Treatment and Outcomes for Patients With Inadequate Lymphadenectomy After Resection of Stage II Small Bowel Adenocarcinoma
Jackson A. Baril, Karl Y. Bilimoria, Eugene P. Ceppa, Michael G. House, Thomas K. Maatman, Alexandra M. Roch, Anthony D. Yang, C. Max Schmidt, Ryan J. Ellis

TL;DR
The study examines how adjuvant chemotherapy affects survival in patients with stage II small bowel adenocarcinoma who had inadequate lymph node removal, finding benefits only in those with additional high-risk features.
Contribution
This study identifies factors influencing chemotherapy use and shows its survival benefit specifically in high-risk patients with inadequate lymphadenectomy.
Findings
525 out of 1765 patients with inadequate lymphadenectomy received adjuvant chemotherapy.
Adjuvant chemotherapy improved 5-year survival in patients with additional high-risk features but not in those without.
T4 primary, poor tumor grade, and positive resection margin were associated with receiving chemotherapy.
Abstract
Adjuvant chemotherapy (AC) is considered for patients with stage II small bowel adenocarcinoma (SBA) with an inadequate lymphadenectomy; however, the prognostic role of additional high‐risk features (T4 primary, positive resection margin, poorly differentiated tumor, or lymphovascular invasion) is unknown. The objectives were to describe utilization of AC among patients with stage II SBA with inadequate lymphadenectomy, identify factors associated with receipt of AC, and examine the association between AC and survival stratified by presence of additional high‐risk features. Patients with stage II SBA were identified using the National Cancer Database from 2004 to 2021. Inadequate lymphadenectomy was defined < 5 lymph nodes duodenal tumors and < 8 lymph nodes other sites. Of 1765 patients with stage II SBA and an inadequate lymphadenectomy, 525 (29.8%) received AC. T4 primary, poor…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
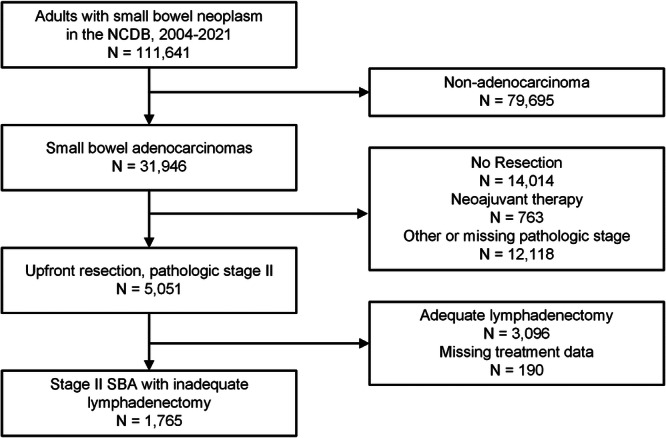 Figure 1
Figure 1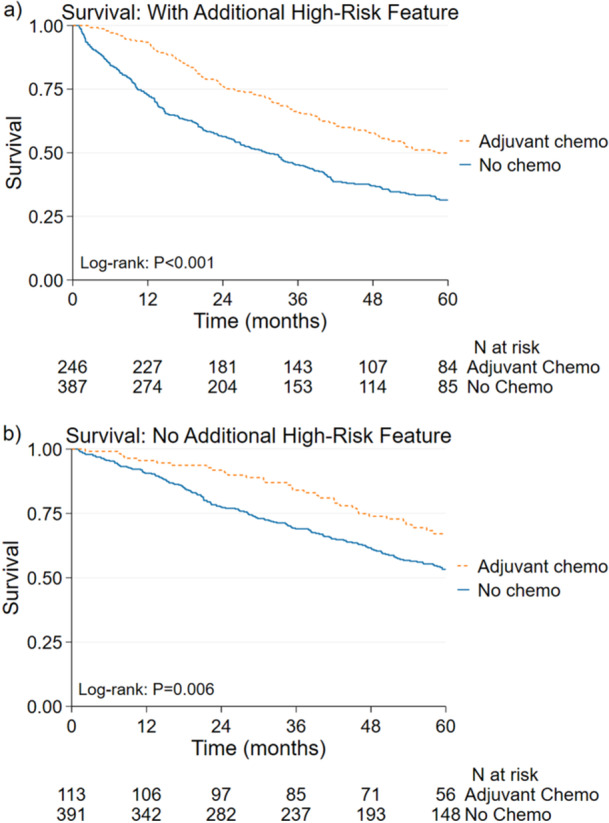 Figure 2
Figure 2|
| Number (%) |
|---|---|
|
| |
| Sex | |
| Female | 815 (46.2) |
| Male | 950 (53.8) |
| Age (yrs) | |
| < 50 | 201 (11.4) |
| 50–59 | 295 (16.7) |
| 60–69 | 456 (25.8) |
| 70–79 | 473 (26.8) |
| 80+ | 340 (19.3) |
| Race and Ethnicity | |
| Non‐Hispanic White | 1224 (69.4) |
| Non‐Hispanic Black | 320 (18.1) |
| Hispanic | 85 (4.8) |
| Asian | 38 (2.2) |
| Other or Unknown | 98 (5.6) |
| Median Household Income | |
| < $46,277 | 272 (15.4) |
| $46,277–$57,856 | 362 (20.5) |
