Long-term survival in extensive-stage small cell lung cancer: a case report on the integration of interventional bronchoscopy and systemic immunotherapy
Ganxiu Deng, Shixuan Yan, Victor Bwembya, Xiaoping Zhu, Zhibing Luo, Changwen Deng

TL;DR
A patient with advanced small cell lung cancer survived five years through a combination of bronchoscopy and immunotherapy.
Contribution
Demonstrates a novel integration of bronchoscopic interventions with systemic immunotherapy for long-term survival in extensive-stage small cell lung cancer.
Findings
A 65-year-old patient with extensive-stage SCLC achieved five-year survival through combined bronchoscopic and immunotherapy treatment.
Repeated bronchoscopic interventions enabled continuation of systemic therapy despite airway obstruction.
Systemic immune activation was observed following bronchoscopic ablation, correlating with sustained partial remission.
Abstract
Small cell lung cancer (SCLC) is an aggressive malignancy with a poor prognosis, particularly in patients with extensive-stage disease (ES-SCLC). Although the incorporation of immune checkpoint inhibitors (ICIs) into first-line chemotherapy has modestly improved survival, long-term disease control remains rare. Central airway obstruction (CAO), a common complication of advanced SCLC, often leads to respiratory failure and interruption of systemic therapy, further compromising outcomes. We report the case of a 65-year-old man diagnosed with ES-SCLC based on endobronchial ultrasound-guided transbronchial needle aspiration. The patient initially responded to platinum–etoposide chemotherapy but experienced treatment interruption during the COVID-19 pandemic, followed by recurrent malignant airway obstruction and respiratory failure. Repeated bronchoscopic interventions, including tumor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
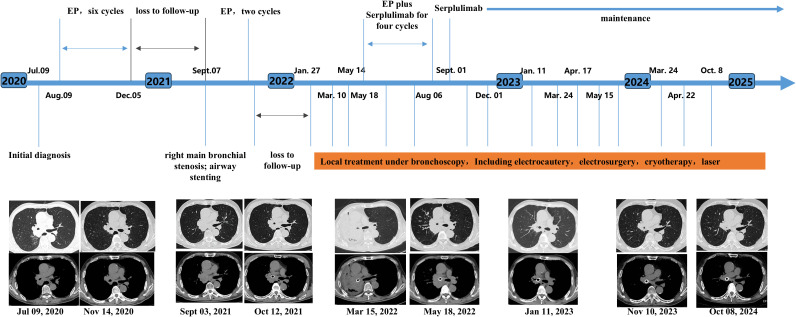 Figure 1
Figure 1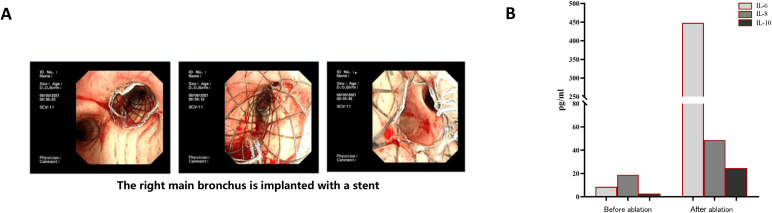 Figure 2
Figure 2| Time | Clinical events | Bronchoscopic intervention | Systemic therapy | Clinical outcome |
|---|---|---|---|---|
| Jul 2020 | Right hilar mass and mediastinal lymphadenopathy detected on chest CT; diagnosis of ES-SCLC confirmed by EBUS-TBNA | None | None | Initial diagnosis established |
| Aug–Dec 2020 | First-line treatment initiated | None | EP chemotherapy (etoposide + cisplatin), 6 cycles | Partial radiological response; symptoms improved |
| Dec 2020–Sep 2021 | Follow-up interrupted due to COVID-19 pandemic | None | Treatment discontinued | Disease progression suspected |
| Sep 2021 | Readmission with severe dyspnea and hypoxemia; severe right main bronchus stenosis on CT and bronchoscopy | Tumor debulking and placement of self-expandable metallic airway stent | EP chemotherapy reinitiated | Rapid relief of airway obstruction and respiratory symptoms |
| Late 2021 | Clinical stabilization | None | Continuation of EP chemotherapy | Temporary disease control |
| Early 2022 | Recurrent airway stenosis with dyspnea | Repeated bronchoscopic interventions including electrocautery, ablation, and cryotherapy | Supportive care | Airway patency restored; respiratory status improved |
| Early 2022 | Post-interventional immune activation observed | — | — | Circulating IL-6 and IL-8 levels significantly increased |
| 2022 | Systemic treatment escalation | Repeated bronchoscopic local ablation and cryotherapy as needed | Chemotherapy combined with PD-1 inhibitor (Serplulimab), 4 cycles | Partial remission achieved |
| 2022–2025 | Long-term disease control | Periodic bronchoscopic interventions for airway maintenance | Maintenance immunotherapy with Serplulimab | Sustained partial remission; good general condition at 5-year follow-up |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Research Studies · Lung Cancer Diagnosis and Treatment · Tracheal and airway disorders
Introduction
1
Small cell lung cancer (SCLC) is an aggressive neuroendocrine malignancy characterized by rapid tumor growth, early metastatic dissemination, and a high rate of recurrence (1). Approximately 10–15% of all lung cancers are classified as SCLC, and nearly 70% of patients present with extensive-stage disease (ES-SCLC) at the time of diagnosis (2–4). Despite initial sensitivity to platinum–etoposide chemotherapy, the majority of patients experience early disease progression, resulting in poor long-term outcomes. In recent years, the addition of immune checkpoint inhibitors (ICIs) to first-line chemotherapy has modestly improved overall survival in ES-SCLC (5, 6). however, durable disease control and long-term survival remain uncommon and are typically observed only in a small subset of patients (7–10).
