The silent spread of Hepatitis E in India - from epidemiological insight to public health action: a comprehensive review
Snigdha Maity, Shivam Chowdhary, Akila Swaminathan, Nidhi Ashtaputre, Piya Paul Mudgal, Chiranjay Mukhopadhyay

TL;DR
Hepatitis E is a growing public health problem in India, spreading through contaminated water and affecting vulnerable groups, requiring better surveillance and policies.
Contribution
This review highlights the epidemiological complexity and public health challenges of Hepatitis E in India, emphasizing the need for integrated interventions.
Findings
Hepatitis E is the leading cause of acute viral hepatitis in India, primarily transmitted through contaminated water.
High-risk groups like pregnant women and immunocompromised individuals face severe outcomes from HEV infection.
A lack of an approved vaccine and limited public awareness hinder effective prevention and control of HEV in India.
Abstract
Hepatitis E represents an increasingly significant yet often overlooked public health issue in India, contributing substantially to both sporadic hepatitis cases and widespread waterborne outbreaks. Hepatitis E virus (HEV) is the foremost cause of acute viral hepatitis (AVH) in India and spreads primarily through contaminated water. Genotype-specific differences in transmission routes, ranging from enteric routes in developing regions to zoonotic routes in industrialized settings, underscore the complexity of its epidemiology. Vulnerable populations such as pregnant women, animal handlers, and immunocompromised individuals face a markedly increased risk of severe disease outcomes, including fulminant hepatic failure and chronic infection, in cases of coinfection with hepatitis B virus. This comprehensive review delves into Indian epidemiological trends, clinical features, diagnostic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
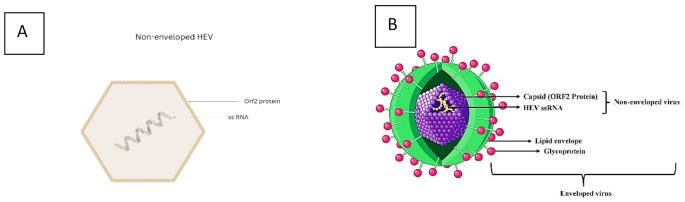 Figure 1
Figure 1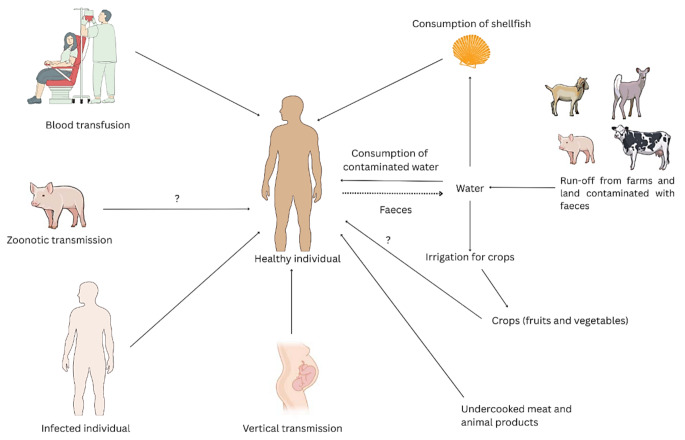 Figure 2
Figure 2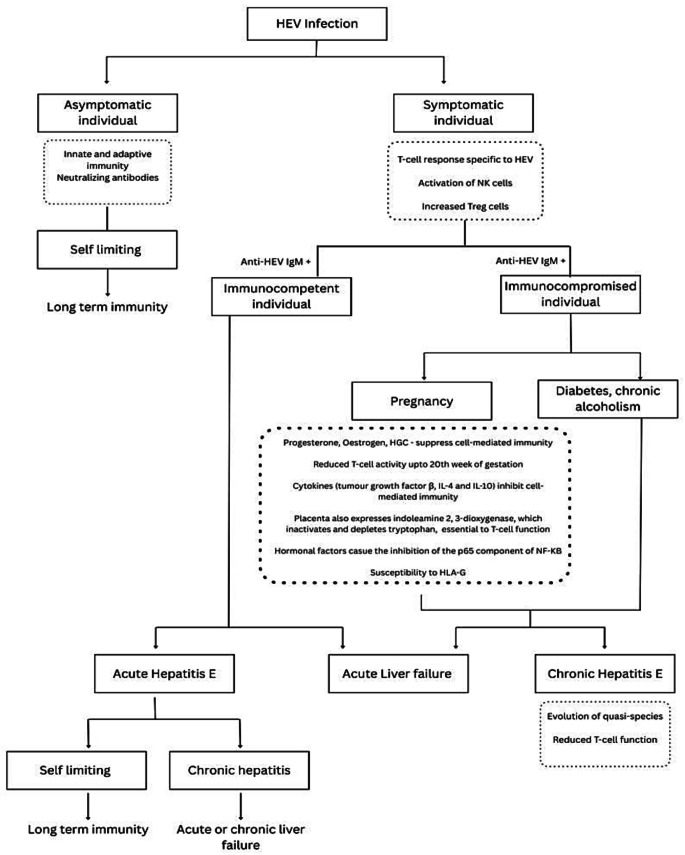 Figure 3
Figure 3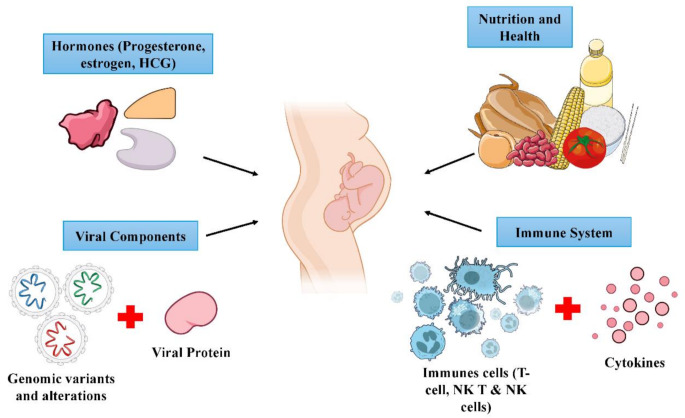 Figure 4
Figure 4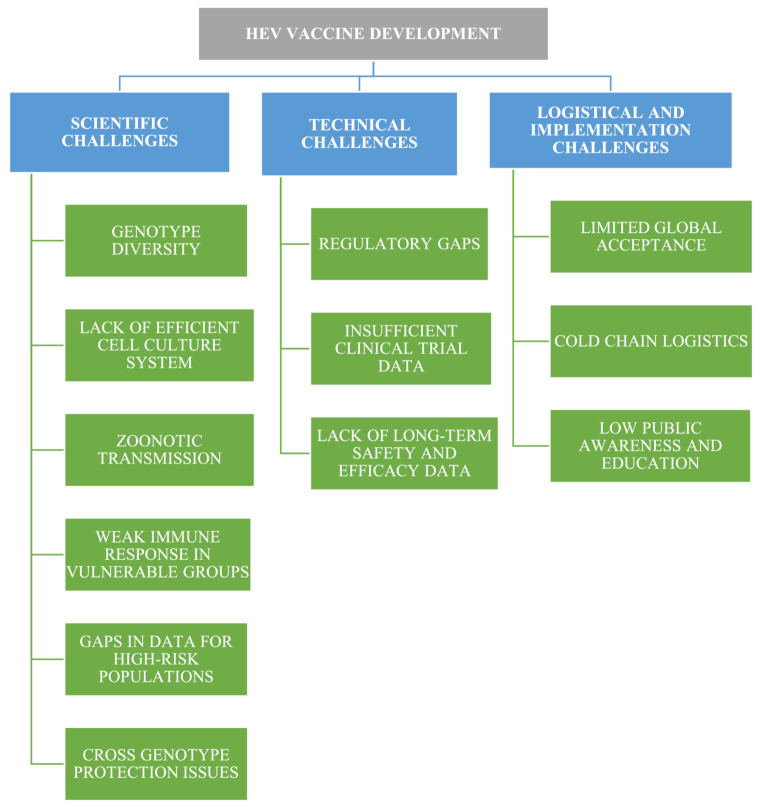 Figure 5
Figure 5- —Manipal Academy of Higher Education, Manipal