| $57,857–$74,062 | 374 (21.2) |
| $74,063+ | 545 (30.9) |
| Unknown | 212 (12.0) |
| % Local No High School Diploma | |
| < 5% | 330 (18.7) |
| 5.0–9.0% | 475 (26.9) |
| 9.1–15.2% | 438 (24.8) |
| 15.3% and up | 316 (17.9) |
| Unknown | 206 (11.7) |
| Insurance Status | |
| Private Insurance | 570 (32.3) |
| Medicare | 994 (56.3) |
| Uninsured/Medicaid | 148 (8.4) |
| Other or Unknown | 53 (3.0) |
| Charlson–Deyo Score | |
| 0 | 1218 (69.0) |
| 1 | 357 (20.2) |
| 2+ | 190 (10.8) |
| Year of Diagnosis | |
| 2004–2008 | 466 (26.4) |
| 2009–2013 | 513 (29.1) |
| 2014–2018 | 502 (28.4) |
| ≥ 2018 | 284 (16.1) |
| Tumor Location | |
| Duodenum | 350 (19.8) |
| Jejunum | 569 (32.2) |
| Ileum | 274 (15.5) |
| Other, Small Intestine | 572 (32.4) |
| T Stage | |
| 3 | 1057 (59.9) |
| 4 | 630 (35.7) |
| Unknown | 78 (4.4) |
| Lymphovascular Invasion | |
| Absent | 783 (44.4) |
| Present | 293 (16.6) |
| Unknown | 689 (39.0) |
| Histologic Grade | |
| Well | 194 (11.0) |
| Moderate | 1106 (62.7) |
| Poor | 400 (22.7) |
| Unknown | 65 (3.7) |
| Resection Margin | |
| Negative | 1524 (86.4) |
| Positive | 205 (11.6) |
| Unknown or Indeterminate | 36 (2.0) |
|
| |
| Hospital Type | |
| Academic | 535 (30.3) |
| Non‐Academic | 1230 (69.7) |
| Hospital Annual Volume Quartile | |
| Q1 (< 4) | 539 (30.5) |
| Q2 (4–8) | 506 (28.7) |
| Q3 (9–15) | 411 (23.3) |
| Q4 (≥ 16) | 309 (17.5) |
| Hospital Region | |
| New England | 80 (4.5) |
| Middle Atlantic | 284 (16.1) |
| South Atlantic | 429 (24.3) |
| East North Central | 273 (15.5) |
| East South Central | 119 (6.7) |
| West North Central | 127 (7.2) |
| West South Central | 136 (7.7) |
| Mountain | 71 (4.0) |
| Pacific | 184 (10.4) |
| Unknown | 62 (3.5) |
| Receipt of adjuvant chemotherapy (%) | aOR (95% confidence interval) |
| |
|---|---|---|---|
| Patient and Tumor Characteristics | |||
| Sex | |||
| Female | 28.8 | 1 | Ref |
| Male | 30.5 | 1.01 (0.79–1.28) | 0.961 |
| Age (yrs) | |||
| < 50 | 51.7 | 1.11 (0.71–1.76) | 0.644 |
| 50–59 | 44.4 | 1 | Ref |
| 60–69 | 37.3 | 0.73 (0.50–1.06) | 0.100 |
| 70–79 | 21.4 | 0.32 (0.20–0.50) | < 0.001 |
| 80+ | 5.6 | 0.07 (0.04–0.14) | < 0.001 |
| Race and Ethnicity | |||
| Non‐Hispanic White | 29.2 | 1 | Ref |
| Non‐Hispanic Black | 33.4 | 1.05 (0.73–1.50) | 0.800 |
| Hispanic | 29.4 | 0.71 (0.38–1.32) | 0.273 |
| Asian | 29.0 | 0.97 (0.39–2.43) | 0.956 |
| Other or Unknown | 25.5 | 0.93 (0.52–1.68) | 0.822 |
| Median Household Income | |||
| < $46,277 | 29.4 | 1 | Ref |
| $46,277–$57,856 | 26.5 | 0.93 (0.61–1.41) | 0.724 |
