The association between long-term opioid therapy and composite infection-related dental outcomes
Anne C. Black, Kirsha S. Gordon, James D. Dziura, Declan T. Barry, Stephen Crystal, E. Jennifer Edelman, Gretchen Gibson, Michelle Hamilton, Marianne Jurasic, Yu Li, Brandon D.L. Marshall, Melissa Skanderson, Katie Suda, William C. Becker, Kimberly Page, Kimberly Page

TL;DR
Long-term opioid therapy is linked to higher risk of dental infections in veterans, but results vary with dental coverage.
Contribution
This study identifies a potential class-wide adverse effect of long-term opioid therapy on dental health in a large national cohort.
Findings
LTOT was associated with increased risk of composite infection-related dental outcomes.
Patients with full dental coverage had higher CIDO rates but no significant LTOT association.
Results suggest unique vulnerability among veterans with full dental coverage.
Abstract
The Food and Drug Administration’s warning that transmucosal buprenorphine, a partial opioid agonist used to treat opioid use disorder and chronic pain, may cause dental disease opens questions about potential class-wide adverse effects involving more widely prescribed opioid analgesics. This was a retrospective matched national cohort study of patients in care at the Department of Veterans Affairs (VA) between October 2010-September 2019. Patients prescribed LTOT were matched 1:2 to patients not prescribed LTOT on age, sex, service region, and VA dental coverage. Cox regression models estimated the association between LTOT and a composite infection-related dental outcome (CIDO). Sensitivity analyses excluded patients with cancer, restricted to patients with comprehensive dental coverage, and to patients with ≥180 days of follow-up time, respectively. The cohort comprised 2,173,435…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
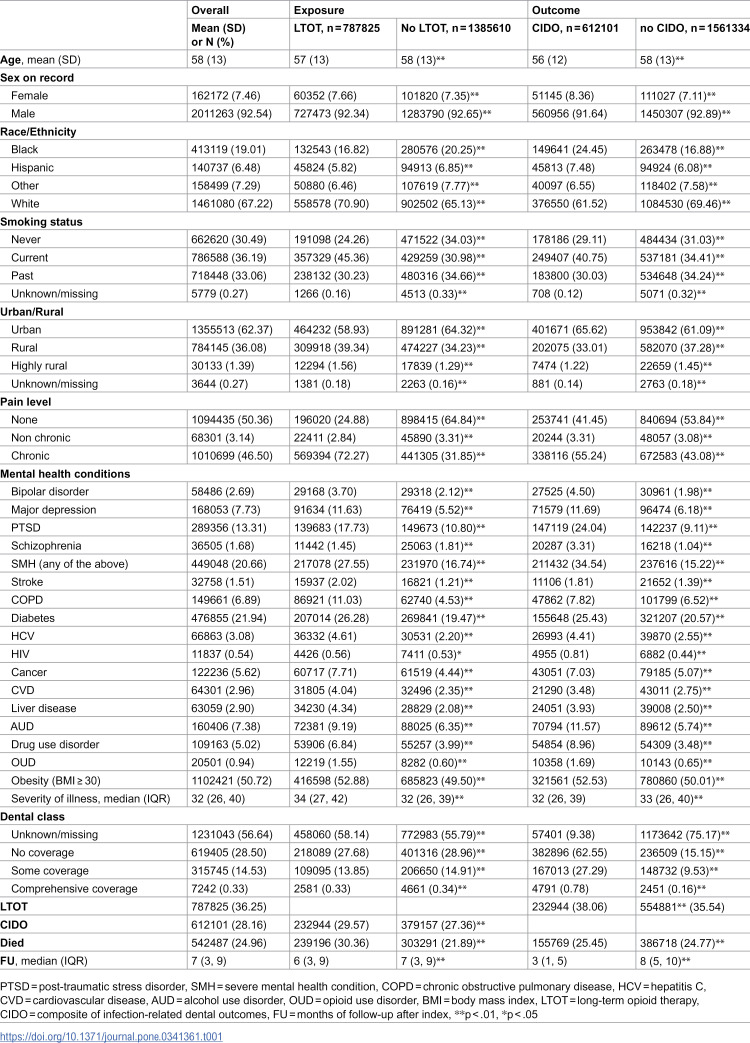 Figure 1
Figure 1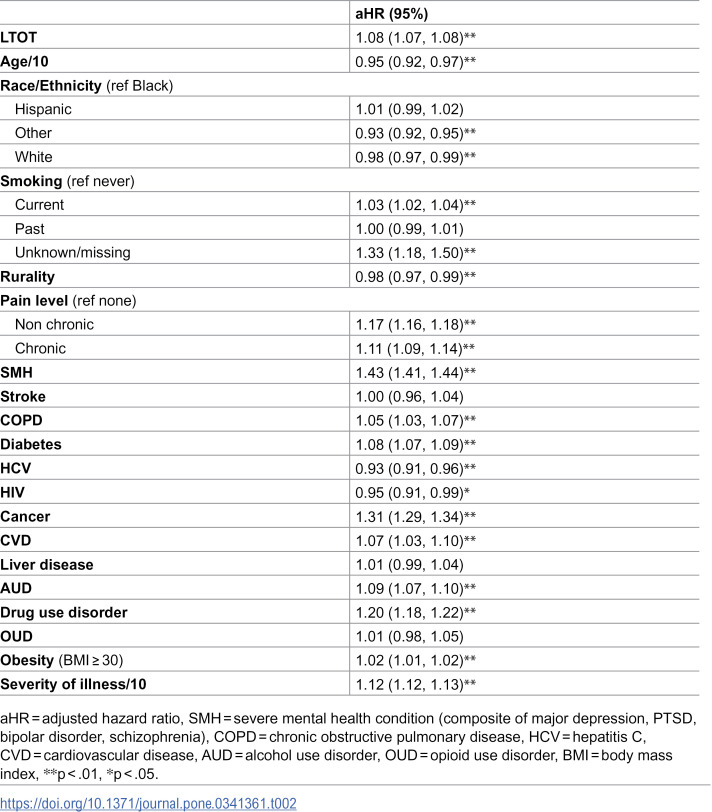 Figure 2
Figure 2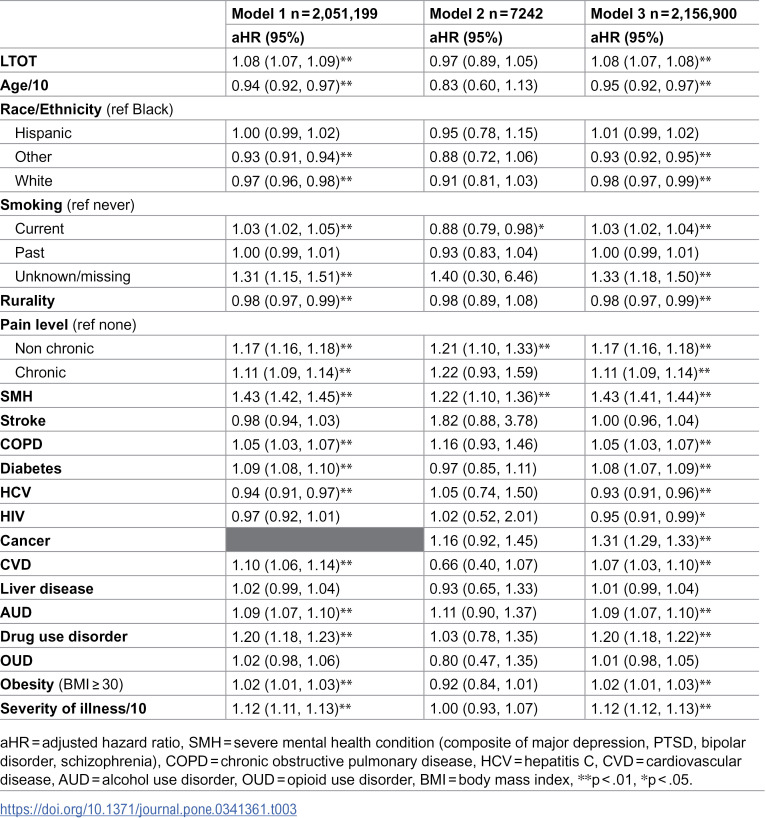 Figure 3
Figure 3- —http://dx.doi.org/10.13039/100000027National Institute on Alcohol Abuse and Alcoholism
