those for GK, in terms of local control [34, 35] and toxicities [36, 37]. Previous publications also proposed that higher doses of FRT were unnecessary to achieve local control [38]. Another issue previously investigated is the comparison between singe-dose SRS and FRT, with mixed results [39–41]. Our results show similar conclusions that higher dose is not associated with better local control. It also shows that SRS is not superior to FRT, and the regimen should be chosen and tailored to the patients’ necessities and expectations.
Regarding the dose for FRT, it is important to highlight that our report and previously published data [38] have showed comparable results for doses between 45 and 50 Gy and the results for doses of 54 Gy and higher. We would suggest, as it is practice [2, 4] in most current guidelines, there is a lack of evidence favoring dose escalation in this disease and our results add to this conclusions and current practice.
Safety is a cornerstone for SRT regimen choice. The incidence of hormonal deficiencies after SRT has been previously demonstrated in larger retrospective cohorts of GK patients and must be kept in mind whenever prescribing SRT [42]. A noteworthy aspect of our report is that our cohort consisted exclusively of LINAC-treated patients with non-functioning PitNETs, where we applied a broader definition of pituitary hormonal deficiencies. In our study, the diagnosis was based on hormonal assessments rather than solely on the prescription of hormonal replacement therapy, as previously reported by Cordeiro et al. [34]. Neurological toxicities, however, are less dependent on SRT regimen [43–45] and may not impact quality of life [46].
The other primary endpoint of this report is to assess the impact of the concurrent use of dopaminergic agonists with SRT. Previous publications have reported some benefit [6, 11, 47] of cabergoline in non-functioning PitNETs management, and this may be an alternative to avoid or postpone SRT and its toxicities. They are however new and the drug have not been consistently prescribed for these patients in the past. The novelty in our report is that we did not find any beneficial association of cabergoline prior or concurrent to SRT. Previous smaller publications have suggested otherwise [48]. In this publication, the negative impact of combined treatment may come from the effect of cabergoline on cell cycle, which promotes an arrest at the radioresistant G1 phase. Nevertheless, that publication is small and comprised of both functioning and non-functioning PitNET. Another information that can be viewed as bias is the cut for concurrent use of cabergoline. This two-week period was used for three main reasons. First, it was the minimum interval for at least one half-life of the drug to be excreted. Second, the main reference we have on the manner is the very limited report of Takkar et al. (2020) [48]. Even though they haven’t reported what they would consider to be simultaneous delivery of cabergoline and SRT, they have stated that the smallest interval was 17 days. Third, because it usually takes two weeks between the first consultation for the radiation oncology department and treatment start, which could be consistently more accurate. We also haven’t demonstrated any enhancement in toxicities with the association of SRT and cabergoline. We discuss that cabergoline should be prescribed as necessary by the referring endocrinologist, without the concern for worse toxicities.
Despite providing novel data on the use of radiotherapy in the management of non-functioning PitNETs and being the first to assess the combined use of cabergoline in terms of radiotherapy efficacy and safety, this study has several limitations. It is a retrospective study, and the prescription of cabergoline was made by the attending physicians before the indication for radiotherapy, meaning that compliance with cabergoline use was not monitored. All included cases were unequivocally classified as non-functioning; however, the histological classification of these tumors did not follow the 2022 WHO criteria, limiting the evaluation of potential differences across tumor subtypes. Nonetheless, the low incidence of toxicities and the lack of impact of cabergoline use in most cases suggest that there are no subtle differences between non-functioning tumor subgroups regarding treatment outcomes.
Conclusion
This is a large, retrospective cohort of non-functioning PitNET patients treated with SRT in a LINAC-setting. We could not demonstrate any benefit comparing single-dose SRS and FRT in this population. Higher doses of FRT also did not translate into local control and dose escalation should not be favored. The use of cabergoline, prior or during SRT, did not impact outcomes. Prospective data is needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Fleseriu, M. Christ-Crain, F. Langlois, M. Gadelha, S. Melmed, (2024). Hypopituitarism. The Lancet.10.1016/S 0140-6736(24)00342-838735295 · doi ↗ · pubmed ↗
- 2R.L. Batista, E.B. Trarbach, M.D. Marques, V.A. Cescato, da G.O. Silva, C.G.B. Herkenhoff, N.R. Musolino, Nonfunctioning Pituitary Adenoma Recurrence and its Relationship with sex, size, and Hormonal Immunohistochemical Profile, vol. 120 (World neurosurgery, 2018), pp. e 241–e 24610.1016/j.wneu.2018.08.04330138730 · doi ↗ · pubmed ↗
- 3Kim, I., Yan, M., Sourour, M., et al. (2025). Pituitary neuroendocrine tumors treated with stereotactic radiosurgery. Journal of Neuro-Oncology, 171(2), 423-430.I. Kim, M. Yan, M. Sourour, R. Heaton, C. Faulkner, A. Kalyvas, D.S. Tsang, (2024). Pituitary neuroendocrine tumors treated with stereotactic radiosurgery. J. Neurooncol., 1–8 10.1007/s 11060-024-04864-3PMC 1169552039466561 · doi ↗ · pubmed ↗
- 4P. Slavinsky, M.S. González Pernas, K. Miragaya, J. Antico, A. Margni, M. Condomí Alcorta, D.A. Katz, Gamma Knife Radiosurgery in Pituitary Adenomas (A single-center experience, 2022)35037869 · pubmed ↗
- 5V. Narayan, N. Mohammed, S.C. Bir, A.R. Savardekar, D.P. Patra, P. Bollam, A. Nanda, Long-term Outcome of Nonfunctioning and Hormonal Active Pituitary Adenoma after Gamma Knife Radiosurgery, vol. 114 (World Neurosurgery, 2018), pp. e 824–e 83210.1016/j.wneu.2018.03.09429574220 · doi ↗ · pubmed ↗