| $57,857–$74,062 | 30.5 | 0.86 (0.55–1.32) | 0.487 |
| $74,063+ | 32.1 | 0.73 (0.45–1.19) | 0.210 |
| % Local No High School Diploma | |||
| < 5% | 35.5 | 1 | Ref |
| 5.0–9.0% | 31.1 | 0.83 (0.58–1.20) | 0.323 |
| 9.1–15.2% | 27.4 | 0.65 (0.42–1.01) | 0.056 |
| 15.3% and up | 25.9 | 0.50 (0.30–0.83) | 0.007 |
| Insurance Status | |||
| Private Insurance | 43.3 | 1 | Ref |
| Medicare | 21.4 | 0.95 (0.68–1.34) | 0.775 |
| Uninsured/Medicaid | 37.2 | 0.78 (0.52–1.17) | 0.227 |
| Other/Unknown | 18.9 | 0.50 (0.21–1.15) | 0.103 |
| Charlson–Deyo Score | |||
| 0 | 32.4 | 1 | Ref |
| 1 | 24.7 | 0.82 (0.60–1.14) | 0.235 |
| 2+ | 22.6 | 0.70 (0.45–1.08) | 0.106 |
| Year of Diagnosis | |||
| 2004–2008 | 24.9 | 0.79 (0.47–1.34) | 0.386 |
| 2009–2013 | 27.7 | 0.69 (0.47–1.00) | 0.051 |
| 2014–2018 | 34.1 | 0.92 (0.63–1.34) | 0.659 |
| ≥ 2018 | 33.8 | 1 | Ref |
| Tumor Location | |||
| Duodenum | 24.6 | 1 | Ref |
| Jejunum | 36.6 | 1.37 (0.96–1.93) | 0.080 |
| Ileum | 26.3 | 1.06 (0.71–1.60) | 0.765 |
| Other, Small Intestine | 27.8 | 0.94 (0.66–1.33) | 0.725 |
| T Stage | |||
| 3 | 25.0 | 1 | Ref |
| 4 | 38.3 | 1.96 (1.50–2.57) | < 0.001 |
| Lymphovascular Invasion | |||
| Absent | 30.4 | 1 | Ref |
| Present | 38.9 | 1.15 (0.82–1.62) | 0.410 |
| Histologic Grade | |||
| Well | 24.2 | 0.76 (0.50–1.15) | 0.191 |
| Moderate | 29.0 | 1 | Ref |
| Poor | 35.5 | 1.42 (1.07–1.89) | 0.015 |
| Resection Margin | |||
| Negative | 28.9 | 1 | Ref |
| Positive | 37.1 | 1.62 (1.12–2.35) | 0.011 |
| Unknown or Indeterminate | 25.0 | 1.53 (0.62–3.78) | 0.349 |
| Hospital Characteristics | |||
| Hospital Type | |||
| Academic | 32.0 | 1 | Ref |
| Non‐Academic | 28.8 | 1.00 (0.71–1.41) | 0.989 |
| Hospital Annual Volume Quartile | |||
| Q1 (< 4) | 30.6 | 0.92 (0.59–1.43) | 0.721 |
| Q2 (4–8) | 26.3 | 0.77 (0.51–1.16) | 0.212 |
| Q3 (9–15) | 30.7 | 0.94 (0.66–1.33) | 0.747 |
| Q4 (≥ 16) | 33.7 | 1 | Ref |
| Hospital Region | |||
| New England | 37.5 | 1 | Ref |
| Middle Atlantic | 28.9 | 0.66 (0.36–1.23) | 0.195 |
| South Atlantic | 30.1 | 0.65 (0.37–1.16) | 0.144 |
| East North Central | 27.1 | 0.63 (0.34–1.14) | 0.127 |
| East South Central | 23.5 | 0.45 (0.21–0.93) | 0.031 |
| West North Central | 30.7 | 0.77 (0.40–1.48) | 0.428 |
| West South Central | 26.5 | 0.56 (0.29–1.08) | 0.082 |
| Mountain | 35.2 | 0.96 (0.50–1.87) | 0.912 |
| Pacific | 24.5 | 0.62 (0.33–1.15) | 0.129 |
| With additional high‐risk feature(s) |
| Without additional high‐risk feature |
| |
|---|---|---|---|---|
|
| ||||
| Post‐operative Chemotherapy | ||||
| No | 1 | Ref | 1 | Ref |
