Relationships among fertility concerns, fear of cancer recurrence, social support, self-efficacy, and family resilience among Chinese adolescents and young adults with cancer: A structural equation modeling
YuQiao Xiao, Can Gu, Li Liu, XiaoRou Zeng

TL;DR
This study explores how fertility concerns and fear of cancer recurrence affect family resilience in young cancer patients, showing that social support and self-efficacy can help reduce these negative effects.
Contribution
The study introduces a structural equation model to clarify the interplay between psychosocial factors and family resilience in Chinese adolescents and young adults with cancer.
Findings
Fertility concerns and fear of recurrence negatively impact family resilience.
Social support and self-efficacy positively influence family resilience.
Social support and self-efficacy partially mediate the negative effects of fertility concerns and fear of recurrence.
Abstract
Fertility concerns, fear of cancer recurrence, social support, and self-efficacy are key factors that influence family resilience in adolescents and young adults with cancer. However, their combined effects and underlying mechanisms remain unclear. This study constructed a structural equation model to examine these relationships and provide evidence for the development of targeted psychosocial interventions in clinical practice. A cross-sectional survey was conducted from April 2024 to March 2025 using convenience sampling of 259 adolescents and young adults with cancer at a tertiary-level specialized cancer hospital in Hunan Province. All the participants completed validated measures of fertility concerns, fear of cancer recurrence, social support, self-efficacy, and family resilience. A structural equation model was constructed using the AMOS software to test the hypothesized…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
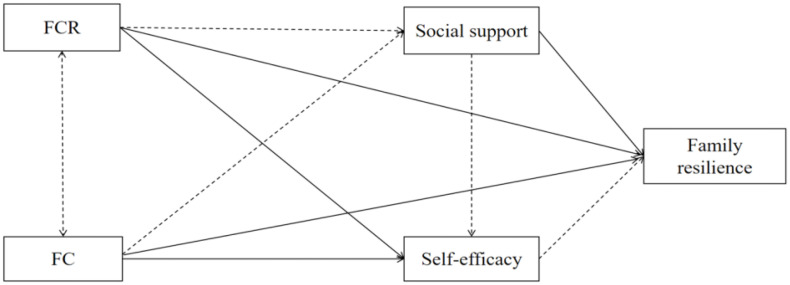 Fig 1
Fig 1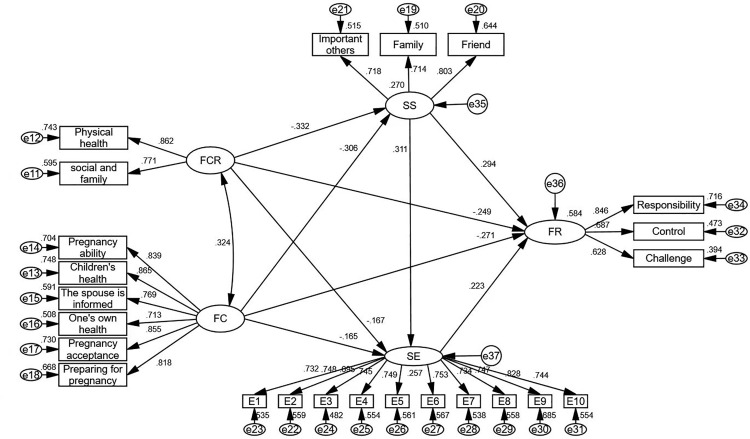 Fig 2
Fig 2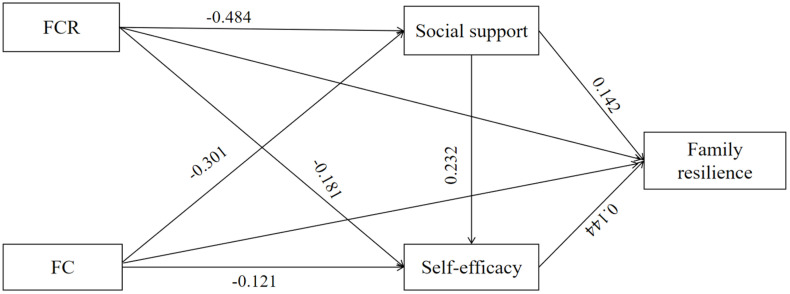 Fig 3
Fig 3- —the National Natural Science Foundation of China
- —the China Medical Board Open Competition Program
- —the Chinese Medical Foundation Project
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive Biology and Fertility · Childhood Cancer Survivors' Quality of Life · Family Support in Illness
Introduction
According to Global Burden of Disease data, cancer is the fourth leading cause of death among adolescents and young adults (AYAs), with approximately 40,380 new cases diagnosed annually in China, ranking it second worldwide in disease burden [1]. Advances in early screening and cancer treatment have enabled more AYAs to achieve long-term survival [2,3]. However, this population is at a unique developmental stage and faces challenges regarding education, career development, intimate relationships, and family planning. Compared to children or older adults, AYAs carry a heavier psychosocial burden. Family serves as the primary source of material and emotional support, and family functioning directly shapes a patient’s ability to adapt to illness and long-term psychosocial outcomes. Family resilience (FR), defined as the ability of family members to adapt, reorganize, and grow together in the face of adversity, plays a vital role in supporting AYAs [4]. Higher FR has been shown to help cancer patients and their families maintain emotional stability, improve treatment adherence, and enhance the quality of life [4,5].
