The vestibular outcomes in non-blast related traumatic brain injury and the role of severity, aetiology and gender: a scoping review
Kübra Bölükbaş, Laura Edwards, Olivia R. Phillips, Veronica Kennedy, Kathryn Fackrell

TL;DR
This review examines how non-blast traumatic brain injuries affect the vestibular system, focusing on outcomes like dizziness and balance issues.
Contribution
The study provides a comprehensive overview of vestibular outcomes in non-blast TBI, highlighting the need for standardized assessment methods.
Findings
Benign paroxysmal positional vertigo (BPPV) was found in 38% of studies.
Central processing disorders were observed despite normal peripheral vestibular function.
BPPV was more common in TBI caused by falls, but severity and gender showed inconsistent effects.
Abstract
Traumatic brain injury (TBI) can lead to various vestibular impairments. This review explored common vestibular outcomes associated with non-blast related TBI and examined possible differences in vestibular outcomes based on TBI severity, aetiology, and gender. A scoping review was conducted using an established methodological framework, which involved electronic and manual searches of databases and journals. Records published in English were included which focused on vestibular outcomes and assessments associated with non-blast related TBI in individuals 18 years and older. Out of a total of 19.200 records, 50 met the inclusion criteria. Data were collated and categorised based on the objectives of the research. Benign paroxysmal positional vertigo (BPPV) was found in 38% of 50 studies. Furthermore, despite normal peripheral vestibular function, central processing disorders such as…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
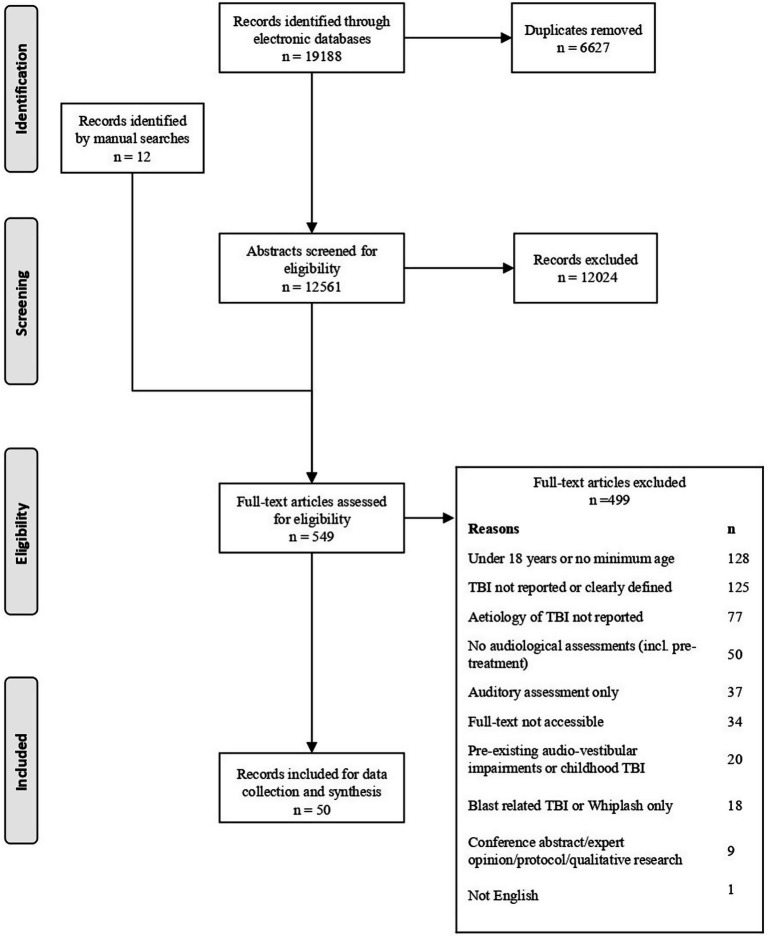 Figure 1
Figure 1| Ref | Country | Study design | Research aim | Sample size and age range (years) | Gender | Severity of TBI | Criteria of severity | Fall | MVA | Assault/direct impact | Sports injury | Other | Time of audiological assessment | Pre-TBI status |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Feneley and Murthy | UK | Case report | To describe the case who presented with acute bilateral deafness and vestibular dysfunction following occipital bone fracture | 1 (57 yrs) | M | NR | NR | ✓ | 3 dys (f/u: 3 wks) | Excellent health, with no meds or history of excessive alcohol consumption | ||||
| Bertholon et al. (2005) ( | France | Case report | To report cases who complained of positional vertigo shortly after head trauma | 1: Case 1 | M | NR | NR | ✓ | 1 mth | C1: No significant medical history | ||||
| Kagoya et al. (2010) ( | Japan | Case report | To present a very rare case of stapedial footplate fracture in which the superstructure with part of the footplate was dislocated and adhered to the tympanic membrane | 1 (25 yrs) | F | NR | NR | ✓ | 11 mths | Unremarkable medical history | ||||
| Ylikoski et al. (1982) ( | USA | Case report | To search for pathologic changes indicating nerve injury by examining the operative specimens of the eighth nerve from patients with post-traumatic dizz. and combining these findings with the clinical, otologic and surgical features of each case, to determine the site of primary lesion | 2: Cases 8, 9 (55, 53 yrs)* | M | C8: NR | NR | ✓ (2) | NR | NR | ||||
| Roup et al. | USA | Case report | To present a case report of a patient with a history of TBI, including self-perceived hearing difficulties and poorer-than-normal auditory processing performance | 1 (58 yrs) | F | Mild | NR | ✓ | 12 mths | No hearing or listening problems | ||||
| Jacobs et al. | USA | Case report | To present results of surgical repair in three patients with fistulas | 1: Case 1 (59 yrs)* | F | C1: NR | NR | ✓ | Subsequent mths | NR | ||||
| Herdman (1990) ( | USA | Case studies | Some common vestibular deficits that occur with a head injury will be illustrated, and the test results, exercise treatment, and course of recovery in those patients will be described | 3: Cases 1–3 (53, 39, 40 yrs) | M = 2 | NR | NR | ✓ (2) | ✓ | C1: 5 dys (f/u: 2 yrs) | NR | |||
| Jani et al. | USA | Case report | To report the usefulness of magnetic resonance imaging and auditory brainstem evoked responses in diagnosis | 1 (46 yrs) | F | Mod. or Severe | NR | ✓ | 13th dy | History of major mood disorder | ||||
| Fitzgerald (1995) ( | USA | Case report | To discuss the typical history and diagnostic tests for patients with perilymphatic fistula | 1: Case 1 (28 yrs)* | F | NR | NR | ✓ | 6 dys (f/u: 10 wks) | NR | ||||
| Lyos et al. | USA | Case report | To describe three patients with transverse temporal bone fracture who presented with residual auditory function only to develop profound SNHL | 3: Cases 1–3 (20, 20, 26 yrs) | M | NR | NR | ✓ | ✓ | ✓ | C1: 1 wk. | NR | ||
| Johnson | USA | Case report | NR | 1 (47 yrs) | F | Mild | NR | ✓ | 6 mths | NR | ||||
| Waninger et al. (2014) ( | USA | Case report | To describe a unique mechanism of ear barotrauma (intratympanic haemorrhage) and concussion caused by helmet-to-helmet contact in American football | 1 (26 yrs) | M | Concuss^ | NR | ✓ | 36 h | No history of prev. Concuss^ or head/ear injuries | ||||
| Blackard et al. (2020) ( | USA | Case report | NR | 1 (22 yrs) | F | Concuss^ | NR | ✓ | 5 dys (f/u: 1 mth) | No prior history of concuss^ | ||||
| Schuknecht and Davison | Canada | Case report | NR | 1: Case 3 (29 yrs)* | M | NR | NR | ✓ | 2 yrs | NR | ||||
| Paxman et al. (2018) ( | Canada | Case report | This case highlights the use of repetitive transcranial magnetic stimulation (rTMS) as a novel treatment option for patients who suffer from post-concussive symptoms and chronic dizz. Secondary to mTBI | 1 (61 yrs) | M | Mild | GCS: 15 | ✓ | NR | NR | ||||
| Ottaviano et al. (2009) ( | Italy | Case report | To report two cases of SNHL with BPPV and anosmia following traumatic head injury | 1: Case 2 (57 yrs)* | F | NR | NR | ✓ | 7 mths | NR | ||||
| Ralli et al. | Italy | Case report | The cases of suffering from vertigo after that fell from a camel during a visit to the middle east are described | 1: Case 1 (60 yrs)* | M | NR | NR | ✓ | 10 dys | NR | ||||
| Kanavati et al. (2016) ( | UK | Case report | NR | 1 (24 yrs) | M | NR | NR | ✓ | NR | NR | ||||
| Preber and | Sweden | Case report | NR | 4: Cases 1–3, 5 (36, 48, 57, 53 yrs)* | M = 2 | NR | NR | ✓ | ✓ (3) | C1: 1 mth (f/u: 1/2/4 mths) | NR | |||
| Tonkin and Fagan | Australia | Case report | The case histories of thirteen patients with such a fistula are described | 3: Cases 7, 9, 10 (20, 55, 26 yrs)* | M | NR | NR | ✓ (3) | C7: several wks | C9: Diabetic underwent a right below the-knee amputation | ||||
| Lerut et al. | Belgium | Case report | To discuss the case and the final diagnosis of carotico-cavernous fistula | 1 (68 yrs) | F | NR | NR | ✓ | 5 dys (f/u: 2 mths) | NR | ||||
| Fujimoto et al. (2007) ( | Japan | Case report | To report a rare and informative case of bilateral progressive SNHL after traumatic subarachnoid haemorrhage and brain contusion, in which cochlear implantation was very successful. | 1 (55 yrs) | M | NR | NR | ✓ | 1 mth (f/u: 23 mths) | No history of administration of ototoxic agents, including aminoglycosides | ||||
| Mohd Khairi et al. (2009) ( | Malaysia | Case report | To illustrate patients who sustained extradural haemorrhage following a motor vehicle accident with profound SNHL on the opposite ear | 1: Case 1 (31 yrs)* | M | NR | NR | ✓ | NR | NR | ||||
| Chung et al. | Korea | Case report | To present the case with bilateral otic capsule violating temporal bone fractures due to head trauma | 1 (44 yrs) | M | NR | NR | ✓ | 6 wks | NR | ||||
| Durbec et al. | France | Case report | NR | 1 (22 yrs) | M | NR | NR | ✓ | 8 dys | NR | ||||