- —http://dx.doi.org/10.13039/100000027National Institute on Alcohol Abuse and Alcoholism
- —http://dx.doi.org/10.13039/100000026National Institute on Drug Abuse
- —http://dx.doi.org/10.13039/100000027National Institute on Alcohol Abuse and Alcoholism
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOpioid Use Disorder Treatment · HIV, Drug Use, Sexual Risk · Forensic Toxicology and Drug Analysis
Introduction
Clinical guidelines for chronic pain management de-emphasize use of long-term full-opioid agonist therapy (LTOT), such as oxycodone and hydrocodone, given risks for opioid-related harms including opioid use disorder (OUD) and equivocal evidence for long-term effectiveness [1,2]. For individuals prescribed LTOT with evidence of OUD, guidelines recommend transition to buprenorphine [3], a partial opioid agonist with analgesic effects and well-established effectiveness for OUD management. Transition to buprenorphine is preferred to drastic reduction or discontinuation of LTOT given the associated high risk for overdose and death [4]. However, in 2022, the Food and Drug Administration [5] published a warning about dental problems associated with transmucosal buprenorphine (e.g., Suboxone, a sublingual buprenorphine/naloxone film), the commonly prescribed buprenorphine formulation, citing risks of tooth decay, cavities, oral infections, and tooth loss. Concern over these risks may present a barrier to buprenorphine initiation in patients prescribed LTOT for whom such treatment is indicated. However, full opioid agonists themselves may pose oral health risks due to immunosuppression and well-documented effects on saliva flow causing xerostomia; both create opportunity for oral disease development [6,7]. Nevertheless, to our knowledge, no published studies have specifically addressed the dental risks of LTOT. The goal of the current study was to assess the effect of LTOT exposure on dental disease development in a retrospective cohort of patients receiving care within the Department of Veterans Affairs (VA).
Methods