Among the many factors influencing FR, fertility concerns (FC) are particularly salient in AYAs [6]. Standard treatments such as surgery, radiotherapy, and chemotherapy often cause reproductive and gonadal toxicity, imposing heavy burdens on patients’ identity, intimate relationships, and future family roles [7–10]. Fear of cancer recurrence (FCR) is defined as persistent worry about disease progression or relapse and is a common negative emotion [11]. Previous research suggests a strong co-occurrence between FC and FCR; fertility-related decisions may trigger recurrent fears, while high levels of FCR can intensify fertility distress [12]. This intertwined psychological dilemma not only impairs individual adaptation but also undermines family functioning [13–15].
Protective resources are crucial to buffer these adverse effects. According to the Family Adjustment and Adaptation Response (FAAR) model, external resources, such as social support (SS), and internal resources, such as self-efficacy (SE), significantly reduce illness-related stress. Higher perceived SS enhances coping capacity, while SE improves self-care and emotional regulation; together, they promote family functioning and adaptation [14–16]. Although previous studies have identified SS and SE as important predictors of FR, their mediating roles in the relationships among FC, FCR, and FR remain insufficiently explored.
Despite the growing attention being paid to FR, existing research has largely focused on single psychological variables, with limited exploration of how multiple factors interact to influence resilience. In Chinese culture, where reproduction and family roles are highly valued, AYAs may face amplified challenges; however, empirical evidence is still lacking. Furthermore, few studies have applied structural equation modeling (SEM) to test these complex pathways. Therefore, this study aimed to construct and validate a SEM based on the FAAR model to examine the mechanisms linking FC, FCR, SS, and SE to FR. We propose the following hypotheses: (a) FC and FCR are positively correlated; (b) both factors negatively influence FR; and (c) SS and SE mediate the relationships between FC, FCR, and FR (Fig 1).
Research concept hypothesis diagram.
Method
Patients and settings
Adolescent and young adult cancer patients who met the inclusion criteria were recruited from April 2024 to March 2025 at a tertiary care hospital specializing in oncology in Hunan Province, China. The inclusion criteria were as follows: (a) female cancer patients aged 15–39 years, (b) conscious and able to cooperate with the investigation, and (c) those who voluntarily participated in this study and provided informed consent. The exclusion criteria were as follows: (a) patients with other comorbid diseases or cancers, (b) those with primary infertility, and (c) those with impaired verbal communication or slurred speech.
Ethical considerations
All procedures were conducted in accordance with the Declaration of Helsinki of the World Medical Association and approved by the ethics committee of the investigator’s institution (Reference: E202430). Written informed consent was obtained from all participants prior to data collection. For participants under the age of 18, written consent was obtained from a parent or legal guardian in accordance with the ethical requirements.
Measures
General information questionnaire.
A self-designed general information questionnaire was used to collect demographic and clinical data. These included demographic details, disease-related information, and fertility information.
Fear of Progression Questionnaire-Short Form (FOP-Q-SF).
Mehnert et al. [17] developed the FOP-Q-SF to measure fear of disease recurrence or progression in patients with cancer and chronic diseases. Mahendran et al. [18] adapted a Chinese version to evaluate the level of cancer-related fear among cancer survivors. The scale consists of 12 items, using a 5-point Likert scale, with total scores ranging from 12 to 60. The Cronbach’s α coefficient of the scale was 0.87.
Reproductive Concerns After Cancer scale (RCAC).
The RCAC was developed by Gorman et al. [19] to assess issues related to fertility and parenting among young adult female cancer survivors. The Chinese version of the scale was adapted from Qiao et al. [20]. The scale consists of six dimensions, with three items in each dimension. The Cronbach’s α coefficient for the scale was 0.792.
Multidimensional Scale of Perceived Social Support (MSPSS).