Due to its rapid growth pattern and tendency for peribronchial infiltration, SCLC frequently involves the central airway, leading to central airway obstruction (CAO) in patients with advanced disease (4). CAO can cause severe dyspnea, post-obstructive pneumonia, and respiratory failure, often resulting in deterioration of performance status and interruption or discontinuation of systemic antitumor therapy. While chemotherapy and radiotherapy remain the cornerstone of treatment for ES-SCLC, these modalities are often insufficient to rapidly relieve life-threatening airway compromise (11). In this setting, bronchoscopic interventions—including tumor debulking, airway stent placement, and local ablation techniques—play a critical role in restoring airway patency and stabilizing respiratory function. Traditionally regarded as palliative measures, these interventions have primarily been used to alleviate symptoms and improve quality of life in patients with malignant airway obstruction (12, 13).
Emerging evidence suggests that local tumor ablation may exert immunomodulatory effects beyond mechanical airway relief by inducing tumor antigen release and remodeling the tumor microenvironment toward a more immunologically active state (14–19). This has generated growing interest in the potential synergy between local ablative therapies and systemic immunotherapy. However, clinical evidence supporting the integration of bronchoscopic local interventions with immune checkpoint blockade in ES-SCLC remains limited. In this context, we report a rare case of ES-SCLC complicated by recurrent central airway obstruction, in which repeated bronchoscopic interventions combined with chemotherapy and immunotherapy were associated with sustained disease control and long-term survival.
Case description
2
A 65-year-old male was admitted to Shanghai East Hospital in July 2020 after chest computed tomography (CT) revealed a mass in the right hilar region accompanied by multiple enlarged mediastinal lymph nodes (Figure 1). The patient had a 30-year history of cigarette smoking (approximately one pack per day). Endobronchial ultrasound-guided transbronchial needle aspiration (EBUS-TBNA) of the right hilar lesion was performed, and pathological examination confirmed small cell lung cancer (SCLC). Immunohistochemical analysis demonstrated positivity for CD56, chromogranin A, and synaptophysin, with a Ki-67 proliferation index of approximately 60%, while PD-1 and PD-L1 expression were negative. Further evaluation revealed enlarged lymph nodes in the right axilla. Brain magnetic resonance imaging and contrast-enhanced abdominal CT showed no evidence of distant metastases. Based on these findings, the patient was diagnosed with extensive-stage SCLC (ES-SCLC).
Timeline of patient treatment. EP, etoposide plus cisplatin chemotherapy regimen.
After exclusion of treatment contraindications, the patient received six cycles of first-line platinum–etoposide (EP) chemotherapy (etoposide 100 mg/m² on days 1–3 and cisplatin 75 mg/m² on day 1, every 3 weeks) from August to December 2020. A partial radiological response was achieved, with improvement in clinical symptoms. However, regular follow-up and further treatment were interrupted due to the COVID-19 pandemic.
In September 2021, the patient was readmitted with severe dyspnea and hypoxemia, with an oxygen saturation of 85% on room air. Chest CT demonstrated severe stenosis of the right main bronchus, which was confirmed by bronchoscopy, showing near-complete luminal obstruction caused by tumor tissue (Figure 1). Urgent bronchoscopic tumor debulking was performed, followed by placement of a self-expandable metallic airway stent (Figure 2A). After relief of the central airway obstruction, the patient’s respiratory symptoms and oxygenation improved markedly. His overall clinical condition and performance status improved sufficiently to allow stabilization of respiratory failure and resumption of systemic antitumor therapy. Based on the favorable response to prior chemotherapy, the EP regimen was reinitiated on September 14, 2021.