| Yes | 0.62 (0.48–0.79) | < 0.001 | 0.83 (0.55–1.24) | 0.363 |
| Sex | ||||
| Female | 0.76 (0.60–0.95) | 0.016 | 1.38 (1.02–1.86) | 0.038 |
| Male | 1 | Ref | 1 | Ref |
| Age (yrs) | ||||
| < 50 | 0.90 (0.54–1.49) | 0.683 | 0.60 (0.29–1.25) | 0.174 |
| 50–59 | 1 | Ref | 1 | Ref |
| 60–69 | 1.18 (0.82–1.71) | 0.372 | 0.94 (0.56–1.57) | 0.805 |
| 70–79 | 1.09 (0.71–1.67) | 0.703 | 1.19 (0.67–2.13) | 0.549 |
| 80+ | 1.60 (1.01–2.53) | 0.046 | 2.33 (1.31–4.18) | 0.004 |
| Race and Ethnicity | ||||
| Non‐Hispanic White | 1 | Ref | 1 | Ref |
| Non‐Hispanic Black | 1.25 (0.90–1.74) | 0.190 | 1.03 (0.69–1.55) | 0.878 |
| Hispanic | 1.40 (0.80–2.45) | 0.233 | 1.19 (0.53–2.69) | 0.669 |
| Asian | 0.82 (0.28–2.40) | 0.721 | 1.30 (0.30–5.67) | 0.724 |
| Other or Unknown | 1.72 (1.14–2.61) | 0.010 | 1.34 (0.70–2.58) | 0.375 |
| Median Household Income | ||||
| < $46,277 | 1 | Ref | 1 | Ref |
| $46,277–$57,856 | 0.82 (0.57–1.28) | 0.441 | 1.11 (0.66‐‐1.89) | 0.684 |
| $57,857–$74,062 | 0.82 (0.54–1.23) | 0.330 | 1.05 (0.61–1.81) | 0.870 |
| $74,063+ | 0.74 (0.48–1.14) | 0.171 | 1.31 (0.72‐2.38) | 0.369 |
| % Local No High School Diploma | ||||
| < 5% | 1 | Ref | 1 | Ref |
| 5.0–9.0% | 0.77 (0.55–1.08) | 0.133 | 0.90 (0.55–1.45) | 0.658 |
| 9.1–15.2% | 0.59 (0.39–0.88) | 0.010 | 1.02 (0.59–1.75) | 0.951 |
| 15.3% and up | 0.0.69 (0.44–1.09) | 0.114 | 0.82 (0.43–1.56) | 0.544 |
| Insurance Status | ||||
| Private Insurance | 1 | Ref | 1 | Ref |
| Medicare | 1.05 (0.75–1.48) | 0.769 | 1.24 (0.80–1.91) | 0.339 |
| Uninsured/Medicaid | 1.38 (0.87–2.17) | 0.167 | 1.89 (1.03–3.46) | 0.039 |
| Other/Unknown | 1.09 (0.54–2.19) | 0.805 | 2.70 (1.12–6.47) | 0.026 |
| Charlson–Deyo Score | ||||
| 0 | 1 | Ref | 1 | Ref |
| 1 | 1.45 (1.11–1.90) | 0.007 | 1.07 (0.74–1.55) | 0.719 |
| 2+ | 2.05 (1.42–2.96) | < 0.001 | 1.43 (0.85–2.43) | 0.181 |
| Year of Diagnosis | ||||
| 2004–2008 | 1.33 (0.76–2.32) | 0.324 | 1.12 (0.58–2.17) | 0.733 |
| 2009–2013 | 1.10 (0.71–1.70) | 0.683 | 0.98 (0.51–1.88) | 0.941 |
| 2014–2018 | 1.08 (0.70–1.67) | 0.718 | 0.91 (0.47–1.80) | 0.795 |
| ≥ 2018 | 1 | Ref | 1 | Ref |
| Tumor Location | ||||
| Duodenum | 1 | Ref | 1 | Ref |
| Jejunum | 0.69 (0.46–1.03) | 0.071 | 0.58 (0.36–0.93) | 0.023 |
| Ileum | 0.97 (0.63–1.50) | 0.899 | 0.67 (0.39–1.15) | 0.149 |
| Other, Small Intestine | 1.13 (0.77–1.66) | 0.519 | 0.97 (0.62–1.51) | 0.889 |
|
| ||||
| Hospital Type | ||||
| Academic | 1 | Ref | 1 | Ref |
| Non‐Academic | 1.16 (0.84–1.60) | 0.379 | 1.48 (0.97–2.26) | 0.067 |
| Hospital Annual Volume Quartile | ||||