The MSPSS was developed by Zimet et al. [21] in 1988 and consists of three dimensions and 12 entries for friends, family, and significant others on a 7-point Likert scale with a total score range of 12–84. Scores of 12–36 indicates low, 37–60 indicates a moderate level of support, and 61–84 indicates a high level of support, scale was 0.890.
General Self-Efficacy Scale (GSES).
The General Self-Efficacy Scale (GSES) was originally developed by Schwarzer and Jerusalem [22] to assess individuals’ perceived ability to cope with a variety of challenging situations. The scale consists of 10 items and adopts a 4-point Likert response format, with higher scores indicating greater self-efficacy. The Chinese version of the GSES has demonstrated good internal consistency and validity across different samples, with reported Cronbach’s α coefficients ranging from 0.75 to 0.91 [23].
Family Hardiness Index (FHI).
The FHI was originally compiled by McCubbin et al. [24]. The Chinese version of the scale was translated, culturally adapted, and psychometrically validated by Liu et al. [25]. The scale has 20 items categorized into three dimensions: responsibility, control, and challenge. The total score ranges from 20 to 80, with higher scores indicating higher levels of family resilience. The scale demonstrated good reliability, with an overall Cronbach’s α of 0.803.
Data collection
The study was conducted across five gynecological oncology wards, three breast wards, and one hematology ward, with the approval of the relevant institutions. The data collection process involved gathering sociodemographic information and patient responses to the three scales and extracting clinical data from medical records to ensure the integrity of the study. A research team was established before the formal survey began and standardized training was provided to all team members to ensure consistency. The questionnaire was administered in two formats: a paper questionnaire and an online questionnaire called Questionnaire Star. Patients first completed the paper questionnaire, which was then double-checked by two researchers before entering the Questionnaire Star system to identify invalid responses. A total of 280 questionnaires were distributed, and 21 invalid questionnaires were excluded, resulting in 259 valid responses. The actual recovery rate was 92.5%.
Data analysis
We used the SPSS software (version 28.0) to analyze the data and calculate the frequencies, means, percentages, and standard deviations to characterize the sample. Pearson’s correlation coefficient was used to determine the relationships between the variables. Before conducting SEM, preliminary data screening was performed to assess the key statistical assumptions. Univariate normality was evaluated using skewness and kurtosis statistics, multivariate outliers were examined using Mahalanobis distance, and multicollinearity was assessed using variance inflation factor values. Minimal missing data were handled using full-information maximum likelihood. To assess potential common method bias, Harman’s single-factor test was conducted by entering all measurement items into an unrotated exploratory factor analysis. Confirmatory factor analysis was conducted to evaluate the measurement properties of the latent constructs, including FC, FCR, SS, SE, and FHI, by assessing factor loadings, internal consistency reliability, convergent validity, and discriminant validity. Subsequently, SPSS AMOS 24.0, was used to construct the structural model with FC, FCR, social support, self-efficacy, and FHI as latent variables and their corresponding items as observed indicators. Model fit was evaluated using multiple goodness-of-fit indices, including the goodness-of-fit index (GFI), the chi-square to degrees of freedom ratio (χ²/df), the root mean square error of approximation (RMSEA), the comparative fit index (CFI), and the incremental fit index. Direct, indirect, and total effects were estimated using SEM, and the bias-corrected bootstrap method with 5,000 re-samples was applied to test the significance of the mediating effects. A mediating effect was considered significant if the 95% bias-corrected confidence interval did not include zero [26]. In all analyses, a p-value < 0.05 was considered statistically significant.
Results
Participant characteristics
A total of 259 AYA cancer patients were investigated in this study, of which 147(56.8%) were under 28, 112 (43.2%) were over 29, 20 had a family history and 239 (92.2%) did not; 167 (64.5%) were married, 78 (30.1%) were unmarried, and 14 (5.4%) were divorced. The other general statistics are presented in Table 1.
Table 1: The participants’ general demographic and characteristics (N = 259).
Assessment of common method bias
The results of Harman’s single-factor test indicated that the first unrotated factor accounted for less than 50% of the total variance, suggesting that common method bias was not a serious concern.
Relationships between fertility concerns, fear of cancer recurrence, social support, self-efficacy, and family resilience
Correlation analyses revealed that fertility concerns (r = –0.474, p < .001) and fear of cancer recurrence (r = –0.431, p < .001) were both significantly negatively correlated with family resilience. Social support (r = .486, p < .001) and self-efficacy (r = .468, p < .001) were positively correlated with family resilience. Further details are presented in Table 2. details.
Table 2: Correlations among fertility concerns, fear of cancer recurrence, social support, self-efficacy, and family resilience(N = 259).