This study was conducted under waiver of informed consent with approval by the VA Connecticut Healthcare System Research and Development Committee and Yale University Human Investigation Committee. Data were accessed for this study between January 24, 2024-March 28, 2025. Authors with IRB-approved access to the data (ACB, KSG, MS, WCB) had access to information that could identify individual participants during and after the data access period.
Using a national cohort curated by the Veterans Aging Cohort Study (VACS), we created a matched cohort of patients who received VA primary care between October 1, 2010-September 30, 2019 (i.e., fiscal years [FY] 2011–2019) and had not experienced the primary outcome in the year prior to cohort entry. The dataset included all administrative, pharmacy, and healthcare data in VA electronic health records (EHR) for the study period. LTOT prescription was defined as ≥ 90 consecutive days, allowing for 30-day refill gaps, of hydrocodone, oxycodone, morphine, fentanyl, hydromorphone, dihydrocodeine, meperidine, pentazocine, propoxyphene, levorphanol, tramadol, or tapentadol (excluding methadone) [8]. Patients with incident LTOT exposure, with no exposure to LTOT in the prior year were matched 1:2 to patients not prescribed LTOT. Matching variables included age (in 5-year increments), sex, VA service region, and category of VA dental coverage (i.e., unknown/missing, no, some, or comprehensive coverage). The index date for LTOT-exposed patients was the day of LTOT initiation, and for those not LTOT-exposed, was the first VA visit date within the same FY as matched LTOT-exposed patients. The baseline period was 12 months prior to index date, during which patient characteristics were ascertained.
The primary outcome was the composite infection-related dental outcome (CIDO), a dichotomous indicator of any new (i.e., post-baseline) diagnosis of dental caries, oral infections, or tooth loss according to International Classification of Diseases (ICD) and Current Procedural Terminology codes adjudicated by dental expert coauthors (GG, MH, MJ, KS; Table in S1 Table).