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatitis Viruses Studies and Epidemiology · Hepatitis B Virus Studies · Viral gastroenteritis research and epidemiology
Introduction
Hepatitis E virus (HEV) has been increasingly identified as a zoonotic pathogen of concern and is considered the leading cause of AVH, a condition characterized by hepatic inflammation and damage, typically resolving within 4 to 6 weeks [1]. Although self-limiting, HEV can cause chronic hepatitis, fibrosis, cirrhosis, and may contribute to the development of hepatocellular carcinoma in immunocompromised individuals, impacting morbidity. It disrupts liver function, causing jaundice and, rarely, fulminant hepatitis, leading to liver failure. HEV accounts for an estimated 20 million annual infections globally, underscoring its significant public health burden [2, 3]. Notably, HEV infection contributes to substantial mortality and morbidity worldwide, especially among pregnant women, who face a heightened risk of severe complications [4]. The evolving spectrum of clinical presentations and epidemiology highlights the serious global health impact of HEV, necessitating further research into its pathophysiology [5].
Hepatitis E virome
HEV is a non-enveloped virus with an icosahedral capsid (27–34 nm) carrying single-stranded, positive-sense RNA (Figure 1). The Hepeviridae family, Orthohepevirus genus [3], was initially recognized as non-A, non-B hepatitis. HEV is transmitted primarily through the enteric route in countries with poor sanitation and unhygienic conditions [4]. Since HEV is excreted in feces, it is capable of surviving outside the host for long periods. In blood and culture supernatants, HEV virions are quasi-enveloped by acquiring a host-derived lipid membrane via the exosomal pathway. When the virus buds into multivesicular bodies, the ORF3 protein assists its release by exocytosis. The envelope assists the virus in evading neutralizing antibodies and escaping the host’s immune system. The envelope is lost as the virions pass through the biliary tract. Hence, in the feces, non-enveloped viral particles are shed and are infectious [6]. Furthermore, the emergence of zoonotic transmission, with genotypes 3 and 4, expands the transmission pathways beyond traditional enteric routes, adding complexity to its epidemiology.