| Sousa Menezes et al. | Portugal | Case report | To report the case of a patient with pneumolabyrinth, involving both the vestibule and the cochlea with intense vestibular symptoms, in whom the anatomic defect was evident on surgical exploration and successfully managed surgically | 1 (52 yrs) | M | NR | NR | ✓ | 3 dys | No relevant personal history | ||||
| Kleffelgaard et al. (2016) ( | Norway | Case series | (i) To describe a grp-based Vestibular Rehabilitation intervention for patients with TBI. (ii) To examine how the intervention may assist in addressing the targeted problems of dizz. and balance problems, by describing changes in self-perceived dizz., balance, and health-related quality-of-life (HRQL) | 4: Cases 1–4 (34, 25, 40, 45 yrs) | M = 2 | Mild | C1: GCS: 15 | ✓ (2) | ✓ | ✓ | C1: 18 mths | No severe psychological disease, cognitive dysfunction, other comorbidities affecting mobility and independent gain | ||
| Taylor et al. (2022) ( | New Zealand | Retrospective clinical case series | (i) determine how often, and which components of the peripheral vestibular system are affected. (ii) identify characteristics of the injury or clinical features that are associated with peripheral vestibular loss. (iii) explore the relationship between vestibular and oculomotor function and postural stability | 99 (18–80 yrs) | M = 40 | Mild (n95) | GCS and post-traumatic amnesia | ✓ | ✓ | ✓ | ✓ | ✓ | Mdn 12 mths | No pre-existing vestibular or neurological diagnoses, and severe visual or musculoskeletal impairment |
| Ouchterlony et al. (2016) ( | Canada | Case comparison interventional study | To determine the effectiveness of the canalith repositioning procedure in the treatment of BPPV among patients after mild-to-moderate traumatic brain injury | 21 BPPV | M = 34 F = 22 | Mild (n51) | GCS | ✓ (23) | ✓(23) | ✓ (3) | ✓ (5) | ✓ (2) | BPPV grp: mdn 50 ± 72.5 dys | No significant audio-vestibular signs and cerebrovascular disease |
| Teramoto et al. (2022) ( | USA | Retrospective study | To advance the science surrounding female head injury and investigate sex-based differences in concussion assessments among male and female varsity college athletes, strengthened by comprehensive longitudinal assessments following acute injury with baseline comparators | 111 | M = 59 | Concuss^ | NR | ✓ | Pre-session baseline | NR | ||||
| Ahn et al. (2011) ( | South | Retrospective study | To identify the clinical characteristics of BPPV after TBI and to determine whether clinical differences exist between BPPV after TBI and idiopathic BPPV. | 32 (30–74 yrs) | M = 18 | NR | NR | ✓ (8) | ✓ (20) | ✓ (4) | NR | No history of BPPV, migraine, brain tumour, or cerebrovascular, history of ear disease | ||
| Dlugaiczyk et al. (2011) ( | Germany | Retrospective study | To study the involvement of the different SSCs in post-traumatic BPPV with special reference to anterior canal | 1: Case 2 (57 yrs)* | M | NR | NR | ✓ | 3 wks | No serious illness, particularly no vertigo or any kind of inner ear disease | ||||
| Uyeno et al. (2024) ( | USA | Retrospective cohort study | To quantify norms and changes in eye-tracking proficiency, and determine vestibular symptom correlations in varsity college athletes following acute mTBI | 119 (18–24 yrs) | M = 63 | Mild | NR | ✓ | Pre-session baseline, | 66% sustained only 1 injury | ||||
| Hides et al. (2017) ( | Australia | Prospective cohort | To explore changes in sensorimotor function in the acute phase following sports concussion | 54 w/ Concuss^ | NR | Concuss^ | NR | ✓ | Pre-session baseline: | NR | ||||
| Joseph et al. (2021) ( | USA | Prospective cohort | To compare performance on the SOT vestibular score versus the Dual-Task test in individuals with and without subjective balance problems at least 1 yr. after a TBI | 26 Symptomatic TBI | M = 31 | Mild (n24) | Department of defence TBI rating scale ( | ✓ (18) | ✓ (16) | ✓ (16) | Symptomatic TBI: Avg. 584.5 dys | No major neurological, visual, or autonomic disorders | ||
| Motin et al. (2005) ( | Israel | Prospective study | To identify patients with BPPV among patients with severe TBI and to evaluate the effectiveness of the Particle Repositioning Manoeuvre | 20 (19–61 yrs) | M = 18 | Severe (n20) | NR | ✓ (6) | ✓ (4) | Mean 67 ± 14 dys | No vertigo any history of inner ear disease | |||
| Glendon et al. (2021) ( | UK | Prospective cohort | To explore if Vestibular-ocular-motor impairment corelates with longer Return to Play, symptom burden, neurocognitive performance and academic capability | 42 (18.2–25.2 yrs) | M = 25 | Concuss^ | NR | ✓ | Pre-session baseline: | NR | ||||
| Jafarzadeh et al. (2022) ( | Iran | Prospective cross-sectional study | The vestibular assessment of patients with persistent symptoms of mTBI by different vestibular tests | 21 (16–60 yrs) | M = 20 | Mild | Loss of consciousness <30 min., | ✓ | 118.2 ± 52.5 dys | No history of hearing loss, vertigo, imbalance or gait abnormality | ||||
| McCormick et al. (2023) ( | USA | Prospective cohort study | To investigate the incidence of BPPV specifically among patients with dizz. in the rehabilitation phase of concussion recovery and to provide evidence regarding the importance of BPPV assessment in physical therapy concussion evaluations | 50 (18–85 yrs) | M = 14 | Concuss^ | NR | ✓ (20) | ✓ (12) | ✓ (1) | ✓ (17) | Mean 32.68 dys | No cognitive impairment, severe arthritis, radiculopathies, or systemic conditions | |
| Galea et al. (2022) ( | Australia | Observational | (1) to identify whether adults 4 wks to 6 mths post mTBI have sensorimotor impairments compared with controls without mTBI. (2) to determine if sensorimotor impairments were evident irrespective of participant perceived absence of symptoms | 74 mTBI | M = 60 | Mild | NR | ✓ (17) | ✓ (10) | ✓ (9) | ✓ (38) | Avg. 72 dys | No neurological, psychiatric, visual, or vestibular impairments. No substance abuse or intracranial bleed | |
| Brown et al. (2022) ( | Australia | An exploratory study | (1) to compare the results of the VOMS in combat sport athletes with a healthy control population. (2) to explore differences between athletes with and without a concussion history. (3) to examine the relationship between VOMS and the Post-Concussion Symptom Scale in combat sport athletes | 40 (18 Concuss^) | M = 80 | Concuss^ | Self-defined: Concussion in Sport grp definition ( | ✓ | Mean 9.8 ± 9.4 wks | Competitive fight within last 2 yrs | ||||
| Honaker et al. (2015) ( | USA | Cross-sectional study | To describe the performance of the Gaze Stabilization Test in a cohort of collegiate football players and to examine the effects of previous concussion on outcome parameters of the Gaze Stabilization Test | 15 Concuss^ | M = 80 | Concuss^ | NR | ✓ | 3 mths–9 yrs | n15: prev. Concuss^. | ||||
| SmullIgan et al. (2024) ( | USA | Cross-sectional study | To investigate dizz., vestibular/oculomotor symptoms, and cervical spine proprioception among adults w and w/o a concussion history | 42 Concuss^ | M = 21 | Concuss^ | NR | ✓ | 6 mths–3 yrs | No neurological conditions and limited physical activity | ||||
| Lin et al. (2015) ( | Taiwan | NR | It examined the variations in balance function and sensory integration that occur within 1 wk. following an mTBI and compared the differences with those observed in healthy control pts | 107 mTBI (mean: 34.8 ± 14.8 yrs) | M = 150 | Mild | Loss of conscious <30 min. | ✓ (33) | ✓ (51) | ✓ (18) | ✓ (3) | ✓ (2) | 1 wk. | No history of epilepsy, |
| Campbell et al. (2021) ( | USA | NR | To identify peripheral vestibular, central integrative, and oculomotor causes for chronic symptoms following mTBI | 58 mTBI | M = 40 | Mild | Loss of conscious <30 min. | ✓ (8) | ✓ (31) | ✓ (7) | ✓ (12) | Mean 343 dys | No significant vestibular signs and cerebrovascular disease. No mod. to severe substance abuse | |