We calculated descriptive statistics for the cohort overall and by LTOT exposure and outcome. Group differences were assessed by chi-square, t-tests, or Wilcoxon signed-rank tests. We used Cox proportional hazards modeling, accounting for matching, to estimate the unconditional effect of LTOT exposure on days to first recorded CIDO, death, or end of study. We then estimated a multivariable Cox model, adjusting for age at index date and baseline-recorded sex, race/ethnicity (Black, Hispanic, White, or other), smoking status (never, unknown, current, past), rurality of home address (rural/highly rural vs. not), pain level (none, non-chronic, or chronic, based on pain-related diagnosis), serious mental health condition (major depressive disorder, post-traumatic stress disorder, bipolar disorder, schizophrenia), medical conditions (cancer, chronic obstructive pulmonary disease, stroke, diabetes, human immunodeficiency virus [HIV], hepatitis C [HCV], cardiovascular disease, liver disease), substance use (alcohol use disorder, non-opioid drug use disorder, opioid use disorder), obesity (body mass index ≥30) [9], and overall illness severity (measured by the VACS index) [10]. Patients with incomplete data and those who died during the baseline period were excluded. Pain, mental health, and medical conditions were determined by ICD codes.
We conducted several sensitivity analyses to test for stability in model estimates: (1) excluding patients with cancer who may be uniquely vulnerable to infection, (2) restricting to patients with comprehensive VA dental coverage provided for service-connected dental disability or other disabling medical condition [11,12] who may be particularly vulnerable to infection and whose dental care records may be differentially available in the VA EHR, and (3) restricting to patients with ≥180 days of follow-up time to standardize the time at risk for CIDO.
Results
The cohort, comprising 2,173,435 patients, was predominantly male (92%) and White (67%), consistent with the VA patient population. The majority smoked or had smoked (69%), 38% lived in a rural setting, and approximately half had obesity (51%) and chronic pain (46%; Table 1). Consistent with the 1:2 matching schema, approximately one-third (36%) were prescribed LTOT. A total of 28% experienced CIDO.
Table 1: Patients in care FY 2010-2019 characteristics, n = 2,173,435.
Relative to patients not prescribed LTOT, those prescribed LTOT were more likely to be White, smoke currently, live in a rural setting, have chronic pain, a serious mental health condition (except schizophrenia), substance use disorder, greater illness severity, and experience CIDO. Although statistically significant, differences in VA dental coverage were negligible due to matching (Table 1).
Patients with CIDO, compared to those without, were more likely to be female, Black, smoke currently, reside in a non-rural setting, have chronic pain, a serious mental health condition, substance use disorder, VA dental coverage, and receive LTOT.
In the simple Cox model, being prescribed LTOT was associated with greater risk of CIDO compared to having no prescribed LTOT; hazard ratio (HR) (95% CI) = 1.24 (1.23, 1.25). Adjusting for covariates, the risk associated with LTOT was attenuated but remained statistically significant; adjusted hazard ratio (aHR) (95% CI) = 1.08 (1.07, 1.08).
Covariates associated with greater risk for CIDO included having a pain-related diagnosis, serious mental health condition, cancer diagnosis, substance use disorder, and higher illness severity. In contrast, increased age, White or other race (compared to Black), rural residence, HCV, and HIV were associated with lower CIDO risk (Table 2).
Table 2: Multivariable Cox proportional hazards model of CIDO, n = 2,173,435.
In individual sensitivity analyses limited to patients without cancer, and to those with at least 180 days of follow-up, respectively, results essentially replicated the multivariable full-cohort model’s; aHR (95% CI) = 1.08 (1.07, 1.09) (Table 3). In contrast, among patients with comprehensive VA dental coverage, whose CIDO rates were substantially higher than among the cohort overall, there was no association between CIDO and LTOT; aHR (95% CI) = 0.97 (0.89, 1.05).
Table 3: Sensitivity analyses: Model 1 excluded those with cancer, Model 2 restricted to those with comprehensive dental coverage, Model 3 restricted to those with index date ≥180 days prior to end of study.