Fig. 1. The dual structure of HEV. HEV exists in two forms depending on its environment. A. Non-enveloped HEV consists of a naked capsid protein (ORF2) that encloses ssRNA genome. These virions are shed in the feces, which are stable outside the body and optimized for fecal-oral transmission. B. Enveloped HEV, also known as quasi-enveloped HEV, is formed in the bloodstream and infected hepatocytes of the host. It consists of capsid protein and ssRNA genome surrounded by host-derived lipid envelope. This envelope masks viral antigens, facilitating immune evasion and persistence within the host.Adapted from Servier (10/8/2024). Enveloped Virus. Smart Servier Medical Art Source. Available from https://smart.servier.com/smart_image/smart-hepatitis-virus/
Tracing the spread: the epidemiology of hepatitis E
Global pathways of HEVs
HEV represents a considerable global health challenge, with annual estimates indicating 2 million infections, 3.3 million symptomatic cases, and over 70,000 fatalities [7, 8]. Approximately 33% of the global population, exceeding 2 billion individuals, resides in HEV-endemic regions [9]. The virus was first identified during a significant outbreak in Kashmir Valley, India, in 1978, causing 52,000 cases and 17,000 fatalities [10]. HEV is endemic across Asia, the Middle East, Central America, and Africa, with India demonstrating high endemicity [1]. In India, Genotype 1 (GT1) HEV, which primarily infects humans, dominates epidemics and sporadic outbreaks [1, 11]. While GT3 and GT4 HEVs circulate among wild mammals, animal-to-human transmission is rare [12]. Globally, GT3 is common in Europe; GT4 is common in China, Korea, and Japan; and GT2 is common in West Africa and Mexico, whereas GT1 is widespread in Asia and Africa [13, 14]. Zoonotic transmission, primarily via porcine reservoirs and consumption of undercooked pork, is common in developed countries [1]. Initially, HEV transmission in developing nations occurred through fecal-contaminated water [15]. Despite improved sanitation, HEV remains prevalent in resource-limited regions lacking clean water. Seroprevalence data on anti-HEV IgG (immunoglobulin G) indicate that approximately 12.47% of the global population has experienced HEV in the past, with Asia (21.76%) and Africa (15.80%) exhibiting the highest rates. Globally, an estimated 110 million individuals have anti-HEV IgM (Immunoglobulin M) and 15 million have detectable HEV RNA [9]. However, underdiagnosis and underreporting in developing countries suggest that the true burden is significantly greater than current estimates [16]. Other HEV GT5 and GT6 have been isolated from wild boars in Japan, but no human infections have been documented. However, the virus can be transmitted to Cynomolgus macaques in laboratory settings, which indicates a potential risk for the transmission from animals to humans. At least one immunocompromised person developed chronic hepatitis E from GT7 after ingesting camel milk and meat in the Middle East, where dromedary camels were found infected. GT8, which is found in Bactrian camels in China, can infect monkeys but not typically humans [17–19].
Mapping HEV: prevalence across the Indian subcontinent
Hepatitis E, a significant cause of AVH in India, is characterized by numerous regional outbreaks. The 1991 Kanpur epidemic, which affected more than 79,000 people, was among the largest, with higher attack rates in adult males [20]. Subsequently, between 2011 and 2013, India’s Integrated Disease Surveillance Programme (IDSP) documented 78 HEV outbreaks and 22,671 cases with 152 deaths from 2013 to 2018 [21]. An HEV genotype 1a outbreak in Raipur (2014), linked to sewage-contaminated water, recorded a 68.8% attack rate, resulting in 23 deaths, including 8 pregnant women [22]. The first major HEV epidemic occurred in Delhi during 1955–1956, and subsequently, retrospective investigations identified the etiological agent as HEV. The outbreak involved more than 29,000 cases of jaundice due to an overflow of sewage-contaminated water from the Yamuna River during monsoon rains. Approximately 266 deaths were recorded with a higher prevalence among pregnant women. The 1978–1979 Kashmir epidemic (November to April) occurred in over 200 villages of the Gulmarg area and affected an estimated population of 600,000. The outbreak resulted in 20,083 cases due to contaminated water supplies. The high mortality rates (20 –30%) among pregnant women supported that HEV is a distinct disease. Subsequently, from 2015 to 2017, Kashmir reported 10 outbreaks with 393 cases [13, 14]. These outbreaks consistently involve fecal contamination of drinking water, confirmed by anti-HEV IgM positivity [10], highlighting waterborne transmission in India. However, our understanding of HEV transmission has evolved. A study in the Amritsar region revealed that HEV was the leading cause of waterborne hepatitis, peaking in the 21–30 years age group [16]. Furthermore, socioeconomic factors, particularly poverty and poor sanitation, are correlated with increased HEV incidence. Vertical transmission to newborns has been reported, although it is self-limiting. Seroprevalence studies among blood donors and patients have revealed widespread anti-HEV IgG and IgM positivity, indicating past, active, and subclinical infections. Coinfection with HBV has also been reported [23–26].
HEV’s evolving landscape: 2015–2024
HEV is a globally recognized enteric pathogen, with diverse transmission routes, including zoonotic, parenteral, and vertical [5]. A systematic review (1987–2023) of Southeast Asia revealed increasing anti-HEV IgG and IgM prevalence. The pooled IgG prevalence was 21.03%, with the highest in Myanmar (33.46%) and the lowest in Malaysia (5.93%). IgM was highest in Indonesia (12.43%) and lowest in Malaysia (0.91%), underscoring the need for targeted public health interventions [7].
Global Burden of Disease data (1990–2019) show a global decline in HEV incidence; however, high-incidence regions such as sub-Saharan Africa, Oceania, South Asia, and Central Asia bear the greatest burden [7]. A 2024 outbreak in Chad, with more than 2000 suspected cases and 0.3% case fatality, demonstrated persistent vulnerability among displaced populations, highlighting sanitation and hygiene needs [8]. Disparities in healthcare access and sanitation remain prevalent, particularly in low- and middle-income countries. Concurrently, affluent countries, notably Europe, have seen rising native cases linked to GT3 from undercooked pork [9].
The evolution of hepatitis E from an overlooked tropical disease to a global concern is marked by an increase in chronic infections, particularly among immunocompromised patients [1]. The WHO emphasizes vaccination and better sanitation to curb HEV, but broader efforts are needed. A meta-analysis revealed that country, testing method, and age distribution influence HEV IgG incidence in nonendemic regions [12]. Despite a highly efficacious recombinant vaccine, Hecolin, being approved in 2011 for use in China, global vaccination remains largely unimplemented [11]. Effective combat requires specialized public health approaches, enhanced diagnostics, and equitable healthcare access, as the true burden is underestimated [5].