Structural equation modeling of AYAs cancer patients
We constructed a structural equation model for AYAs with cancer. We hypothesized that fertility concerns and fear of cancer recurrence are exogenous variables, and social support, self-efficacy, and family resilience are endogenous variables. The results showed that all goodness of fits met the applicable index criteria (x2/df = 1.335; GFI = 0.908; RMSEA = 0.036; NFI = 0.912; TLI = 0.973; CFI = 0.976). This indicates that the structural equation model developed in this study fit well with the study data, as shown in Table 3 and Fig 2.
Table 3: Goodness-of-fit indices for structural equation modeling of AYAs cancer patients (N = 259).
Structural equation modeling of AYAs cancer patients.
Path analysis showed that FC had a negative effect on social support (β = −0.306, P < 0.001) and SE (β = −0.165, P < 0.05). FCR had a negative effect on SS (β = −0.332, P < 0.001) and self-efficacy (β = −0.167, P < 0.05). SS and SE positively influenced each other (β = 0.311, P < 0.001). SS (β = 0.294, P < 0.001) and SE (β = 0.233, P < 0.01) were positive influences on FR. Further details are presented in Table 4. details.
Table 4: Path analysis table for structural equation modeling of AYAs cancer patients.
Chain-mediated effects of social support and self-efficacy
Mediation results showed that SS and SE played significant chain-mediated roles in FC, FCR, and FR. In particular, the effect value for mediating Effect 1 (FC-SS-SE-FR) was −0.023 (SE = 0.012, p = 0.004), and the effect value for mediating Effect 2 (FCR-SS-SE-FR) was −0.021 (SE = 0.011, p = 0.005). Further details are provided in Table 5 and Fig 3.
Table 5: Chain-mediated effects of social support and self-efficacy.
Research hypothesis verification diagram.
Discussion
This study assessed the correlations among FC, FCR, SS, SE, and FR using structural equation modeling to validate the potential mediation among these factors. The results indicated that FC and FCR were significantly and negatively associated with FR, with SS and SE serving as mediators.
This study found a significant positive correlation between FC and FCR, which is consistent with previous findings. This result may be due to the fact that, when facing a major health crisis such as a cancer diagnosis, AYAs cancer patients reassess their self-worth and the value of life after going through a cancer diagnosis and treatment. They must continually overcome the tremendous shock of cancer diagnosis and adapt to the changes in their bodies [27,28]. The inevitable damage to fertility caused by cancer diagnosis and treatment methods may lead to a sense of resource plundering, particularly among young women, resulting in a pessimistic perception of fertility loss [12]. Influenced by traditional concepts, women are often expected to assume more reproductive roles within their family [10]. Additionally, AYA are at a critical stage of personal development. Due to the economic downturn and the unique social “inward spiral” in China, they must navigate the transformation of their social roles while constantly balancing career development, self-improvement, and family expectations. Consequently, when patients face both the threat of death from cancer and fertility issues, they often struggle to manage the relationship between survival and fertility, viewing them as contradictory and finding it difficult to maintain a balance in their decision-making processes [3,7].
The main findings of this study confirmed the chain-mediated roles of SS and SE. Specifically, excessive FC and FCR diminished patients’ perceived SS and SE. This reduction, in turn, negatively impacts their FR level and adversely affects their physical and mental health, as well as the quality of life of both patients and their family members. This is consistent with Lazarus’s theory of stress and coping, which states that when faced with a major crisis, individuals mobilize both internal and external resources to assess and cope with the stressor [29]. When stress is too high, it can weaken their resources and coping strategies, which in turn affect the outcomes of their physical, mental, and social dimensions of adaptation [29–31]. The results of the SEM pathway confirmed that SS and SE, as external and internal resources for individuals, can significantly alleviate the negative psychological burdens of FC and FCR. Previous studies have shown that a strong social support system can effectively alleviate negative psychological experiences in patients with cancer [32,33]. This enhances their ability to cope with crises, thereby increasing their confidence and sense of control in managing such events. This finding is consistent with the results of the present study. This suggests that in actual clinical intervention practice, the importance of social support and psychosocial outcomes for patients should be emphasized.