Discussion
To our knowledge, this is the first study to demonstrate the association between LTOT exposure and dental disease. This finding is important in light of recent warnings of buprenorphine risks that may influence decision-making in the context of chronic pain and/or OUD. Evidence of LTOT-associated dental risks may inform clinical guidelines for LTOT prescribing, including recommendations for specific monitoring of patients’ oral health, attention to oral healthcare while taking LTOT, and patient-provider discussions of dental risks before initiating LTOT. However, several study limitations should be considered when interpreting study results, including the risk for confounding by indication. Specifically, despite our effort to control for covariates of LTOT prescribing including substance use and medical comorbidities, unmeasured confounders may have driven observed associations attributed to LTOT. Secondly, the study was limited by our use of available data in patients’ EHR. Patients without VA dental coverage may have CIDO recorded in other systems not reviewed in the current study, posing risk for access-related ascertainment bias. However, given our matching paradigm, outcome misclassification likely would not differ by LTOT status. Whereas in this study we controlled for substance use disorders, future research is needed to account for the unique oral health-related risks of specific substance use in the context of LTOT exposure. Further, as conditions comprising CIDO (e.g., oral infection, tooth loss) differ in etiology and clinical course, our use of a composite outcome may mask mechanism-specific associations. Thus, future research on this topic should assess effects of LTOT on individual CIDO conditions. Sensitivity analyses suggested LTOT may pose minimal additional risk to patients already vulnerable to dental infection, such as patients provided VA comprehensive dental coverage. However, smaller sample size in that analysis may have masked differences in CIDO rate. Finally, given the study’s focus on a patient sample receiving services within the VA, results may not generalize to a broader population of patients. Despite these limitations, the demonstrated association between incident LTOT exposure and new diagnosis of dental disease in this rigorous, large-sample analysis exposes the need for additional study. To inform the critical decision to transition from LTOT to buprenorphine to address OUD, research is needed to assess the relative oral health risks of these medications.
Supporting information
S1 TableCurrent dental terminology (CDT) and international classification of diseases (ICD) codes for the composite of infection-related dental outcomes (CIDO), a composite of dental caries, oral infections, and loss of teeth.(DOCX)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Department of Veterans Affairs. VA/Do D clinical practice guideline for the use of opioids in the management of chronic pain. 2024. https://www.healthquality.va.gov/guidelines/pain/cot/
- 2Dowell D, Ragan KR, Jones CM, Baldwin GT, Chou R. CDC Clinical Practice Guideline for Prescribing Opioids for Pain - United States, 2022. MMWR Recomm Rep. 2022;71(3):1–95. doi: 10.15585/mmwr.rr 7103 a 1 36327391 PMC 9639433 · doi ↗ · pubmed ↗
- 3U.S. Department of Health and Human Services. HHS guide for clinicians on the appropriate dosage reduction or discontinuation of long-term opioid analgesics. 2019. https://www.hhs.gov/system/files/Dosage_Reduction_Discontinuation.pdf
- 4Oliva EM, Bowe T, Manhapra A, Kertesz S, Hah JM, Henderson P, et al. Associations between stopping prescriptions for opioids, length of opioid treatment, and overdose or suicide deaths in US veterans: observational evaluation. BMJ. 2020;368:m 283. doi: 10.1136/bmj.m 283 32131996 PMC 7249243 · doi ↗ · pubmed ↗
- 5Knopf A. FDA warns about dental problems with buprenorphine medicines dissolved in the mouth. Child and Adolescent Update. 2022;24(3):8–8. doi: 10.1002/cpu.30656 · doi ↗
- 6Götrick B, Åkerman S, Ericson D, Torstenson R, Tobin G. Oral pilocarpine for treatment of opioid-induced oral dryness in healthy adults. J Dent Res. 2004;83(5):393-–397. doi: 10.1002/cpu.3065615111631 · doi ↗ · pubmed ↗
- 7NinkovićJ, Roy S. Role of the mu-opioid receptor in opioid modulation of immune function. Amino Acids. 2013;45(1):9–24. doi: 10.1007/s 00726-011-1163-0 22170499 PMC 3912755 · doi ↗ · pubmed ↗
- 8Edelman EJ, Gordon K, Becker WC, Goulet JL, Skanderson M, Gaither JR, et al. Receipt of opioid analgesics by HIV-infected and uninfected patients. J Gen Intern Med. 2013;28(1):82–90. doi: 10.1007/s 11606-012-2189-z 22895747 PMC 3539026 · doi ↗ · pubmed ↗