HEV causes 30–70% of acute sporadic hepatitis cases and large outbreaks, primarily in low- and middle-income countries. Outbreaks involving HEV types 1 and 2 are linked to inadequate sanitation, fecal contaminated water, population displacement, low socioeconomic conditions, and natural disasters such as floods. In contrast, rare sporadic cases in developed nations are mainly due to zoonotic HEV genotype 3, acquired from the consumption of undercooked meat, particularly pork [3, 13, 14].
Urban vs. rural: how environments shape transmission
HEV transmission, primarily via the fecal‒oral route, is influenced by water quality, sanitation, hygiene, and food practices (Figure 2) and varies between rural and urban settings. Rural areas often face greater challenges [12], as floods, contaminated water sources, inadequate sanitation, and poor hygiene increase infection risk [13, 14]. Additionally, agricultural practices involving close contact and handling of infected livestock, especially pigs, can contribute to zoonotic transmission in rural populations [15]. A lack of awareness, poor socioeconomic status, and limited healthcare access in rural areas delay diagnosis and treatment [16].
High population density and rapid urbanization in cities favour HEV spread, as overcrowding and poor sanitation accelerate transmission [13, 14, 20]. Migration to urban areas and informal settlements further elevates risk. Despite better infrastructure, transmission continues due to poor hygiene, contaminated water, and inadequate sewage [27]. Although less frequent, zoonotic transmission from shellfish and contaminated animal products remains a risk [15]. Extreme weather, such as droughts and floods, can worsen water scarcity, leading to compromised hygiene and increasing HEV transmission [12].
Fig. 2. Transmission routes of HEV. HEV is transmitted via contaminated water, feces, and shellfish; zoonotic transmission is also seen after direct contact with animals and consumption of undercooked meat. Although less frequent, HEV is also transmitted vertically and through blood transfusions [28]. Diagram created in Canva. Icons and illustrations sourced from Canva’s content library and adapted from NIAID Visual & Medical Arts. (8/10/2024)
The dual faces of HEVs: endemicity explained
Hepatitis E virus presents two distinct epidemiological patterns on the basis of its four genotypes (Table 1). In developing countries, genotypes 1 and 2 are widely prevalent; they spread via the fecal‒oral route and cause acute outbreaks, mainly in young adults and pregnant women, whereas chronic cases are rare [29]. In contrast, genotypes 3 and 4 in developed countries cause sporadic zoonotic infections, which sometimes progress to chronic disease in older and immunocompromised individuals [13–16].
Table 1. Two distinct epidemiological patterns of hepatitis ECHARACTERISTICHIGH ENDEMICITYLOW ENDEMICITYGeographical locationDeveloping countries- South/Central Asia,* Africa*,* Central America* Developed countries- North and South America,* Europe*,* Australia*,* East Asia*,* South Africa*HEV Genotypes 1 and 2
3 and 4 Transmission RouteFecal-oral,* contaminated waterZoonotic*,* blood transfusionAffected PopulationYoung adults*,* pregnant womenElderly*,* immunocompromised*Chronic Infection Rare
Common in immunocompromised
Hepatitis E: recognizing the signs & complications
Acute hepatitis E
HEV infection is often mild or asymptomatic, with a 2–10-week incubation period [29]. Symptomatic cases begin with a prodromal phase marked by low-grade fever, fatigue, nausea, vomiting, and anorexia, followed by signs of acute hepatitis, including dark urine, pale stools, myalgia, abdominal pain, itching, hepatomegaly, and jaundice [4]. The levels of liver transaminases, bilirubin, alkaline phosphatase, and γ-glutamyl transferase are often elevated. Although alanine aminotransferase (ALT) levels in typical HEV patients can reach ~ 1500 IU/L, some patients may present minimal or normal levels despite active viremia. Jaundice occurs in approximately 40% of acute cases. In immunocompetent individuals, infection usually resolves spontaneously with rest and supportive care within weeks [30, 31].
Severe complications such as acute liver failure (ALF) or fulminant hepatitis can rarely occur, especially in pregnant women and those with preexisting liver conditions. ALF involves rapid loss of liver function within eight weeks of symptom onset and is characterized by coagulopathy (International Normalized Ratio ≥ 1.5) and encephalopathy without preexisting cirrhosis [32]. ALF is characterized by jaundice, encephalopathy, severe liver injury, bleeding, and increased risk of death, necessitating close monitoring and, in some cases, emergency liver transplantation [32].
Chronic hepatitis E
Chronic Hepatitis E, characterized by symptoms persisting beyond 6 months, primarily affects immunocompromised individuals such as transplant recipients, patients on immunosuppressants, and those with pre-existing liver disease. HIV–HEV coinfected individuals, pregnant women, and cancer patients on chemotherapy are also at increased risk for severe complications and extrahepatic manifestations [8, 9]. Clinical features include elevated transaminase levels, progressive liver damage, cirrhosis, and possible mortality [33]. Extrahepatic complications include pancreatitis; neurological disorders such as Guillain–Barré syndrome; myelitis; encephalitis; neural amyotrophy; hematological abnormalities; renal injury [33]; and cryoglobulinemia and rheumatologic manifestations [27]. The diagnosis of chronic HEV requires a persistently positive reverse transcriptase polymerase chain reaction test for HEV RNA in serum or stool samples obtained at least three to six months after the initial diagnosis [9].