In addition, we found that peer support was important for AYAs with cancer. Peer support was the social support dimension with the highest scores. This may be because, under the influence of our traditional culture, young patients believe that reporting good news is a sign of filial piety and love for their parents. They tend to rely heavily on their families after an immediate illness but are reluctant to fully expose their vulnerabilities and sadness to their families in the early stages of the disease, which is not conducive to the overall resilience of the patient and their family. Therefore, friends provide vital spiritual support for patients with cancer. Pain associated with cancer diagnosis, treatment, and the disease itself often requires patients to invest more time and energy to cope with stress. This increased burden can lead to a decrease in social interactions and changes in friendships, which negatively impacts the physical and mental health of patients with cancer [34]. This suggests that we should pay attention to the significant role of peer support for AYA cancer patients, as well as the emotional changes and negative psychological burdens they experience. We can implement interventions such as lectures or live broadcasting classes, inviting patients of the same age during the recovery period to share inspirational stories about their fight against the disease. This approach provides strong informational support and emotional value, enhances self-efficacy in coping with illness, and strengthens family resilience.
Limitations
Although this study confirmed the mediating role of social support and self-efficacy in the family resilience of cancer patients facing a major crisis by constructing a structural equation model, there are still some limitations. First, although this study defined a group of AYAs with cancer, the actual percentage of young patients with cancer was larger because data collection was conducted in only one hospital. Second, all data collected in this study were related to female patients with cancer, which might limit the general applicability of this research. Male cancer patients can also be included to explore the differences in the influence of related variables under different sexes, with the aim of enriching the research results further.
Furthermore, although statistical tests indicated no significant common method bias, the study relied entirely on self-reported measures, which may have introduced potential common method and reporting biases. Finally, this was a cross-sectional study, which could not interpret the dynamics of these variables, and the mediated outcomes need to be treated with caution. Therefore, in the future, we recommend a multicenter longitudinal study to better confirm the causal relationship between these variables.
Conclusion
Perceiving strong social support and a powerful sense of self-efficacy are effective ways to help cancer patients cope with the fear of cancer recurrence and fertility concerns and enhance the resilience of their families. This suggests that, in future clinical work, the levels of social support and self-efficacy of patients should be identified early, effective intervention approaches should be established, and buffer pathways should be provided to patients to help them cope better with major crisis events.
Supporting information
S1 DataDataset.(XLSX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024;74(3):229–63. doi: 10.3322/caac.21834 38572751 · doi ↗ · pubmed ↗
- 2Triarico S, Capozza MA, Mastrangelo S, AttinàG, Maurizi P, Ruggiero A. Gynecological cancer among adolescents and young adults (AYA). Ann Transl Med. 2020;8(6):397. doi: 10.21037/atm.2020.02.41 32355841 PMC 7186636 · doi ↗ · pubmed ↗
- 3Mulder RL, Font-Gonzalez A, Hudson MM, van Santen HM, Loeffen EAH, Burns KC, et al. Fertility preservation for female patients with childhood, adolescent, and young adult cancer: recommendations from the Pan Care LIFE Consortium and the International Late Effects of Childhood Cancer Guideline Harmonization Group. Lancet Oncol. 2021;22(2):e 45–56. doi: 10.1016/S 1470-2045(20)30594-5 33539753 · doi ↗ · pubmed ↗
- 4Shao M, Yang H, Du R, Zhang M, Zhu J, Zhang H, et al. Family resilience in cancer treatment and key influencing factors: a systematic review. Eur J Oncol Nurs. 2023;66:102403. doi: 10.1016/j.ejon.2023.102403 37690311 · doi ↗ · pubmed ↗
- 5Cui P, Shi J, Li S, Getu MA, Wang R, Chen C. Family resilience and its influencing factors among advanced cancer patients and their family caregivers: a multilevel modeling analysis. BMC Cancer. 2023;23(1):623. doi: 10.1186/s 12885-023-11101-z 37403053 PMC 10320962 · doi ↗ · pubmed ↗
- 6Gorman JR, Lyons KS, Harvey SM, Acquati C, Salsman JM, Kashy DA, et al. Opening the conversation: study protocol for a Phase III trial to evaluate a couple-based intervention to reduce reproductive and sexual distress among young adult breast and gynecologic cancer survivor couples. Trials. 2022;23(1):730. doi: 10.1186/s 13063-022-06665-3 36056413 PMC 9438271 · doi ↗ · pubmed ↗
- 7Jardim FA, Lopes-Júnior LC, Nascimento LC, Neves ET, de Lima RAG. Fertility-related concerns and uncertainties in adolescent and young adult childhood cancer survivors. J Adolesc Young Adult Oncol. 2021;10(1):85–91. doi: 10.1089/jayao.2020.0058 32945713 · doi ↗ · pubmed ↗
- 8Gorman JR, Su HI, Roberts SC, Dominick SA, Malcarne VL. Experiencing reproductive concerns as a female cancer survivor is associated with depression. Cancer. 2015;121(6):935–42. doi: 10.1002/cncr.29133 25377593 PMC 4352116 · doi ↗ · pubmed ↗