| Q1 ( < 4) | 1.02 (0.73–1.42) | 0.899 | 1.20 (0.65–2.19) | 0.564 |
| Q2 (4–8) | 0.94 (0.64–1.38) | 0.765 | 1.42 (0.79–2.52) | 0.238 |
| Q3 (9–15) | 0.90 (0.60–1.35) | 0.599 | 1.01 (0.56–1.82) | 0.964 |
| Q4 ( ≥ 16) | 1 | Ref | 1 | Ref |
| Hospital Region | ||||
| New England | 1 | Ref | 1 | Ref |
| Middle Atlantic | 1.11 (0.61–2.03) | 0.734 | 1.96 (0.74–5.18) | 0.175 |
| South Atlantic | 1.12 (0.61–2.06) | 0.704 | 1.42 (0.55–3.73) | 0.466 |
| East North Central | 0.80 (0.43–1.48) | 0.484 | 2.12 (0.81–5.58) | 0.127 |
| East South Central | 0.87 (0.44‐1.74) | 0.695 | 1.24 (0.42–3.68) | 0.694 |
| West North Central | 1.06 (0.56–2.03) | 0.848 | 2.25 (0.80–6.33) | 0.126 |
| West South Central | 0.92 (0.48–1.78) | 0.814 | 1.56 (0.55‐4.45) | 0.402 |
| Mountain | 1.19 (0.54–2.64) | 0.661 | 1.40 (0.40–4.88) | 0.594 |
| Pacific | 0.74 (0.38–1.43) | 0.365 | 1.42 (0.51–3.98) | 0.503 |
- —Funder National Cancer Institute of the National Institutes of Health (Grant T32CA282070).
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastric Cancer Management and Outcomes · Colorectal Cancer Surgical Treatments
Introduction
1
Small bowel adenocarcinoma (SBA) is rare and accounts for around 1 in 3 small bowel malignancies. SBA has a poor prognosis with a median overall survival (OS) of 12.8 months for duodenal tumors and 40.4 months for jejunal tumors [1, 2, 3]. In 2024, an estimated 12,440 patients will be diagnosed with SBA in the United States and over 2000 will die from the disease [4]. Patients with Crohn Disease, ulcerative colitis, Lynch syndrome, familial adenomatous polyposis, and Celiac disease are at increased risk of developing SBA [5, 6, 7, 8, 9, 10]. SBA rarely is detected on cross‐sectional imaging and may be found incidentally during resections for stricture, bowel obstruction, or fistulizing disease [9, 11]. Without a suspected diagnosis of malignancy, an oncologic resection might not be performed leading to inadequate lymphadenectomy. Due to the rarity of SBA, limited prospective data are available to guide treatment in patients with an early stage primary and inadequate lymphadenectomy and thus some recommendations are extrapolated from colorectal adenocarcinoma data [12]. However, current guidelines for treatment of SBA recommend adjuvant chemotherapy for stage III disease and to consider adjuvant chemotherapy in stage II patients with other high‐risk features such as T4 primary tumor, positive resection margin, poor differentiation, tumor perforation, lymphovascular or perineural invasion, and inadequate lymphadenectomy [13, 14].