Extrahepatic
These include neurological, renal, and rheumatological complications. The neurological issues most commonly include pyramidal signs, ataxia, myopathy, encephalitis, cognitive impairment, and various neuropathies. Renal complications, including glomerulonephritis, IgA nephropathy relapses, and nephrotic syndrome, have been reported, especially in transplant recipients. Rheumatological manifestations, including arthralgia, myalgia, dermatological rashes, and cryoglobulinemia, are primarily associated with chronic infection [33]. Figure 3 illustrates the clinical features and immune response of HEV.
Fig. 3. Clinical manifestations and immune response in HEV infection. Created via Canva elements
HEV in pregnancy: a critical concern
HEV infection during gestation, especially in the third trimester, is linked to high maternal and fetal mortality, with case fatality rates reaching 20–25% [33]. GT1 infections are associated with greater disease severity, including complications such as ALF and fulminant hepatitis, especially in the second and third trimesters. Vertical transmission may lead to adverse outcomes such as miscarriage, stillbirth, premature delivery, postpartum haemorrhage, and both neonatal and maternal mortality [24]. The underlying mechanisms of severe liver injury in pregnancy remain unclear, but hormonal and immunological alterations, combined with HEV genome variability, are implicated [1] (Figure 4). In contrast, breastfeeding is generally considered safe in the absence of active symptomatic infection [34].
Fig. 4. Mechanisms underlying HEV-induced severe liver injury in pregnancy [24, 34]. Image adapted from Servier Medical Art (https://smart.servier.com/), licensed under CC BY 4.0 (https://creativecommons.org/licenses/by/4.0/) and NIAID Visual & Medical Arts. (10.8.2024)
Illuminating insights (via biomarkers)
To assist in diagnosing hepatitis E and understanding its progression, various biomarkers have been identified, including those in plasma, urine, and microRNA (miRNA) profiles, reflecting the host’s response to HEV.
Plasma and urine biomarkers
Taneja et al. identified plasma transthyretin and urinary α1-microglobulin as potential biomarkers for acute hepatitis E. Preliminary data also suggest that urinary zinc alpha glycoprotein levels are lower in fulminant patients than in acute HEV patients, but these findings require further validation. Five potential peptide peaks were further identified through mass spectrometry, indicating strong diagnostic potential for differentiating hepatitis E patients from healthy controls [35].
MicroRNA signature biomarkers
Costafreda et al. reported that certain miRNA signatures, including the upregulation of miR-122 and miR-194 in acute hepatitis E patients and the downregulation of miR-125b-5p and miR-192-5p in chronic hepatitis E patients, could serve as biomarkers [36]. While these biomarkers show promise for improving hepatitis E diagnosis, the variability in HEV outcomes necessitates further research to validate findings and identify additional markers.
Optimizing biomarker profiles for sporadic HEVs
A study of 271 sporadic acute hepatitis cases revealed 91 confirmed HEV infections on the basis of RNA, IgM, or significant increases in IgG. It revealed frequent false negatives with individual markers, emphasizing the need for a combined diagnostic approach using HEV RNA, IgM, and rising IgG, especially in regions with variable endemicity and reinfection rates [37].
Interleukin-18 (IL-18) as an indicator of HEV exposure and transfusion risk
A cross-sectional study of Mexican blood donors revealed 9.4% HEV seropositivity and detected HEV RNA in one pooled seropositive sample, highlighting the risk of transfusion-related transmission. Elevated IL-18 and interferon gamma (IFN-γ) levels are associated with HEV seropositivity, suggesting that IL-18 is a potential biomarker of HEV exposure, which is consistent with profiles observed in acute cases [38].
HEV: a challenging diagnosis
Early HEV diagnostic methods, such as electron microscopy, fluorescent antibody assays, and antigen detection, are labor-intensive and complex, limiting their clinical use. Cloning of the HEV genome later enabled significant advances in molecular and serological diagnostics [35]. The European Association for the Study of the Liver guidelines recommend including HEVs in the differential diagnosis for viral hepatitis and drug-induced liver injury, especially during chronic liver disease flares or in immunocompromised patients and transfusion recipients with abnormal LFTs (liver function tests) [39].
Clinically, HEV is indistinguishable from other AVHs requiring serological confirmation. Diagnosis is typically considered during outbreaks, suspected water contamination, severe hepatitis during pregnancy, or when hepatitis A is excluded. Serum anti-HEV IgM confirms recent infection and lasts 3–4 months, sometimes up to a year [40]. Anti-HEV IgG antibodies, while long-lasting, suggest past exposure, with variable persistence [41]. However, a diminished antibody response in immunocompromised patients makes serology unreliable [40].
Molecular testing, such as HEV RNA detection in conjunction with IgM antibody detection, is crucial for confirming an acute or chronic active infection. RNA appears ~ 3 weeks post-exposure, with fecal shedding lasting 4–6 weeks [36, 41]. In acute HEV, the serum bilirubin level typically exceeds 2.5 mg/dL, and ALT level increases over tenfold (29–33 U/L in men, 19–25 U/L in women) [42]. The diagnosis of HEV in immunocompetent individuals should combine serology and molecular methods, while PCR is critical for immunocompromised patients and for identifying chronic HEV, defined by HEV RNA persistence for over 3 months [13, 14]. In low-resource settings, epidemiological evidence may support diagnosis [13]. The World Health Organization (WHO) has set nucleic acid amplification test-based standards for blood and plasma safety [43]. The Indian Council of Medical Research-National Institute of Virology has developed enzyme-linked immunosorbent assays (ELISAs), PCR assays, and rapid strip tests for waterborne HEVs to aid diagnosis in resource-limited areas [44].