| Calzolari et al. (2021) ( | UK | NR | It was investigated the brain mechanisms of imbalance in acute TBI, its link with vestibular agnosia, and potential clinical impact | 37 TBI | M = 42 | Mild (n4) | Mayo TBI severity classification system ( | ✓ (20) | ✓ (14) | ✓ (3) | 2–77 dys | No active pre-morbid medical, neurological or psychiatric condition, musculoskeletal condition impairing ability to balance, substance abuse history | ||
| Felipe and Shelton | USA | NR | To evaluate subclinical cervical abnormalities in the vestibulospinal pathway in pts. w/ a concussion history, w/ and w/o related symptoms, using c-VEMP | 45 Normal | Concuss^ | NR | ✓ | NR | No significant audio-vestibular signs and cerebrovascular disease | |||||
| Christy et al. (2019) ( | USA | NR | Compare athletes with and without sport-related concussions on the subtests | 28 Concuss^ | M = 65 | Concuss^ | NR | ✓ | 17 pts.: 72 h | n13: Prev. concuss^ | ||||
| Gard et al. (2022) ( | Sweden | NR | To establish the cause of vestibular impairment in athletes with concussion who have persisting post-concussive symptoms | 21 w/ prev. Concuss^ | M = 25 | Concuss^ | NR | ✓ | Min. 6 mths ff concuss^ | No prev. or current self-reported neurological or psychiatric disorder | ||||
| Kim et al. (2024) ( | Korea | NR | To evaluate the characteristics of head trauma and brain injury and assess the relationship between them and treatment outcomes in patients with t-BPPV | 63 (18–62 yrs) | M = 34 | NR | NR | ✓ (34) | ✓ (25) | ✓ (4) | 2–15 dys | No history of other labytrinthine or central nervous system disorders |
| Ref | Gender | Severity of TBI | Fall | MVA | Assault/ direct impact | Sports injury | Other | Patients reported auditory symptoms | Vestibular | PROMS |
|---|---|---|---|---|---|---|---|---|---|---|
| Schuknecht and Davison (1956) ( | M | NR | ✓ | C3: Severe vertigo, nausea for dys | ||||||
| Preber and | M = 2 | NR | ✓ | ✓ | C1/2: Vertigo w/ position changes | |||||
| Tonkin and Fagan | M = 3 | NR | ✓ | C7: Unsteady on feet | ||||||
| Herdman (1990) ( | M = 2 | NR | ✓ | ✓ | C1: Dizz., vomiting, headache, blurred vision, diplopia & ataxia | |||||
| Lyos et al. | M = 3 | NR | ✓ | ✓ | ✓ | C1: Nausea, vertigo | ||||
| Kleffelgaard et al. (2016) ( | M = 2 | Mild | ✓ | ✓ | ✓ | C1: | ||||
| Feneley and Murthy | M | NR | ✓ | Support to sit upright; fell to sides. Remained unsteady standing w/ support | ||||||
| Bertholon et al. | M | NR | ✓ | Positional vertigo when rolling onto right or left side in bed | ||||||
| Lerut et al. | F | NR | ✓ | Vertigo | ||||||
| Fujimoto et al. (2007) ( | M | NR | ✓ | NR | ||||||
| Johnson (2009) ( | F | Mild | ✓ | Chronic vertigo; initial vertigo, nausea & emesis. Intermittent position-provoked vertigo (<1 min) w/ nausea; no recent emesis | ||||||
| Ralli et al. (2010) ( | M | NR | ✓ | Shortly severe vertigo | ||||||
| Dlugaiczyk et al. (2011) ( | M | NR | ✓ | Strong vertigo in bed, bending over, or looking up | ||||||
| Chung et al. | M | NR | ✓ | Mild dizz. & ataxia | ||||||
| Sousa Menezes et al. (2019) ( | M | NR | ✓ | Severe dizz., vertigo, otalgia or otorrhea | ||||||
| Jafarzadeh et al. (2022) ( | M = 20 | Mild | ✓ | n21: persistent vertigo or n14: imbalance | ||||||
| Ylikoski et al. | M = 2 | NR | ✓ | C8: Constant unsteadiness; unable to walk straight | ||||||
| Jani et al. (1991) ( | F | Mod-Severe | ✓ | NR | ||||||
| Fitzgerald | F | NR | ✓ | Positional vertigo, motion intolerance | ||||||
| Ottaviano et al. (2009) ( | F | NR | ✓ | Vertigo | ||||||
| Kagoya et al. (2010) ( | F | NR | ✓ | Dizz. w/ head position changes; subsided over 2 M | ||||||
| Paxman et al. (2018) ( | M | Mild | ✓ | Persistent dizz., light-headed, disorientation, nausea, fatigue. Worse w/ activity, posture/ contrast changes, convergence, improved w/ rest | ||||||
| Roup et al. (2020) ( | F | Mild | ✓ | Dizz. & problems w/ balance | ||||||
| Waninger et al. (2014) ( | M | Concuss^ | ✓ | NR | ||||||
| Honaker et al. (2015) ( | M = 80 | Concuss^ | ✓ | Athletes w/ previous concuss^: | ||||||
| Hides et al. | NR | Concuss^ | ✓ | NR | ||||||
| Christy et al. (2019) ( | M = 65 | Concuss^ | ✓ | NR | ||||||
| Felipe and Shelton | F = 154 | Concuss^ | ✓ | Symptom grp: dizz., persisting > 10 dys | ||||||
| Glendon et al. (2021) ( | M = 25 | Concuss^ | ✓ | NR | ||||||
| Teramoto et al. (2022) ( | M = 59 | Concuss^ | ✓ | NR | ||||||
M/F pts. had significantly higher scores at post-injury than pre-injury F reported more symptoms than M in all categories but there were statistically significant differences in smooth pursuit, horizontal saccades & vertical saccades | ||||||||||
| Brown et al. (2022) ( | Athlete: | Concuss^ | ✓ | Self-reported history of concuss^ | ||||||
| Gard et al. | SRC: | Concuss^ | ✓ | Vestibular disturbance | Vestibular dysfunction in 13 of 21 pts. w/ SRC (Peripheral: 9, central & peripheral: 4) | |||||
Vestibular dysfunction did not correlate with gender | No correlation with DHI | |||||||||
| Smulligan et al. (2024) ( | M = 21 | Concuss^ | ✓ | NR | ||||||
There is no statistically significant association between gender & performance on the Visio-vestibular exam | No statistically significant association between gender and DHI | |||||||||
| Uyeno et al. | M = 63 | Mild | ✓ | NR | ||||||
| Kanavati et al. | M | NR | ✓ | Dizz. | ||||||
| Durbec et al. | M | NR | ✓ | Loss of balance | ||||||
| Jacobs et al. | F | NR | ✓ | Intermittent nausea, light-headedness, & vertigo | ||||||
| Mohd Khairi et al. (2009) ( | M | NR | ✓ | NR | ||||||
| Blackard et al. (2020) ( | F | Concuss^ | ✓ | Mild concuss^ symptoms | ||||||
| Lin et al. (2015) ( | mTBI | Mild | ✓ | ✓ | ✓ | ✓ | ✓ | NR | ||
| Campbell et al. (2021) ( | Chronic mTBI: | Mild | ✓ | ✓ | ✓ | ✓ | > 3 mths post mTBI w/ non-resolving balance complaints (for mTBI grp) | |||
| Galea et al. (2022) ( | mTBI: | Mild | ✓ | ✓ | ✓ | ✓ | NR | |||
| Ouchterlony et al. (2016) ( | M = 34 | Mild | ✓ | ✓ | ✓ | ✓ | ✓ | BPPV: 90.5%; NSD: 76.2% spinning w/ dizz. | ||
BPPV grp had significantly more in pts. with mod. TBI (23.8%) than the NSD grp All of NSD grp had mild TBI | ||||||||||
| Calzolari et al. | TBI | Mild | ✓ | ✓ | ✓ | NR | ||||
15 pts. with mod-severe TBI 3 pts. with mild TBI | ||||||||||
| Taylor et al. (2022) ( | M = 40 | Mild | ✓ | ✓ | ✓ | ✓ | ✓ | Dizz. and/or balance symptoms | 33 pts. (33.3%) had abnormalities involving one or more vestibular organs/afferent divisions | |
No significant relationship between presence of abnormalities on vestibular function tests & gender | ||||||||||
| McCormick et al. (2023) ( | M = 14 | Concuss^ | ✓ | ✓ | ✓ | ✓ | Dizz. | n11 (22%) had positive BPPV | ||
| Kim et al. (2024) ( | M = 34 | NR | ✓ | ✓ | ✓ | NR | ||||
Mostly posterior SCC post-traumatic BPPV was more prevalent in M than in F, which may be attributed to gender differences in the incidence of TBI | ||||||||||
| Joseph et al. (2021) ( | M = 31 | Mild (n24) | ✓ | ✓ | ✓ | NR | ||||
No statistically significant relationship between vestibular score & gender in SOT | No significant effect of gender on DHI score in SOT vestibular score. | |||||||||
| Motin et al. | M = 18 | Severe | ✓ | ✓ | ✓ | Vertigo w/ positional changes/physical exertion, relieved by rest; light-headedness, floating, drunkenness sensations | ||||
| Ahn et al. (2011) ( | M = 18 | NR | ✓ | ✓ | ✓ | Vertigo | ||||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVestibular and auditory disorders · Traumatic Brain Injury Research · Hearing, Cochlea, Tinnitus, Genetics
Introduction
1
Traumatic Brain Injury (TBI) is a widespread cause of death and disability worldwide (1, 2). TBI, with its associated physical, behavioural, cognitive and emotional deterioration (3–5), not only adversely impacts the quality-of-life of individuals but also causes a global burden on states due to the costs it incurs (6). It is estimated that the annual cost of TBI in the United Kingdom (UK) alone is 15 billion pounds (7).