According to current guidelines, an inadequate lymphadenectomy is defined as removal of fewer than 5 lymph nodes for duodenal tumors and fewer than 8 lymph nodes for tumors of the ileum or jejunum [14]. Node‐positive disease is known to have worse outcomes, thus adequate staging for treatment sequencing is critical [3, 15, 16]. Studies have suggested varying cutoffs for adequate lymphadenectomy to optimize staging and survival: removal of 5 to 8 lymph nodes for tumors of the duodenum and 8 to 16 lymph nodes for tumors of the jejunum or ileum [17, 18, 19, 20]. It is hypothesized that an adequate lymphadenectomy misses nodal disease leading to risk of understaging [18]. Thus, patients with inadequate lymphadenectomy who forego adjuvant chemotherapy are at risk for undertreatment of occult nodal disease.
Previous studies have examined the optimal number of lymph nodes to adequately stage patients with small bowel adenocarcinoma; however, whether an inadequate lymphadenectomy necessitates adjuvant chemotherapy in the presence or absence of additional high‐risk features has not been well described. The objectives of this study are to (1) describe the rate of adjuvant chemotherapy use among patients with stage II small bowel adenocarcinoma, (2) identify factors associated with receipt of adjuvant chemotherapy and (3) examine the association between chemotherapy and overall survival among patients with inadequate lymphadenectomy stratified by the presence or absence of additional high‐risk features.
Materials and Methods
2
Data Source
2.1
This retrospective cohort study of the National Cancer Database (NCDB) 2021 participant user file (PUF) examined patients diagnosed with small bowel adenocarcinoma from January 1st, 2004, to December 31st, 2021. The NCDB is a registry of patients treated at Commission on Cancer (CoC) affiliated sites across the United States and includes data from over 70% of invasive cancer diagnoses nationwide [21]. The project is not human subjects research and thus exempt from institutional review board (IRB) review.
Study Population
2.2
Patients aged 18 and older with confirmed pathologic diagnosis of stage II small bowel adenocarcinoma disease who underwent upfront, curative‐intent surgery and were found to have an inadequate lymphadenectomy were included. An inadequate lymphadenectomy was defined as fewer than 5 lymph nodes retrieved for tumors of the duodenum and fewer than 8 lymph nodes for tumors of the jejunum or ileum. Small bowel adenocarcinomas were identified using International Classification of Diseases for Oncology (ICD‐O‐3) histology codes for non‐mucinous adenocarcinomas 8140, 8143–8145, 8210, 8211, 8255, 8261–8263, and 8490 in locations C17.0, 17.1, 17.2, and 17.9. Patients with missing pathologic staging data, pathologic stage other than stage II, neoadjuvant therapy, missing number of nodes examined, or missing post‐operative treatment data were excluded. In assessing factors associated with receipt of chemotherapy, patients with documented refusal of chemotherapy were excluded. In assessing survival, patients diagnosed in year 2021 and patients who died or were censored within 30 days of surgery were excluded.
Outcomes and Covariates
2.3
Outcomes of interest were receipt of adjuvant chemotherapy within 180 days after surgery and overall survival among patients undergoing surgery for stage II small bowel adenocarcinoma. Overall survival was defined as time from diagnosis to last follow up or death. High‐risk features were defined as T4 primary tumor, positive resection margin, poor differentiation and lymphovascular invasion. Other key covariates contained within the NCDB included basic social and demographic variables, Charlson‐Deyo Comorbidity Index, and hospital characteristics. Average annual hospital volume was defined as the number of patients treated for SBA divided by the number of years the hospital participated in the NCDB. Staging was defined using the American Joint Committee on Cancer (AJCC) 8th edition TNM staging.
Statistical Analysis
2.4
Factors associated with receipt of chemotherapy after upfront resection were assessed using multivariable logistic regression. Models were constructed with all sociodemographic variables and clinically relevant variables included. Missing data were classified as a separate category for multivariable logistic regression analysis. Postoperative survival was assessed using log‐rank testing. Multivariable Cox proportional hazard models were used to assess receipt of adjuvant chemotherapy and postoperative survival in patients with inadequate lymphadenectomy, stratified by the presence or absence of additional high‐risk features. To adjust for immortal time bias, a Cox proportional hazard model with landmark analysis was employed, excluding patients who died or were censored within 180 days. A significance level of α < 0.05 was used for statistical tests. Analyses were completed using Stata® Standard Edition version 18.5 (StataCorp, College Station, TX).