Point-of-care diagnostics: bringing the lab to the patient
Currently, no Food and Drug Administration (FDA)-approved point-of-care test (POC) exists for HEV [37]. However, significant progress has been made with CRISPR-Cas13a (clustered regularly interspaced short palindromic repeats - CRISPR-associated proteins) systems, lateral flow assays, and molecular POC tests, which offer high sensitivity, specificity, and rapid results and are especially valuable in resource-limited settings [45, 46]. Ying et al. developed a fluorescent microbead-based immunoassay (FMIA) for rapid point-of-care HEV antigen detection, which demonstrated high sensitivity (92%) and specificity (100%). This FMIA correlated well with HEV RNA levels and commercial assays, proving valuable for the rapid and simple diagnosis of acute HEV in developing and rural settings [47]. Li et al. developed a rapid HEV RNA diagnostic method using reverse-transcription recombinase polymerase amplification (RT-RPA) combined with a lateral flow strip. The assay showed high sensitivity (detection limit: 1.0 × 10² copies/mL) and specificity, with no cross-reactivity to other hepatitis viruses, and effectively detected HEV GTs 3 and 4 [48, 49]. CRISPR-Cas13a-based systems have shown great promise for HEV RNA detection, with high sensitivity and specificity. Detection limits reach 12.5 IU/mL for fluorescence assays and 200 IU/mL for strip formats, identifying HEV genotypes 1–4 without cross-reactivity [50]. Advanced lateral flow assays, such as reverse transcription recombinase-aided amplification with lateral flow dipstick (RT-RAA-LFD) and quantitative real-time reverse transcription recombinase-aided amplification (qRT-RAA), enable rapid HEV RNA detection with high sensitivity and specificity. RT-RAA-LFD is complete in 15 min at 39 °C (limit of detection (LOD): 247 copies/µL), whereas qRT-RAA is completed in 20 min at 42 °C (LOD: 25 copies/µL), making it a valuable tool for rapid screening, including in veterinary settings [51].
Treatment roadmaps
Effective management of hepatitis E requires a tailored approach on the basis of disease severity, patient risk factors, and immune status. While most acute cases are self-limiting and require supportive care, specific antiviral therapies are considered for chronic infections and high-risk groups. Table 2 summarizes current and emerging HEV treatment strategies.
Table 2. Summary of current therapeutic interventions for HEVTreatment CategoryApproach/DrugMechanism of Action/UseClinical Notes/LimitationsReferenceSupportive care (Acute Hepatitis E)Ursodeoxycholic acid & CholestyramineSymptomatic management- used to manage symptoms like jaundice, pruritus, and fatigue.Most acute HEV cases are self-limiting; no antiviral therapy is needed, monitor LFTs and bilirubin for progression.[52]Antiviral Therapy (Chronic Hepatitis E)RibavirinInhibits viral RNA synthesis. Normalizes liver enzymes and reduces viral load in chronic cases.First-line therapy (approx. 3 months) with optimal dose of 1.8–2.3 mg/L for Solid Organ Transplant (SOT) recipients; contraindicated in pregnancy due to teratogenicity; EASL advises use only if immunosuppression reduction fails.[53]Pegylated Interferon -αAn immunomodulator used in liver transplant or HIV patients with chronic HEV.Risk of organ rejection in SOT patients; not universally recommended due to adverse effects in pregnant women and limited efficiency data.[54]Sofosbuvir (± Ribavirin)Inhibits Non-structural protein 5B viral RNA polymerase; in combination with ribavirin, may partially clear the virus in chronic HEV.Ineffective as monotherapy but shows potential in HEV genotype 3 during pregnancy; clinical value under review, and optimal dosage yet to be established.[55]Zinc sulfate & zinc oxide (ZnSO₄, ZnO)Inhibits HEV replication by targeting RNA polymerase, with virucidal activity, especially in GT1 and 3.Demonstrated efficacy *in vitro.*Good enteric absorption and bioavailability with ZnO nanoparticles. [56]Investigational & Repurposed DrugsIfenprodilN-methyl-D-aspartate receptor antagonist; reduces HEV RNA accumulation and viral protein expression.Effective in liver-derived cells and in vivo models; under investigation.[57]Vidofludimus calcium, PyrazofurinVidofludimus calcium: dihydroorotate dehydrogenase inhibitor. Pyrazofurin: targets uridine monophosphate synthetase.Both inhibit pyrimidine synthesis enzymes, leading to disruption of HEV RNA synthesis.Potential for treating chronic infections; Identified via drug repurposing, promising antiviral activity in preclinical settings.[58]MethotrexateAn anti-inflammatory drug that inhibits HEV helicase, essential for RNA processing and replication.Novel antiviral target for HEV; early-phase data suggest efficacy.[59]NITD008 & GPC-N114Broad-spectrum antivirals showing inhibition of HEV replication; synergistic in combination.Promising results in vitro, particularly against genotype 1, identified via drug repurposing; further validation needed.[60]Management of Severe ComplicationsLiver Support Devices, Liver TransplantationProvide temporary hepatic function support for severe HEV cases progressing to ALF.Transplantation is critical when liver failure is irreversible, requires extensive postoperative care; life-saving option.[61]
Safeguarding tomorrow
Preventing HEV transmission in endemic regions requires enhanced sanitation, hygiene, and clean drinking water. Cooking meat above 70 °C reduces zoonotic transmission risk [20]. Fecal-oral transmission is curbed via a safe water supply, proper waste disposal, and food hygiene education [3]. Vaccine development targeting the ORF2 capsid protein has advanced, with a 56-kDa recombinant vaccine showing high efficacy in a phase II trial in Nepal, though tested in males [62]. Hecolin^®^, a 26-kDa truncated ORF2 protein vaccine produced by Xiamen Innovax Biotech Co., Ltd., in China, is the only licensed hepatitis E vaccine [63]. Approved by the China FDA in 2012, Hecolin^®^ is available for individuals over 16, especially high-risk individuals. Despite demonstrating 96% efficacy in a phase III trial, its use remains restricted to China, with the WHO calling for further phase IV studies in vulnerable populations [63]. A phase IV study in Bangladesh is evaluating Hecolin’s efficacy and safety in women of reproductive age, including pregnant women, where it has shown potential [64]. Further studies are needed to address existing concerns and facilitate the global acceptance of Hecolin^®^, alongside research on novel HEV vaccine candidates [63].