Different methods are used for classifying the severity of TBI. Commonly, the Glasgow Coma Scale (GCS) at the time of injury and the duration of post-traumatic amnesia are employed for classification of TBI as mild (GCS: 13–15; post-traumatic amnesia: <24 h), moderate (9–12; >24 h), or severe (3–8; >7 days) (8). For TBI cases presenting to the hospital, more than 90% are classified as mild TBI (9). The common causes (aetiologies) known to lead to TBI include motor vehicle accidents (MVA), falls, sports-related injuries, assaults (all of these also known as non-blast related) and explosions (blast-related). The mechanisms of brain injury can vary across different aetiologies, particularly between blast-related and non-blast related TBI. In blast-related TBI, damage occurs due to the high-pressure waves generated during the explosion, whereas in non-blast related TBI, damage is typically observed as a result of a blunt force trauma to the head, concussion, or penetration (10). Due to this fundamental distinction and the different damage that would be related to distinct vestibular issues, the focus of this review will be on non-blast related TBI.
Dizziness, vertigo and imbalance stand out as some of the most commonly reported issues associated with TBI. The prevalence of dizziness and/or vertigo post-TBI was found to be between 23.8 and 81% (11, 12). The unpredictable damage caused by TBI to the brain can complicate the detection of the exact source of resulting vertigo and/or dizziness complaints. However, anatomically, TBI can lead to these symptoms by causing damage to the peripheral and central vestibular systems, brainstem pathways, as well as visual, motor, and oculomotor pathways (13). For example, currently, the most commonly reported peripheral vestibular disorder post-TBI is Benign Paroxysmal Positional Vertigo (BPPV) (14–16).
Despite the availability of many studies related to vestibular outcomes associated with TBI, there is a need for a comprehensive review synthesising common vestibular findings related to non-blast related TBI, including the relationship of TBI aetiology, severity and gender with vestibular conditions. A review conducted for this purpose can contribute to the development of diagnostic and treatment methods in this patient group, helping to identify appropriate and effective strategies for addressing vestibular complaints. Thus, a wide range of benefits can be achieved in the long term, from improving individual quality-of-life to alleviating the economic burden on states.
The aim of this study is to map and synthesise the literature on vestibular impairments associated with non-blast related TBI, with specific consideration of the potential influence of injury severity, aetiology, and gender.
In particular, the research questions are:
i) What are the common vestibular assessments and impairments of TBI,ii) Whether vestibular outcomes vary according to severity of TBI,iii) Whether vestibular outcomes vary according to aetiology of TBI,iv) Whether vestibular outcomes vary by gender following TBI.
To address these broad and diverse research questions, map the literature, summarise the findings, and synthesise evidence from more than one study design, a scoping review was selected as the most appropriate approach (17, 18).
Materials and methods
2
This scoping review followed the 6-stages framework developed by Arksey and O’Malley (18). These stages were conducted in the following order: (1) identifying the research question(s), (2) identifying the relevant studies using appropriate keywords, (3) selecting relevant studies through an iterative scanned title, abstract, and full text, (4) extraction and charting the data, (5) collating, summarising and reporting of the results, (6) clinician review. The review was conducted in accordance with the PRISMA-S guidelines (19) (see Supplementary Appendix Table 1 for PRISMA-ScR Checklist).
Identifying the research question(s)
2.1
The research questions (listed above) were developed collaboratively with team members based on existing knowledge and literature in the field.
Identifying relevant studies
2.2
Eligibility criteria
2.2.1
To be included, records had to report studies involving adults (≥18 years old) with non-blast related TBI, focusing on vestibular outcomes and assessments. This included self-reported vestibular outcomes if vestibular impairment was clinically confirmed. If articles reported both auditory and vestibular outcomes, only the vestibular components were included. Records were eligible if they reported symptoms or assessment pre-treatment and were sourced from cohort studies, randomised control trials, case series, and case studies, as well as from grey literature such as dissertations and theses. In studies where treatments (e.g., Epley or Semont manoeuvre) were applied, the follow-up assessments were not reported in this review. Only initial (pre-treatment) assessments, including any follow-up conducted before treatment were reported. All records included in the study were published in English language and were available in full text. Cases that did not meet our inclusion criteria were removed from the case series studies.
Records were excluded if the studies were reporting adults who may have experienced blast-related TBI, whiplash injuries or non-TBI conditions (e.g., strokes, acoustic neuroma), TBI in childhood or with pre-existing audio-vestibular disorders prior to TBI, or where the aetiology of TBI was unspecified. Records were also excluded if they did not clearly define TBI or did not report structural injury or functional impairment resulting from TBI or only reported auditory condition without any assessment of vestibular outcomes or broadly focused on balance assessments rather than vestibular-specific tests. Records reporting the reliability and validity of tests, animal studies, review articles, including systematic reviews, book chapters, qualitative research studies and any sources presenting protocols, personal/expert opinions or tutorials were excluded.
Search strategy
2.2.2
The research strategy was developed by the research team and was supported by a medical information specialist (Dr Farhad Shokraneh). The search was conducted following Cochrane Handbook (20) and Cochrane’s MECIR (21) and PRESS guideline for peer-reviewing the search strategies (22). Electronic databases were searched, including Embase, MEDLINE, ProQuest Dissertations & Theses A&I, PsycINFO, Science Citation Index Expanded and SPORTDiscus. Initial searches were conducted in May 2022. An additional database search of Cochrane Central Register of Controlled Trials (CENTRAL) was conducted in November 2025. The search strategy included keywords on TBI, auditory and vestibular conditions (a separate review was conducted for auditory outcomes). These were reviewed and revised following a primary search (see Supplementary Appendix Table 2 for search strategy). Specific search term strategies were employed across each search engine, covering article topics, titles, abstracts, and keywords. Filters were implemented to select articles written in English language and involving human participants only, when feasible. No limitations were imposed on the search timeframe. Additionally, manual searches of reference lists and prominent journals, identified using the interquartile rule for outliers, were conducted to identify additional eligible documents. The final database and manual searches were conducted in November 2025.
Study selection
2.3
Records retrieved from electronic searches were transferred to EndNote (version X9), containing citation, title, and abstract, where duplicates were eradicated. Four researchers (KB, KF, LE, OP) independently screened the records via Rayyan (23), initially scrutinizing the title and abstract, followed by a review of the full text. Lead researcher (KB) was responsible for screening all records. The records obtained as a result of the manual search were subjected to full-text screening. In instances of discordance regarding the eligibility of any record, reviewers deliberated on their reasons until an agreement was reached, or a third reviewer (VK) was consulted to achieve a majority decision.
Extraction and charting of the data
2.4
A data extraction form was created and developed in Microsoft Excel and piloted on five included records and was subsequently modified following team discussions. Data from each record was extracted by the lead researcher (KB) and checked by KF. Data were extracted on study characteristics, study population, TBI characteristics, vestibular complaints and assessments/outcomes, and limitations (Box 1).
BOX 1 Data extraction fields AuthorsYear of publicationCountry where study was conductedStudy titleAim of studyStudy designStudy populationSample sizeAgeGenderClassification method for TBISeverity of TBICauses/aetiology of TBIStatus pre/post-TBIPresence of comaRadiological resultsList of vestibular complaintsList of vestibular assessment toolsVestibular outcomesAssessment time since injurySingle or repeated assessmentsStudy limitations
Collating, summarising and reporting results
2.5
Extracted data were collated and categorised depending on the objectives of our research. Each relevant study was grouped according to categories such as vestibular outcomes, severity of TBI, aetiology, and gender effects. Data were then summarised to highlight common patterns and significant variations in vestibular outcomes.
Clinician review
2.6
Following the identification of categories, categorised findings were reviewed by clinicians (LE & VK).
Results
3
The process of record identification and selection is in the PRISMA flow diagram (Figure 1). Electronic searches were produced in an initial set of 19,188 records. After removing duplicates, 12,561 records remained and of these, 12,024 were excluded during the title and abstract screening due to not meeting the eligibility criteria. Manual searches identified a further 12 potential articles which were subjected to full-text screening. Of the remaining 549 records, a further 499 records were excluded at the full-text screening. Most commonly the studies excluded did not report TBI or clearly define TBI, included participants under 18 years old and did not report TBI aetiology. Full-text records could not be located for 31 records. None of these records could be traced, regardless of support from the University of Nottingham librarian. The electronic and manual searches resulted in a final list of 50 eligible full-text records for data collection.