Results
3
Study Cohort
3.1
Of 5051 patients who underwent resection for stage II SBA, 1765 (34.9%) patients had an inadequate lymphadenectomy (Figure 1). An inadequate lymphadenectomy occurred in 350 (20.9%) of duodenal tumors, 569 (49.1%) of jejunal tumors, 274 (32.7%) of ileal tumors, and 572 (61.1%) of other or non‐specified sites in the small intestine. Among all patients with stage II SBA and an inadequate lymphadenectomy, the median age was 68 years, 815 (46.2%) were female, and 1013 (57.4%) had at least one additional high‐risk feature. Most of the cohort was non‐Hispanic white (n = 1224, 69.4%), had a Charlson‐Deyo Score of 0 (n = 1218, 69.0%), and had Medicare insurance (n = 994, 56.3%). Most tumors were T3 (n = 1057, 59.9%) and moderate grade (n = 1106, 62.7%). Additional cohort characteristics are described in Table 1.
Patient cohort flow diagram. NCDB = National Cancer Database.
Factors Associated With Receipt of AC
3.2
Of patients with an inadequate lymphadenectomy, 525 (29.8%) received AC overall including 364 (35.9%) with any high‐risk feature and 161 (21.4%) with no high‐risk features. Most patients, 351 (66.9%), received multiagent AC, while 145 (27.6%) received single agent AC and 29 (5.5%) had unknown regimens. Several clinicopathologic features were associated with receipt of AC including T4 primary tumor (vs. T3 primary tumor, aOR 1.97; 95%CI 1.50–2.57; p < 0.001), poor grade tumor (vs. moderate, aOR 1.42, 95%CI 1.07–1.89; p = 0.015), and positive resection margin (vs. negative margin, aOR 1.62, 95%CI 1.12–2.35; p = 0.011). Older patients were less likely to receive chemotherapy including those aged 70–79 (vs. age 50–59, aOR 0.32, 95%CI 0.20–0.50; p < 0.001) and 80+ (vs. age 50–59, aOR 0.07, 95%CI 0.04–0.14, p < 0.001). Patients living in areas where a higher percentage (≥ 15.3%) of adults with no high‐school diploma were less likely to receive chemotherapy (vs. < 5%, aOR 0.50, 95%CI 0.30–0.83; p = 0.007). A numerically higher rate of AC use was found in later years of diagnosis and for jejunal tumors (vs. duodenal), but did not reach statistical significance. Hospital type (academic or non‐academic) and average annual volume of small bowel adenocarcinomas were not associated with receipt of AC (Table 2).
Adjuvant Chemotherapy and Postoperative Survival
3.3
Receipt of AC, compared with no receipt of AC, was associated with improved 5‐year postoperative survival on unadjusted log‐rank test (p < 0.001) and adjusted Cox model (55.3% vs. 42.3%; Hazard Ratio for mortality (HR) 0.67, 95%CI 0.55–0.83; p < 0.001). When stratified by the presence of additional high‐risk features, receipt of AC, compared with no receipt of AC, was associated with improved 5‐year survival for patients with any additional high‐risk feature on adjusted Cox model (49.9% vs. 31.4%; HR 0.62, 95%CI 0.48–0.79; p < 0.001 Figure 2a). Among patients without additional high‐risk features, AC was associated with improved 5‐year survival on unadjusted log‐rank (p = 0.006) but not on adjusted Cox model (67.1% vs. 53.2%; HR 0.83, 95%CI 0.55–1.24; p = 0.363 Figure 2b, Table 3). Two sensitivity analyses (1) excluding patients 80 years and older and (2) excluding patients diagnosed before 2011 were performed with similar results on the association of adjuvant chemotherapy with survival. A separate landmark analysis excluding patients who died or were censored within 180 days of surgery was performed to adjust for immortal time bias and the Cox model had similar results (Supplemental Table 1).
Kaplan‐Meier survival curves for patients with stage II small bowel adenocarcinoma and inadequate lymphadenectomy (a) with at least one additional high‐risk feature and (b) with no additional high‐risk feature. High‐risk features include T4 primary tumor, positive resection margin, poor differentiation, and lymphovascular invasion.