(A) The right main bronchus is implanted with a stent under bronchoscopy; (B) circulating cytokines IL-6 and IL-8 significantly increased after bronchoscopic local interventional therapy.
Despite initial clinical stabilization, regular follow-up was again disrupted during the pandemic period. In early 2022, the patient was readmitted because of recurrent dyspnea due to restenosis of the right main bronchus. During this period, multiple bronchoscopic interventions were performed to maintain airway patency, including electrocautery, laser therapy, ablation, and cryotherapy. Cryotherapy was administered using repeated freeze–thaw cycles under bronchoscopic guidance, with each freeze lasting approximately 20–40 seconds, tailored to the extent of endobronchial tumor involvement. No clinically significant complications related to tumor debris retention, massive hemoptysis, or procedure-related infection were observed. Supportive treatment, including anti-infective therapy and oxygen supplementation, was provided as needed.
Following bronchoscopic local ablation, peripheral blood analysis revealed transient elevations in circulating inflammatory cytokines, including interleukin-6 (IL-6) and interleukin-8 (IL-8) (Figure 2B). The patient’s respiratory status improved, and airway patency was successfully restored.
Subsequently, systemic therapy was escalated to combination treatment with chemotherapy and the programmed cell death protein-1 (PD-1) inhibitor serplulimab. After four cycles of combination therapy, the treatment regimen was transitioned to maintenance monotherapy with serplulimab. During follow-up, the patient underwent periodic bronchoscopic interventions, including ablation and cryotherapy, to maintain airway patency. No severe immune-related adverse events were observed, and no clinically significant complications related to the airway stent, such as infection, hemoptysis, or symptomatic granulation tissue formation, occurred.
Radiological evaluation demonstrated sustained partial remission, with marked reduction of the right hilar mass and preservation of patency in the right main bronchus. At five years after the initial diagnosis, the patient remains alive with stable disease and good general condition. The detailed clinical course and treatment timeline are summarized in Table 1.
Discussion
3
Small cell lung cancer (SCLC) is characterized by rapid tumor growth, early metastatic dissemination, and a high propensity for relapse, resulting in a historically poor prognosis, particularly in patients with extensive-stage disease (ES-SCLC) (4). Although the addition of immune checkpoint inhibitors (ICIs) to platinum–etoposide chemotherapy has modestly improved overall survival, durable long-term survival remains uncommon and is typically confined to a small subset of patients (20). In this context, the present case is notable for achieving sustained disease control and survival exceeding five years, highlighting the potential clinical value of integrating bronchoscopic local interventions with systemic chemotherapy and immunotherapy.
Central airway obstruction (CAO) is a frequent and life-threatening complication in advanced SCLC, often leading to respiratory failure, recurrent infections, and rapid deterioration in performance status. While systemic therapy remains the cornerstone of treatment, it is often insufficient to promptly relieve critical airway compromise. In such scenarios, bronchoscopic interventions play a pivotal role by rapidly restoring airway patency, improving ventilation and oxygenation, and stabilizing the patient’s clinical condition (11, 12, 21). In our case, repeated episodes of severe airway stenosis led to respiratory failure and interrupted systemic therapy. Timely bronchoscopic tumor debulking and airway stent placement effectively alleviated obstruction, enabling the patient to recover respiratory function and resume systemic antitumor treatment. Importantly, these interventions did not directly enhance drug delivery but rather improved physiological reserve and treatment tolerance, thereby allowing continued chemotherapy and immunotherapy. Beyond their mechanical and palliative benefits, bronchoscopic local ablation techniques may exert immunomodulatory effects that complement systemic immunotherapy (22, 23). Local tumor ablation induces tumor necrosis and apoptosis, facilitating the release of tumor-associated antigens and danger-associated molecular patterns, which can promote dendritic cell activation and antigen presentation (24, 25). This process may remodel the tumor microenvironment from an immunologically “cold” state toward a more inflamed and immune-responsive phenotype (17, 19, 26). Preclinical and clinical studies have demonstrated that local ablation can increase infiltration of CD4^+^ and CD8^+^ T cells while reducing immunosuppressive populations such as regulatory T cells, thereby enhancing antitumor immune responses. Moreover, ablation-induced cytokine release, including IL-6 and IL-8, has been associated with immune activation and may contribute to systemic antitumor effects. In the present case, circulating levels of IL-6 and IL-8 were markedly elevated following bronchoscopic local ablation, suggesting a transient systemic inflammatory and immune activation response. While causality cannot be definitively established in a single case, this observation raises the possibility that repeated bronchoscopic ablation may have synergized with PD-1 blockade to enhance immune-mediated tumor control. Recent evidence supporting abscopal effects and STING-dependent type I interferon signaling following cryoablation further supports the biological plausibility of combining local ablation with immunotherapy (19). The durable partial remission observed in this patient may reflect not only effective airway management but also a favorable interaction between local tumor destruction and systemic immune modulation.