The PRISMA flow diagram for the study selection process.
Study characteristics
3.1
Table 1 summarises the characteristics of the study and participants. Among the 50 included articles, the most commonly reported study design was case report(s)/case series (27/50, 54%) (24–50). The other study designs are shown in Table 1. Articles were published from 1956 to 2024. Studies were mainly conducted in the United States (n = 19), followed by the UK (n = 4) and Australia (n = 4) (Table 1).
Participant characteristics
3.2
Across 50 records, 1,793 participants were included. Of these, 1,218 were in the patient group (all group participants who had TBI, whether they had symptoms or not), whilst 575 were in the control group (either healthy controls or with vestibular symptoms). Pre-TBI status or history of participants are shown in Table 1, however this information was not consistently reported across all studies. Assessment time since injury varied widely across studies, ranging from as early as 2 days (24) to an average of 584.5 days (51) (Table 1). Four sports-related concussions studies included a pre-session baseline assessment (52–55). In 8 studies, follow-up/s’ assessments were performed after the initial time of injury before any treatment was offered (24, 25, 28, 31, 34, 38, 40, 49).
Overview of vestibular assessments and impairments following non-blast related TBI
3.3
Many different symptoms were reported in included studies, from brief dizziness experienced with changes in head position to prolonged dizziness and vertigo accompanied by nausea. These symptoms were assessed using a variety of tests and patient-reported outcome measurements (PROMs). The following sections briefly describe the vestibular assessments, PROMs and findings. A detailed summary of the assessments and PROMs is presented in Supplementary Appendix Table 3, and the results are demonstrated in Table 2. The vestibular impairments reported in the records are presented in Supplementary Appendix Table 4.
Dynamic positional tests
3.3.1
The Dix-Hallpike manoeuvre (56, 57) and the side-lying manoeuvre are used in the differential diagnosis of both peripheral and central types of positional vertigo and posterior and anterior semicircular canals (SCCs) BPPV. The Roll manoeuvre is used to diagnose horizontal SCC BPPV (57). The Dix-Hallpike manoeuvre was reported in 18 studies (25, 30, 38, 40, 43, 46, 49, 50, 52, 58–66) and the side-lying manoeuvre was used in one study (65), whilst both the Dix-Hallpike and Roll manoeuvres (horizontal SCC manoeuvre/supine head turning) were applied in 8 out of the 18 records (25, 46, 52, 59, 63–66). In one study, participants were prospectively audited for the presence or absence of BPPV without any manoeuvres (67), whilst in another study, participants were retrospectively monitored (68).
Positive results in favour of BPPV were observed in 16 out of 18 records in which the Dix-Hallpike and Roll manoeuvres were applied (25, 30, 38, 40, 46, 49, 50, 58–66). Posterior SCC BPPV was reported in 11 of these studies (25, 30, 40, 46, 50, 58–60, 64–66). Horizontal (lateral) SCC BPPV was observed in 6 records (25, 46, 59, 63, 64, 66). Furthermore, the two audit studies, one prospective and one retrospective, Calzolari et al. (67) and Taylor et al. (68) reported the presence of BPPV in participants. Ottaviano et al. (32) reported left post-traumatic benign positional vertigo without specifying the manoeuvre used.
Oculomotor assessment and/or nystagmography (ENG/VNG)
3.3.2
Oculomotor assessment provides a detailed examination of the neurological pathways associated with oculomotor function (69). The Electronystagmography (ENG) and Videonystagmography (VNG) test battery, which provides information about the function of the peripheral and central vestibular system (70), also includes an oculomotor assessment component.
Oculomotor assessment/screening was performed across 4 studies (46, 52, 62, 71). In the 3 studies, Binocular goggles (71), Frenzel goggles (52), or a light bar (62) were utilised; however, there was no detail of using VNG or ENG. Therefore, results from studies utilising VNG/ENG are reported separately from those without such specifications. In 3 studies, oculomotor assessment results were generally found to be normal or did not show significant differences compared to the control group or pre-concussion conditions (46, 52, 62). In one cross-sectional study, although abnormalities were detected in both athlete groups with and without a previous concussion, there was no significant difference in the distribution of normal and abnormal oculomotor findings between the groups (71). The examinations performed within the scope of each oculomotor assessment are provided in detail in Table 2.
In seven studies, eye assessments were presented under various names (e.g., neurological or bedside examination, neurotologic or neuro-vision assessment) (28, 37, 42, 43, 65) or with specific eye assessments such as spontaneous or gaze-evoked nystagmus (39, 49). Although the results were reported differently in each study, visual-vestibular abnormalities were observed in 5 out of 7 studies (28, 37, 39, 42, 65). However, in 1 out of 5 studies, abnormal results were detected in gaze and pursuit tests, whilst spontaneous nystagmus and saccades were normal (65). In remaining 2 studies, the results were normal (43, 49).
Furthermore, ENG (n = 6) (29, 38, 42, 44, 47, 49) and VNG (n = 7) (28, 32, 41, 43, 63, 68, 72) were utilised across a total of 13 studies. In four studies, one using VNG (41) and three using ENG (42, 47, 49), only caloric test results were presented, rather than ENG or VNG. Therefore, these findings are reported in the next section. Normal results were obtained across 3 studies (28, 38, 43), whilst abnormal VNG or ENG results were observed in 8 studies (29, 32, 38, 44, 49, 63, 68, 72) in at least one case. Notably, a normal VNG result was obtained 23 months post-TBI; however, the initial neuro-visual assessment conducted approximately 8 months after the TBI, revealed visuo-vestibular dysfunction in a case study (28). Abnormalities varied across studies, including findings such as spontaneous nystagmus, reduced vestibular responses, gaze-evoked nystagmus and positive optokinetic nystagmus indicating both peripheral and central vestibular dysfunctions (Table 2).
In an observational cohort study, visual vestibulo-ocular reflex assessment (VVOR) and vestibulo-ocular reflex suppression (VORS) were performed. Individuals with TBI showed more positive results in both the VVOR and VORS compared to the controls (63). Similarly, poor VOR suppression was observed in 3.6% of patients following TBI in a retrospective clinical case series study (68).
Vestibular-oculomotor screening (VOMS) tests the ability to complete vestibular and ocular-related performances and measures the level of symptoms provocation caused by them (73). It was used in 6 studies (34, 53–55, 74, 75). In all 6 studies, at least one subtest of VOMS showed impairment, abnormal findings or an increase in symptoms following concussion/TBI (34, 53–55, 74, 75).
Caloric test
3.3.3
The caloric test evaluates the horizontal SCCs and by extension the superior vestibular nerve (76). The caloric test was performed in 18 out of 50 studies (24, 26, 27, 31, 35, 36, 38, 41, 42, 44, 45, 47–49, 62, 67, 68, 72). In caloric testing, bilateral (24, 42, 48, 49), unilateral (27, 36, 41, 42, 44, 45, 49) vestibular dysfunction (e.g., canal paresis, reduced vestibular responses, vestibular areflexia) or abnormal results (68, 72) were reported in 11 out of 18 studies. One study noted central vestibular tonus differences (38), and 8 studies noted normal caloric responses (26, 31, 35, 38, 44, 47, 62, 67). However, one of these, unilateral canal paresis was observed in the follow-up assessment performed 23 months after the injury (31).
Head thrust/head impulse/video head impulse (vHIT) test
3.3.4
The above tests measure VOR and provides physiological information relating to SCC function (77, 78). Head thrust/impulse (n = 5) (33, 46, 49, 58, 71) and vHIT (n = 6) (52, 62, 63, 67, 68, 72) were performed in a total of 11 records. Normal (negative) results were obtained in 5 studies (33, 46, 49, 62, 67), whilst findings such as positive, increased asymmetry, and impairment were observed across 6 studies (52, 58, 63, 68, 71, 72). In two studies, the horizontal SCC was assessed (62, 71), while in two studies, all SCCs were reported to be evaluated (68, 72). In seven studies, there was no indication of which SCCs were assessed (33, 46, 49, 52, 58, 63, 67).
Head shaking test
3.3.5
Head-shaking test enables the determination of vestibular asymmetry by rapid head shaking and abrupt stopping movements (79). Head shaking test was used in three records (49, 58, 71). Abnormal results were observed in 2 studies (e.g., unstable optic disc or impairment in previous concussion group) (58, 71), whilst no nystagmus was observed in one study (49).
Vestibular evoked myogenic potential (VEMP) test
3.3.6
Among VEMPs, cervical VEMP (c-VEMP) evaluates the saccule via the sternocleidomastoid muscle, whilst ocular VEMP (o-VEMP) evaluates the utricle via the inferior oblique muscle (80, 81). VEMP measurement was performed in 8 studies (31, 43, 62, 65, 68, 72, 82, 83). In two studies, both c-VEMP and o-VEMP were applied (62, 68), in 4 studies only c-VEMP was performed (65, 72, 82, 83), and in 2 studies, it was not stated which VEMP method was used (31, 43). VEMP results were normal (31, 43, 62) or showed no significant difference between groups with or without TBI/concussion (62, 83) in four studies. In one study, VEMP was performed only at follow-up assessment (31).