Hurdles on the horizon: challenges in HEV vaccine development
The development of an effective hepatitis E vaccine faces key challenges due to the complex biology, diverse genotypes, and varied immune responses of the virus (Fig. 5) [65]. A major barrier is the lack of a robust cell culture system, hindering large-scale vaccine production [62, 66]. Current vaccines, such as Hecolin^®^, primarily target GT1 and offer limited protection against GT3, necessitating broader cross-genotype coverage.
The limited global availability of Hecolin^®^ underscores the need for more trials in diverse high-risk groups and solutions to logistical challenges in endemic areas. Despite two months at 30–37 °C, it still requires cold-chain storage (2–8 °C). Prefilled syringes aid dosing and reduce contamination, but complicate transport, storage, and waste management [62]. Additionally, infrastructure limitations, cost, and insufficient awareness impede vaccine integration into routine immunization schedules, especially in low- and middle-income countries [67]. Therefore, broader genotype coverage, more data in high-risk groups, and improved access are crucial for effective global HEV prevention [68].
Fig. 5. Challenges in hepatitis E vaccine development
On trial: promising HEV vaccine candidates
The development of investigational HEV vaccines has advanced considerably, with several candidates in clinical trials. Recombinant vaccines using ORF2-based virus-like particles (VLPs) have shown promise, stimulating neutralizing antibodies [69]. Four VLP candidates have demonstrated safety and immunogenicity, particularly against GTs 1 and 4 (Table 3).
Table 3. List of HEV candidate vaccines and commercialized vaccinesVACCINEMANUFACTURERANTIGENEXPRESSION SYSTEMDOSEEFFICACYDEVELOPMENT STATUSREFERENCE(Recombinant Hepatitis E Virus) rHEVGlaxoSmithKlineHEV-1ORF-2 (*aa 112–607) Baculovirus 0,1,6 months>99%Phase II[70]HEV 239(Hecolin^®^)Xiamen Innovax BiotechHEV-1ORF-2(aa 368–606) Escherichia coli 0,1,6 months95.5%LicencedPhase IV[71, 72]Lipo-NE-PZydus Lifesciences Ltd.HEV-1ORF-2 (aa 458–607) Escherichia coli 0,1,6 months-Phase II[73]HEV P179Changchun Institute of Biological Products Co. Ltd.HEV-4ORF-2 (aa 439–617) Escherichia coli 0,1,6 months-Phase Ib[74]*aa- amino acid
Combined vaccines
Dong et al. developed a combined hepatitis A and E vaccine containing inactivated HAV and recombinant HEV components. In mice, it induced neutralizing antibodies against both viruses, indicating dual protective potential [75]. Gao et al. developed a mucosal vaccine combining HAV and HEV proteins linked to tuftsin. Intranasal delivery increased IgG and IgA levels in the intestines, vagina, and lungs; increased IFN-γ levels and CD4⁺/CD8⁺ T-cell ratio, outperforming intramuscular injection. These findings support the use of HE-ORF2, HA-viral capsid protein 1, and tuftsin for improved immunogenicity in a combined hepatitis A and E vaccine [76].
Bivalent vaccines
Li et al. developed a potential bivalent vaccine by linking an HEV capsid protein segment (aa 551–607) to hepatitis B surface antigen (HBsAg) with a synthetic glycine linker. Expressing this fusion protein in Pichia pastoris resulted in high immunoreactivity of the chimeric VLPs, indicating strong potential as a dual vaccine candidate against both HBV (Hepatitis B virus) and HEV [77]. Wang et al. developed a bivalent vaccine targeting norovirus (NoV) and HEV by covalently linking their dimeric P domains with dimeric glutathione-S-transferase (GST). Immunization of mice with GST-NoV P–HEV P and NoV P–HEV P complexes significantly increased antibody titres, supporting their potential as dual vaccine candidates [78]. Another study utilized a recombinant fusion protein that combines a truncated HEV ORF2 (amino acids 112–607) with rotavirus (RV) NSP4, which is expressed via a baculovirus system, suggesting another promising multivalent vaccine [79].
Trivalent subunit vaccines
A recent study developed a trivalent subunit vaccine targeting HEV, rotavirus, and astrovirus (AstV). Two formats were tested: a “fused vaccine” combining spike protein antigens into one molecule and a “mixed vaccine” of individual antigens. Both were efficiently produced in E. coli. Mouse studies have shown that the fused vaccine elicits higher antibody titres and stronger neutralizing activity against HEV, alongside improved blocking of RV receptor binding. These findings highlight the use of the fused vaccine as a promising candidate for simultaneous protection against HEV, RV, and AstV [80].
Multiple epitope peptide vaccines
Computationally designed multiepitope peptide vaccines show promise in preclinical models, inducing humoral and cellular immunity. These constructs use validated HEV epitopes and adjuvants to enhance immune responses but require further laboratory validation [81].