From a safety perspective, the patient tolerated repeated bronchoscopic interventions and long-term immunotherapy well, without major procedure-related complications, severe immune-related adverse events, or clinically significant stent-related sequelae such as hemoptysis, infection, or symptomatic granulation tissue formation. This favorable safety profile underscores the feasibility of repeated bronchoscopic interventions as part of a multidisciplinary treatment strategy in carefully selected patients.
Nevertheless, this case has several limitations. The patient’s treatment course and follow-up were intermittently disrupted during the COVID-19 pandemic, potentially influencing disease assessment and management continuity. Additionally, although multiple bronchoscopic biopsies were performed, molecular subclassification of SCLC based on transcriptional or immune signatures was not feasible, limiting insights into predictive biomarkers of immunotherapy response. Furthermore, multiple bronchoscopic modalities—including electrocautery, laser therapy, ablation, and cryotherapy—were used in combination, making it difficult to determine which specific technique contributed most significantly to the observed clinical benefit.
In conclusion, this case illustrates that bronchoscopic local interventions can serve not only as life-saving measures for malignant airway obstruction but also as critical enablers of sustained systemic therapy in ES-SCLC. When integrated with chemotherapy and immunotherapy, these interventions may contribute to prolonged disease control and long-term survival in selected patients. Although broader validation is required, this case supports a multidisciplinary treatment paradigm in which local airway management and systemic immunotherapy are strategically combined to optimize outcomes in advanced SCLC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Brody H . Lung cancer. Nature. (2020) 587:S 7. doi: 10.1038/d 41586-020-03152-0, PMID: 33208969 · doi ↗ · pubmed ↗
- 2Shepherd FA Crowley J Van Houtte P Postmus PE Carney D Chansky K . The International Association for the Study of Lung Cancer lung cancer staging project: proposals regarding the clinical staging of small cell lung cancer in the forthcoming (seventh) edition of the tumor, node, metastasis classification for lung cancer. J Thorac Oncol Off Publ Int Assoc Study Lung Cancer. (2007) 2:1067–77. doi: 10.1097/JTO.0b 013e 31815 bdc 0d, PMID: 18090577 · doi ↗ · pubmed ↗
- 3Govindan R Page N Morgensztern D Read W Tierney R Vlahiotis A . Changing epidemiology of small-cell lung cancer in the United States over the last 30 years: analysis of the surveillance, epidemiologic, and end results database. J Clin Oncol Off J Am Soc Clin Oncol. (2006) 24:4539–44. doi: 10.1200/JCO.2005.04.4859, PMID: 17008692 · doi ↗ · pubmed ↗
- 4Rudin CM Brambilla E Faivre-Finn C Sage J . Small-cell lung cancer. Nat Rev Dis Primer. (2021) 7:3. doi: 10.1038/s 41572-020-00235-0, PMID: 33446664 PMC 8177722 · doi ↗ · pubmed ↗
- 5Horn L Mansfield AS Szczęsna A Havel L Krzakowski M Hochmair MJ . First-line atezolizumab plus chemotherapy in extensive-stage small-cell lung cancer. N Engl J Med. (2018) 379:2220–9. doi: 10.1056/NEJ Moa 1809064, PMID: 30280641 · doi ↗ · pubmed ↗
- 6Paz-Ares L Dvorkin M Chen Y Reinmuth N Hotta K Trukhin D . Durvalumab plus platinum–etoposide versus platinum–etoposide in first-line treatment of extensive-stage small-cell lung cancer (CASPIAN): a randomised, controlled, open-label, phase 3 trial. Lancet. (2019) 394:1929–39. doi: 10.1016/S 0140-6736(19)32222-6, PMID: 31590988 · doi ↗ · pubmed ↗
- 7Nabet BY Hamidi H Lee MC Banchereau R Morris S Adler L . Immune heterogeneity in small-cell lung cancer and vulnerability to immune checkpoint blockade. Cancer Cell. (2024) 42:429–43.e 4. doi: 10.1016/j.ccell.2024.01.010, PMID: 38366589 · doi ↗ · pubmed ↗
- 8Xie M Vuko M Rodriguez-Canales J Zimmermann J Schick M O’Brien C . Molecular classification and biomarkers of outcome with immunotherapy in extensive-stage small-cell lung cancer: Analyses of the CASPIAN phase 3 study. Mol Cancer. (2024) 23:115. doi: 10.1186/s 12943-024-02014-x, PMID: 38811992 PMC 11137956 · doi ↗ · pubmed ↗