In 4 studies, abnormal findings were observed (65, 68, 72, 82). In the group comparison performed by Felipe and Shelton (82), P13 and N23 latency scores were higher in the concussion group with symptoms and asymptomatic concussion groups than in the control and normative groups. However, there was no difference between the two concussive groups in terms of latency scores. Furthermore, only one study reported that bilateral abnormalities were observed (65).
Rotational testing
3.3.7
Rotational/Rotary chair test allows for the assessment of the VOR through the horizontal SCC (84). Rotary chair testing was utilised in 3 studies (49, 67, 83). Another study published in 1957 (38) used cupulometria evaluation (now not widely used), which is similar to the rotational test, and assesses vestibular responses through rotary chair but uses different stimulus magnitudes and durations (85). The results varied depending on the patients or cases, from normal gain to a severe bilateral vestibular deficit (Table 2). Furthermore, in a study comparing healthy athletes to those with concussions, there was no difference in VOR gain or phase (83). However, the timing of the rotary chair test implementation differs across studies (whether during the initial or follow-up assessments).
Furthermore, VOR thresholds and vestibular motion perceptual thresholds were evaluated using a rotary chair in one study (67). Vestibular motion perceptual thresholds measure the smallest appreciable stimulus or perceiving motion (86). In this assessment, dramatically elevated perceptual thresholds were observed in acute TBI patients with vestibular agnosia compared to controls. The VOR threshold was defined as the lowest acceleration required to elicit appropriately directed both slow and fast phases of vestibular nystagmus (87). Elevated VOR thresholds were observed in acute TBI (67).
Dynamic visual acuity (DVA) test and gaze stabilization test (GST)
3.3.8
Dynamic visual acuity (DVA) measures the ability to maintain visual clarity and focus on a target while the head is in motion, reflecting the function of the VOR (88). DVA test was performed in 2 studies (46, 58). A drop in visual acuity was observed in a participant with BPPV on one side and peripheral vestibular loss on the other side (58), whilst there are cases where positive DVA (≥4 lines difference) indicating reduced VOR or negative DVA results were reported following TBI (46).
Another test that evaluates VOR is the GST, which determines the head velocity that causes significant deterioration in visual acuity (89). In one study in which GST was applied, individuals with a previous concussion were found to have significantly larger GST asymmetry scores (71).
Posturography
3.3.9
Posturography provides information on balance function, interactions and impact of sensory system such as visual, vestibular and proprioceptive systems by evaluating body sway through the measurement of the centre of pressure displacement on a force-measuring platform (90). Posturography is divided into two: static and dynamic. Static posturography evaluates changes in the centre of pressure on a fixed platform (91), whilst dynamic posturography measures postural reactions on a moving platform (92). Posturography was used in 11 out of 50 studies (43, 46, 49, 51, 62, 65, 67, 68, 72, 83, 93). Three studies used static posturography (46, 67, 93) and seven studies used dynamic posturography (43, 49, 51, 62, 65, 68, 83). However, it was not specified in one study which type of posturography was used and observed abnormal results in 38% of participants with concussion (72).
The modified clinical test of sensory integration and balance (mCTSIB), one of the subtests of static posturography, was used in 2 studies (46, 93). Although the results were reported differently, unstability, increased sway or sensory integration dysfunction was observed after TBI in static posturography evaluation in all three studies (46, 67, 93). However, there is also a case where normal results were obtained (46). In addition, acute TBI patients with vestibular agnosia were more unstable on static posturography compared to those without vestibular agnosia (67).
Sensory organization test (SOT), which is one of the subtests of dynamic posturography, was performed in 6 studies (49, 51, 62, 65, 68, 83). In one of these studies, it was not stated that SOT was applied, but it was shown in the figure (49). The results were generally reported differently in each record based on their research aims. However, in general, two studies stated significantly abnormal responses/worse scores in TBI, or concussion groups compared to control groups (62, 83) and increased sway, imbalance or abnormal results on one or more SOT scores were observed in two studies (49, 68). The other two studies reported no significant statistical differences within TBI groups (e.g., symptomatic versus asymptomatic TBI or those with normal versus saccular abnormalities) (51, 65). In one study, the dynamic posturography results were normal following TBI (43).
Other tests
3.3.10
Hennebert’s sign, which is a pressure-induced nystagmus resulting from changes in pressure applied to the external auditory canal, can be a finding that indicates semicircular canal dehiscence, Meniere’s disease or vestibulofibrosis (94, 95). Fistula Test is used to assess the integrity of the bony labyrinth (95). Fistula test was negative in three studies (26, 29, 42). A positive Hennebert’s sign was observed in one study (39). In three of these studies, it was indicated through assessments that the patients had perilymphatic fistula (29, 39, 42).
PROMs
3.3.11
Symptoms, quality-of-life, functional status, experiences or satisfaction can be evaluated via PROMs (96). PROMs related to vestibular disorders were conducted in 14 studies (46, 51, 52, 54, 61–65, 67, 71, 72, 74, 93), of which 4 studies reported using two PROMs (46, 51, 62, 63). The most commonly used PROM was Dizziness Handicap Inventory (DHI) (13/14) (46, 51, 52, 61–65, 67, 71, 72, 74, 93). Two studies used the Neurobehavioural Symptom Inventory (NSI) (51, 62), whilst others used the space and motion discomfort-II (SMD-II) (63), Post-concussion Symptom Scale (PCSS) (54), and Vertigo Symptom Scale Short Form (VSS-SF) (46).
Following TBI/concussion, 11 studies observed impairment based on DHI (46, 51, 52, 61–63, 67, 71, 72, 74, 93). In 2 studies, only reported the mean score of DHI and did not provide any interpretation of the score (64, 65). However, in 5 out of 13 studies, group comparisons (e.g., pre-post, control, with and without vestibular agnosia, positive and negative BPPV, normal and abnormal saccular function) indicated no significant difference in DHI scores (52, 64, 65, 67, 71). In studies using other PROMs in addition to the DHI, impairments were detected, as shown in Table 2 (46, 51, 62, 63).
Effect of severity of non-blast related TBI on vestibular outcomes
3.4
Twenty-three studies have not clearly stated the severity of TBI (23/50) (24–27, 29–33, 36, 38–42, 44, 45, 47–49, 59, 60, 66). Of the remaining 27 studies (7 of which were case studies/series), 9 studies included mild TBI (28, 43, 46, 50, 55, 62, 63, 65, 93), 12 studies reported concussions (i.e., mild TBI) (34, 37, 52–54, 64, 71, 72, 74, 75, 82, 83), one observed moderate/severe TBI (35), one study included severe TBI (58). Two studies included a range from mild to severe TBI (51, 67), whilst two studies involved participants with mild and moderate TBI (61, 68) (see Table 1 for more details on severity).
In four studies that included various TBI severity groups, different assessments were conducted (51, 61, 67, 68), although three studies did not perform any statistical assessment regarding severity (51, 67, 68). In one case comparison interventional study, BPPV was detected significantly more in individuals with moderate TBI (61) and in another study, most individuals with BPPV had moderate to severe TBI (67). In final study, the severity of TBI at which BPPV occurred was not specified (68).
Of the 9 studies in which TBI severity was classified as mild, four were case studies (28, 43, 46, 50). In 2 out of the nine studies, normal peripheral and central vestibular function was observed (43, 46). Although one case study reported a normal result, it was unclear whether normal vestibular function was fully present, as only a VNG test was conducted (28). BPPV was identified in 5 studies following mild TBI (46, 50, 62, 63, 65), whilst in 5 studies, one of the possible diagnoses observed included sensory integration dysfunction (46, 62, 93), persistent sensorimotor impairment (63), or peripheral, central vestibulopathy (55).
Abnormal findings were obtained in at least one test or subtest in 12 studies involving concussion (34, 37, 52–54, 64, 71, 72, 74, 75, 82, 83). Of these 12 studies, two were case studies (34, 37). The most commonly used assessment was VOMS (5/12) (34, 53, 54, 74, 75). Among studies using dynamic positional tests, one identified both posterior and horizontal SCC BPPV (64), whilst the other found no BPPV post-concussion (52). Two studies reported no significant differences in vestibular assessments between pre- and post-concussion or between those with and without a history of concussion (52, 75), whilst three studies observed a significant increase in VOMS scores post-concussion or in patients with a concussion history compared to those without (53, 54, 74). Additionally, throughout concussion-related studies, abnormalities in vestibular function (34, 37, 72), saccular or vestibulocollic function abnormalities (82), vestibulo-oculomotor dysfunction (54), vestibular-vision interaction deficits (71), persistent chronic vestibulo-oculomotor symptom provocation (74), and impairments in the central integration of vestibular function (83) were observed. In the study reporting severe TBI, posterior SCC and bilateral BPPV were observed (58). In moderate/severe TBI, bilateral normal nystagmus was observed on caloric (35).
PROMs were not used in any study in the severe TBI group. In the studies that were used, the results were reported differently from each other and the score severity for DHI, which was the most frequently used in the studies, was not stated consistently in each study. However, both mild TBI and concussion were reported impairments ranging from moderate to severe (46, 74). Furthermore, in studies with various TBI groups from mild to severe, one reported a mild impairment (51) while the other stated a moderate impairment in DHI (67).