Oral HEV vaccines
Recent studies have shown that oral delivery of recombinant HEV capsid proteins with immunobiotic bacterium-like particles induces strong systemic and mucosal immune responses in murine models, suggesting a needle-free HEV vaccination approach [82]. Research indicates that oral vaccines can effectively induce IgA and IgG responses, although optimal results may require combined oral and subcutaneous administration [83].
Another study evaluated the use of recombinant HEV virus-like particles (rHEV VLPs) for oral immunization. Even without a mucosal adjuvant, purified rHEV VLPs induced robust systemic (serum IgG, IgM, IgA) and mucosal (fecal IgA) responses in mice. These antibodies recognize the native HEV antigen, suggesting that rHEV VLPs are promising oral vaccine candidates [84]. Furthermore, a plant-based oral vaccine using genetically transformed tomato plants with a partial HEV ORF2 gene showed promise. Transgenic lines confirmed successful DNA integration, and the recombinant protein retained immunoactivity, highlighting transgenic tomatoes as a promising, low-cost platform for oral vaccination [85].
Future horizons: addressing challenges and paving new paths
Hepatitis E remains a significant yet underdiagnosed public health issue in India, stemming from limited awareness and a lack of routine screening. Addressing this requires strengthened surveillance, improved diagnostics, and effective vaccination strategies. Continued research is crucial to develop safer, broadly protective vaccine candidates and address safety concerns in vulnerable groups (e.g., pregnant women and chronic liver disease patients), ensuring broader global acceptance of vaccines such as Hecolin^®^ [5].
Preventive strategies should focus on basic hygiene, safe drinking water, and proper waste disposal, alongside HEV screening in blood banks, to reduce transfusion-related transmission. A ‘One Health’ approach is essential, promoting collaboration between the human and veterinary sectors to monitor animal reservoirs such as swine, camels, and wild boar, given the diverse transmission routes of HEVs, including fecal-oral, zoonotic, parenteral, and vertical. Further research into HEV molecular virology and pathogenesis is needed to identify new therapeutic targets and develop more effective treatments for both acute and chronic infections [4, 5].
Summing it up: insights and outlook
Hepatitis E remains a formidable and underestimated public health challenge in India. Its evolving spread, encompassing zoonotic, waterborne, and vertical routes, has placed human populations at heightened risk. The true burden often remains underestimated due to limited public awareness and a lack of standardized diagnostic methods.
To effectively curtail this disease, a multipronged approach is essential. This encompasses enhancing public awareness, facilitating early diagnosis, improving vaccination strategies, and implementing robust preventive measures. Such efforts must include strengthening surveillance systems, widespread improvements in water, sanitation, and hygiene infrastructure. Moreover, continued research into HEV pathogenesis and the development of efficacious vaccines and novel therapeutics are crucial for transforming hepatitis E control and safeguarding the public health of the nation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Girish V, Grant LM, Sharma B et al. Hepatitis E. [Updated 2025 Apr 6]. In: Stat Pearls. Treasure Island (FL): Stat Pearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK 532278/
- 2Zhu FC, Zhang J, Zhang XF, Zhou C, Wang ZZ, Huang SJ et al. Efficacy and safety of a recombinant hepatitis E vaccine in healthy adults: a large-scale, randomized, double-blind placebo-controlled, phase 3 trial. Lancet Lond Engl. 2010;376(9744):895–902.10.1016/S 0140-6736(10)61030-620728932 · doi ↗ · pubmed ↗
- 3Koyuncu A, Mapemba D, Ciglenecki I, Gurley ES, Azman AS. Setting a course for preventing hepatitis E in low and lower-middle-income countries: a systematic review of burden and risk factors. In Open Forum Infectious Diseases. 2021;8(6):ofab 178. US: Oxford University Press.10.1093/ofid/ofab 178PMC 818624834113684 · doi ↗ · pubmed ↗
- 4Virhuez-Mendoza M, Ishijima K, Tatemoto K et al. Recent hepatitis E virus infection in wild boars and other ungulates in Japan. Viruses. 2025;17(4):524. 10.3390/v 17040524. PMID: 40284967.10.3390/v 17040524 PMC 1203102840284967 · doi ↗ · pubmed ↗
- 5Santos-Silva S, Hemnani M, Lopez-Lopez P et al. A systematic review of hepatitis E virus detection in camels. Veterinary Sciences. 2023;10(5):323. 10.3390/vetsci 10050323. PMID: 37235406.10.3390/vetsci 10050323 PMC 1022240337235406 · doi ↗ · pubmed ↗
- 6Zhang W, Li S, Shu X et al. A cross-species transmission of a camel-derived genotype 8 hepatitis E virus to rabbits. Pathogens. 2021;10(11):1374. 10.3390/pathogens 10111374. PMID: 34832530.10.3390/pathogens 10111374 PMC 861870934832530 · doi ↗ · pubmed ↗
- 7Nasir M, Wu GY. HEV and HBV dual infection: a review. J Clin Transl Hepatol. 2020;8(3):313–321. 10.14218/JCTH.2020.00030. Epub 2020 Jul 3. PMID: 33083255; PMCID: PMC 7562801.10.14218/JCTH.2020.00030 PMC 756280133083255 · doi ↗ · pubmed ↗
- 8Treagus S, Wright C, Baker-Austin C, Longdon B, Lowther J. The foodborne transmission of hepatitis E virus to humans. Food Environ Virol. 2021;13(1):127–45.10.1007/s 12560-021-09461-5PMC 811628133738770 · doi ↗ · pubmed ↗