In summary, the impact of TBI severity on vestibular outcomes varies across studies. Different outcomes can be observed for each TBI severity, from normal vestibular function to sensory integration dysfunction. In addition, due to differences in the reporting of DHI results and methodological approaches among the studies, a common conclusion could not be reached on the effect of TBI severity on DHI outcome.
Effect of aetiology of non-blast related TBI on vestibular outcomes
3.5
To investigate the impact of different aetiologies associated with TBI, they were categorised into five groups: falls, motor vehicle accidents (MVA), sports-related injuries, assaults, and others. Although penetrating TBI was not explicitly reported as an aetiology in the included studies, cases with potentially penetrating mechanisms may be present within the “other” category (e.g., industrial injuries involving metal impact (45)). The majority of studies (26/50) reported falls as the cause (24, 25, 30, 31, 38–40, 42, 44, 46, 48–51, 58–68, 93), followed by 21 studies reporting MVA (26–29, 32, 35, 36, 38, 43, 46, 49, 58, 59, 61–64, 66–68, 93). Across these aetiologies, a wide range of vestibular impairments were observed; however, BPPV was associated across all aetiologies except those including only sports-related TBI/concussion and was particularly common following falls.
In 15 studies reporting at least one TBI related to falls (26/50), at least one vestibular test showed abnormal results (24, 25, 30, 31, 38–40, 42, 44, 46, 48–50, 60, 65). Posterior, horizontal or anterior SCC BPPV due to fall was observed (25, 30, 40, 46, 50, 60, 65). In 4 studies, BPPV was observed only in the posterior SCC (30, 40, 50, 65); in 2 studies, it was found in both the posterior and horizontal SCCs (25, 46), and in one study, it was identified in both the anterior and posterior SCCs (60). There were 5 studies in which caloric testing showed absent bilateral or unilateral responses (24, 42, 44, 48, 49), while three studies showed normal caloric responses following a fall (31, 38, 44). However, in two studies where normal results were obtained, abnormal caloric results were detected in the follow-up assessment (31, 38).
Across studies reporting MVA (21/50), the most commonly used vestibular assessments were the caloric test (n = 6) (26, 27, 35, 36, 38, 49) or ENG/VNG (n = 5) (28, 29, 32, 38, 43). Similar to findings following falls, a range of results was observed in caloric testing following MVA in the first assessment, from normal (26, 35) responses to unilateral/bilateral abnormalities (27, 36, 49) or central tonus differences (38). Additionally, both normal (28, 43) and abnormal results were recorded in VNG/ENG (29, 32, 38). BPPV (38) or benign positional vertigo (32) was observed in two studies. In one study, it supported normal peripheral and central vestibular function in all tests (43).
In 11 studies reporting sports-related concussion or TBI, various test batteries were used. However, the commonly applied assessment was the VOMS (5/11) (53–55, 74, 75). In all of these studies, abnormal results were obtained in at least one VOMS subtest. Moreover, three studies identified significant differences between groups pre- and post-TBI (53, 54) or between those with and without a concussion history (74). No study reported BPPV in studies that only included sports-related TBI/concussion. However, positional tests were performed in only one study (52). Furthermore, various outcomes were observed across studies, ranging from vestibular dysfunction (72), abnormalities in saccular or vestibulocollic function (82), peripheral vestibular deficits (71), central or peripheral vestibulopathy (55) or impaired central integration of vestibular function despite a normal peripheral vestibular system (83).
Out of 4 studies reporting different types of assaults, normal SCC response (33), unilateral vestibular dysfunction (41, 42), and somatosensory integration dysfunction (46) were detected. Three studies were classified under “other” causes of injury, including striking the back of the head (42), being hit by a volleyball during practice (34), and an object falling from a bookcase (47). Of these three studies, one reported normal vestibular finding (47), whilst the other two reported abnormal vestibular findings (34, 42), including nystagmus on VOMS or spontaneous right-beating nystagmus.
There were 11 studies that included participants with a variety of aetiologies, from falls to assault (51, 58, 59, 61–64, 66–68, 93) (results reported together under all aetiologies). In 5 out of the eleven studies, results of each participant were reported separately, BPPV was observed following TBI due to both MVA and falls (59, 61, 64, 67, 68) (Table 2). Additionally, in one study, BPPV was observed following TBI due to MVA (58), whilst in another study, BPPV was reported but results were not categorised by different aetiologies (e.g., MVA, falls and blow to head) (66). In all studies reporting the affected SCC in cases of BPPV, the posterior SCC was the most impacted following both MVA and falls (59, 64). McCormick and Kolar (64) reported that falls were a statistically significant TBI aetiology for BPPV. In addition, another study reported that falls were a common aetiology among participants with vestibular hypofunction (68).
Although PROMs were utilised in studies examining various TBI aetiologies, the results were not separately reported by aetiology across those studies. Therefore, the effect of aetiology on PROMs could only be assessed in studies focusing on a single aetiology. No PROMs were used in the studies reporting MVA. In studies reporting falls, one study observed moderate and severe impairments (46), whilst studies associated with sports-related injuries identified mild (52) and severe impairments (74) based on DHI scores.
Summarily, while BPPV is commonly observed, particularly due to falls, common or different vestibular findings were detected across various aetiologies, including peripheral and central vestibular dysfunctions, abnormal ocular or postural responses, and impairments in sensory integration.
Effect of gender on vestibular outcomes following non-blast related TBI
3.6
Out of the 50 studies, 21 included both genders (38, 46, 49, 51, 53–55, 58, 59, 61–68, 72, 74, 83, 93), whilst the remaining studies either reported only male participants (n18) (24, 25, 27, 30, 31, 33, 36, 37, 39, 41–45, 48, 60, 71, 75), or only female participants (n10) (26, 28, 29, 32, 34, 35, 40, 47, 50, 82). One study did not specify gender (52).
In 7 out of the 21 studies that included both genders, multiple participants were included, but no results were reported by gender (54, 55, 62, 63, 65, 83, 93). Six out of these 7 studies had more males than females following TBI (54, 55, 63, 65, 83, 93). In the remaining 14 studies, although there were studies with multiple participants, either a statistical analysis was conducted between genders (51, 53, 68, 72, 74), results were presented based on gender in at least one assessment (58, 59, 61, 64, 66, 67), or in case studies, results were reported individually for each patient (38, 46, 49). A statistically significant difference was found for females in smooth pursuit, horizontal, and vertical saccades in the VOMS assessment (53), whilst Smulligan et al. (74) reported no statistically significant relationship between gender and VOMS performance. In two studies with similar vestibular assessments, there was no significant difference between vestibular function abnormalities and gender (68), nor was vestibular dysfunction correlated with gender (72). Moreover, there was no statistically significant relationship between vestibular score and gender in SOT (51). In studies where separate results were obtained, including case studies by gender, BPPV was observed in both males and females (38, 46, 49, 58, 59, 61, 64, 67). However, in 4 out of 8 studies, the number of males with BPPV was higher than the number of females (58, 59, 61, 67). Furthermore, in Ahn et al. (59) study, the number of males with posterior SCC BPPV was higher than females, while in another study, no males were observed with posterior SCC BPPV (64). However, Kim et al. (66) also reported that posterior SCC BPPV was more prevalent in males than females following TBI. Additionally, in all the studies included in this scoping review, the SCCs in which BPPV was observed were not consistently specified (Table 2).
In studies reporting male participants only, in 9 out of 18 studies, the caloric test revealed either a normal response (31, 44) or bilateral (24, 31, 42, 48) and unilateral abnormalities (27, 36, 41, 42, 44, 45). Furthermore, in three studies including only male participants where positional tests were applied, right posterior SCC BPPV was observed (25, 30, 60), while horizontal (25) or anterior SCCs (60) BPPV accompanied posterior SCC in two of these studies. Of the 10 studies including only female participants, normal horizontal SCC function via caloric test was identified in three studies (26, 35, 47). Similarly, in studies involving only females, bilateral or unilateral posterior SCC BPPV (40, 50) and benign positional vertigo (32) were reported. Moreover, following TBI, a range of vestibular outcomes were identified across genders. In males, findings ranged, from normal SCC function (e.g., normal HIT) (33) or overall peripheral and central vestibular functions (43) to perilymphatic fistula (39, 42) or vestibular-visual interaction deficits (37, 71, 75). In females, reported impairments included perilymphatic fistula (29), vestibulo-oculomotor dysfunction (34), and impairments in saccular or vestibulocollic function (e.g., abnormal c-VEMP responses) (82).
None of the studies that included only females used PROMs. In the study with only males, although the previous concussion group had a wider score range, there was no statistically significant difference between the comparison group (71). Among the 12 studies that included both genders, only 3 reported PROMs by gender (46, 72, 74). In two studies, there was no statistically significant association between gender and DHI (74) or that gender was not correlated with DHI score (72). In the case study, severe impairment was reported in male patients, while severe or moderate impairment was observed in females (46).
In summary, a variety of vestibular impairments, including BPPV, perilymphatic fistula, and vestibulo-oculomotor dysfunction, were observed in both male and female participants across different studies.
Discussion
4
This scoping review synthesised the common vestibular impairments associated with non-blast related TBI and investigated the influence of TBI severity, aetiology, and gender on vestibular outcomes. We found large inconsistencies in the reporting of vestibular tests, results and demographics across the studies, which not only highlight methodological and clinical standardisation deficiencies, but also complicate the understanding of the overall impact of TBI on the vestibular system.
In this review, the most commonly detected peripheral vestibular deficit following TBI was BPPV, most frequently involving the posterior SCC (15, 97, 98), which aligns with the anatomical predisposition for otoconia to accumulate in this canal due to gravity (99). In accordance with the existing literature, we also found that TBI can cause damage to other peripheral vestibular structures, including the labyrinth, vestibular nerve, and otolith organs (15, 100). In contrast to the findings reported here, Akin et al. (101) found in their review that otolith organs may be more damaged compared to SSCs following TBI. However, this discrepancy may be due to differences in the inclusion criteria of the reviews, for example, Akin et al. (101) included blast-related TBI. Therefore, a comprehensive assessment of all vestibular components in TBI patients is essential to draw a definitive conclusion regarding the relative susceptibility of otolith organs and SSCs to damage following TBI.
Some studies yielded important findings regarding the central contributions to the vestibular system. For example, Taylor et al. (68) reported that patients with abnormal oculomotor function following chronic TBI had significantly more difficulty in vestibular-dependent conditions on the SOT. Other research highlighted that, despite normal oculomotor and peripheral vestibular function following chronic TBI, a high proportion of abnormal SOT performance was still observed (62). This review also identified that patients with normal peripheral vestibular function who exhibited vestibular agnosia (impaired self-motion perception), and along with acute TBI patients, showed greater posturography instability than those without vestibular agnosia (67). All these findings support the view that balance relies not only on the inner ear and brainstem pathways but also on cortical processing and integration of vestibular signals (102). Moreover, self-motion perception is considered to arise from the integration of multiple brain regions, rather than being localised to a single region (67).
Similar to vestibular tests, the lack of standardisation in the application of PROMs and the reporting of results was observed throughout the records. Although the DHI, which was more commonly used than other PROMs, identified impairments, findings from some studies indicate an inability to differentiate between different groups. This may be an indication that the DHI may not be an appropriate measure of vestibular symptoms and quality-of-life for this specific patient population. To our knowledge, there is no specific study on the validity and reliability of using the DHI for adults with TBI. However, a study investigating the clinical utility of the DHI for Children and Adolescents (DHI-CA) (103) post-concussion reported that its clinical utility was questionable (104). In this context, developing specific PROMs especially for vestibular impairments in adults with TBI or determining which of the existing PROMs is more suitable in this population can be important for evaluating the quality-of-life and monitoring rehabilitation processes.
The observation of both peripheral vestibular impairments and central impairments across different TBI severities, including mild TBI, may suggest that TBI severity does not necessarily influence vestibular outcomes. Similarly, BPPV was reported across all severities, although some studies found BPPV more frequently in moderate (105) or severe TBI (58) than in mild TBI. Remarkably, the finding that even after concussion, central processing of vestibular and visual information may be altered without affecting the peripheral vestibular organs or associated brainstem and cerebellar processes (83) underscores the importance of a comprehensive evaluation in all TBI severities.
The findings suggest that the aetiology of TBI may be associated with the presence of BPPV, influence of aetiology does not follow a clear pattern on other peripheral and central vestibular impairments. Although BPPV was commonly reported following fall in our review, in contrast, MVA was also reported to be one of the most frequent causes of BPPV in the literature (98, 106). Therefore, further studies specifically designed to understand the impact of TBI aetiology on vestibular findings are needed.
The observation of similar peripheral or central vestibular outcomes in both males and females, along with differing statistical results from included studies, made it difficult to draw conclusions about the gender differences. Regarding BPPV, the findings suggest that BPPV may be more common in males, whilst there are studies in the literature that report no gender difference in BPPV following TBI (106, 107). Additionally, in line with the results of Teramoto et al. (53), a few studies were found statistically significant higher impairment in females compared to males in some oculomotor and vestibular assessments (108, 109). However, since these studies were mainly conducted with adolescents and those experiencing sport-related concussions, the generalisability of these results to the entire adult TBI population is limited.
The timing of assessment can have a significant impact on the interpretation of vestibular outcomes following TBI. Although the post-injury assessment times were extracted in the included studies, the results were not analysed according to assessment time. The terms “acute” and “chronic” TBI are commonly used in the literature, whilst there is no consistent agreement regarding the exact time frames for these periods. For example, some of the included studies accepted the acute period to last up to approximately 3 months post-injury (67, 68), whereas other extended this period to 6 months (74). Future research should clearly define different TBI phases such as acute, subacute, chronic, or post-chronic, and stratify vestibular outcomes accordingly. This would allow investigation of whether the effects of certain variables differ over time and contribute to the development of more effective assessment and management strategies. Moreover, future studies should also investigate which vestibular tests and assessment protocols are most appropriate at different post-injury time points to provide guidance for clinical practice.
Our findings provide insights into the common peripheral and central vestibular impairments following non-blast related TBI, while highlighting the complexity of understanding the effects of factors such as severity, aetiology, and gender due to the multifaceted nature of vestibular deficits combined with the intricate nature of TBI. Future research should develop comprehensive vestibular assessment protocols for individuals with TBI and focus on consistent methodology and standardised reporting of results to better understand the effects of variables on vestibular findings.
Strengths and limitations
4.1
This scoping review study provided a comprehensive review of the literature related to the research questions. Through the established inclusion criteria, studies that precisely matched the definition of TBI were carefully selected to ensure the examination of TBI-specific findings. However, the differences across research questions and the heterogeneity in the study designs of the included studies (for example, high proportion of case studies/series) have complicated the synthesis and comparison of the findings. Furthermore, the assessment times reported following TBI (e.g., acute and chronic TBI) were widely variable between records, with some not reporting the assessment time clearly. Moreover, the assessment time for acute TBI is debated in the literature and therefore, it was not possible to group the data into acute and chronic TBI and as such we were unable to investigate the effect of assessment time. Additionally, due to the broad scope of the study, some vestibular findings accompanied by auditory findings in certain studies were addressed in another scoping review. Although including only English-language studies may have limited the results, the inclusion of studies from non-English-speaking countries allowed for the presentation of results from a broader perspective.
Conclusion
5
Our review has demonstrated the diversity of vestibular findings following non-blast related TBI. However, the complexities of the vestibular system and TBI, as well as inconsistencies in vestibular assessment methods and reporting approaches (e.g., lack of clear specification of oculomotor assessment method) and lack of consistent use of PROMs, limit a comprehensive understanding of vestibular findings in individuals with TBI. These limitations hinder the ability to identify which methods should be prioritised for vestibular assessment in individuals with TBI and, consequently, obstruct the development of diagnostic and therapeutic processes. In this context, future research should focus on adopting more consistent methodologies and standardised reporting practices to enhance vestibular assessment and management approaches for individuals with TBI. To achieve this, establishing some level of agreement or consensus on testing protocols can be beneficial. Additionally, investigating the effects of variables such as severity, aetiology, and gender on vestibular findings through large-scale studies is important for developing more effective interventions for this patient group.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Dewan MC Rattani A Gupta S Baticulon RE Hung YC Punchak M . Estimating the global incidence of traumatic brain injury. J Neurosurg. (2019) 130:1080–97. doi: 10.3171/2017.10.JNS 17352, 29701556 · doi ↗ · pubmed ↗
- 2Capizzi A Woo J Verduzco-Gutierrez M. Traumatic brain injury: an overview of epidemiology, pathophysiology, and medical management. Medical Clinics. (2020) 104:213–38. doi: 10.1016/j.mcna.2019.11.001, 32035565 · doi ↗ · pubmed ↗
- 3Benedictus MR Spikman JM Van Der Naalt J. Cognitive and behavioral impairment in traumatic brain injury related to outcome and return to work. Arch Phys Med Rehabil. (2010) 91:1436–41. doi: 10.1016/J.APMR.2010.06.019, 20801264 · doi ↗ · pubmed ↗
- 4Khoury S Benavides R. Pain with traumatic brain injury and psychological disorders. Prog Neuro-Psychopharmacol Biol Psychiatry. (2018) 87:224–33. doi: 10.1016/J.PNPBP.2017.06.007, 28627447 · doi ↗ · pubmed ↗
- 5Kornblith ES Langa KM Yaffe K Gardner RC. Physical and functional impairment among older adults with a history of traumatic brain injury. J. Head Trauma Rehabil. (2020) 35:E 320–9. doi: 10.1097/HTR.0000000000000552, 31996604 PMC 7335322 · doi ↗ · pubmed ↗
- 6Humphreys I Wood RL Phillips CJ Macey S. The costs of traumatic brain injury: a literature review. Clinico Econ Outcomes Res. (2013) 5:281–7. doi: 10.2147/CEOR.S 44625, 23836998 PMC 3699059 · doi ↗ · pubmed ↗
- 7Ahmed Z. Current clinical trials in traumatic brain injury. Brain Sci. (2022) 12. doi: 10.3390/brainsci 12050527, 35624914 PMC 9138587 · doi ↗ · pubmed ↗
- 8Teasdale G Jennett B. Assessment of coma and impaired consciousness: a practical scale. Lancet. (1974) 304:81–4. doi: 10.1016/S 0140-6736(74)91639-04136544 · doi ↗ · pubmed ↗