Discussion
4
Adjuvant chemotherapy is considered for patients with stage II SBA with any high‐risk tumor feature or inadequate lymphadenectomy. It is not well understood if an inadequate lymphadenectomy holds prognostic value in the presence or absence of additional high‐risk factors. This study found that among patients with an inadequate lymphadenectomy, those with T4 tumors, poor grade tumor, or positive resection margins were more likely to receive AC. When examining 5‐year overall survival, adjuvant chemotherapy was associated with improved survival among patients with an inadequate lymphadenectomy and any additional high‐risk feature, but not in those without any additional high‐risk features.
Patients with high‐risk features were more likely to receive AC for stage II SBA with inadequate lymphadenectomy, whereas older patients were less likely to receive AC. These high‐risk features included positive resection margin, T4, and poorly differentiated tumors. These results are concordant with retrospective analyses indicating that patients who received chemotherapy for stage II disease were younger and had T4 tumors or inadequate lymphadenectomy [22]. However, AC was administered to just 35.9% of patients with stage II SBA and inadequate lymphadenectomy with at least one additional high‐risk feature, which shows significant treatment heterogeneity. Some patients may have refused chemotherapy, have access or affordability barriers, or been too ill to undergo adjuvant treatment. NCCN guidelines list both observation and adjuvant chemotherapy as management options for patients with stage II SBA with inadequate lymphadenectomy, and thus patients who underwent observation only received guideline‐concordant treatment [14].
Among patients with stage II SBA with a high‐risk feature in addition to inadequate lymphadenectomy, this study found improved survival after receipt of AC in adjusted modeling. The high‐risk features of T4 tumor, lymphovascular invasion, positive margin or poor differentiation suggest more aggressive tumor biology and elevated risk of missed nodal disease. These results are concordant with a previous propensity‐matched analysis of the NCDB found data which supported use of AC in patients with SBA and nodal disease and a potential benefit for those with T4 tumors or positive margins [13]. Likewise, a multicenter retrospective analysis found a survival benefit for AC in patients with stage III disease and for those with high‐risk stage II disease (defined as T4 and/or fewer than 8 lymph nodes examined), suggesting inadequate lymphadenectomy may corelate with disease that would benefit from AC. The present study uses current guideline definitions of inadequate lymphadenectomy and criteria of high‐risk tumor characteristics. The high‐risk SBA tumor characteristics of perineural and lymphovascular invasion or poorly differentiated tumors are based on extrapolation from colorectal studies. When considering the high‐risk features in aggregate, these results suggest that patients with an inadequate lymphadenectomy and any high‐risk feature may have improved outcomes with AC. Notably, fewer than half of such patients received AC in this study's retrospective cohort. For patients with inadequate lymphadenectomy and no additional high‐risk feature, the data indicate numerically higher survival with adjuvant chemotherapy, but this outcome did not reach statistical significance in adjusted modeling. Clinicians may consider individual patient clinical and pathologic factors when recommending adjuvant treatment for a patient with stage II SBA and inadequate lymphadenectomy.
This study has several limitations which affect the ability to address the aims of this study. First, there are limitations associated with utilizing a retrospective database. The NCDB has known selection bias of Commission on Cancer‐associated facilities and underrepresents certain racial and ethnic groups [23]. Second, certain treatment details are not present in the NCDB such as specific regimen and duration of systemic chemotherapy, which may underestimate the effect of adjuvant therapy as patients who complete all cycles of chemotherapy are grouped with those who do not. Third, retrospective studies of postoperative survival are prone to immortal time bias when stratified by an adjuvant treatment, as those who receive the adjuvant treatment must survive to that point to receive it. To adjust for immortal time bias, a landmark analysis was conducted with time zero being 180 days after surgery which showed similar results and association between AC and survival. However, there is likely selection bias in which patients receive adjuvant chemotherapy, such as those who are healthier, which is not fully captured by variables available in the NCDB and may overestimate the beneficial effects of chemotherapy in this retrospective analysis. Fourth, data on disease‐specific recurrence is not available, and limits the ability to assess recurrence‐free survival after curative‐intent surgery for stage II SBA.
Conclusion
5
Among patients with upfront resection for stage II small bowel adenocarcinoma and an inadequate lymphadenectomy, 29.8% received adjuvant chemotherapy and 57.4% had an additional high‐risk feature such as T4 tumor, poorly differentiated tumor, lymphovascular invasion, or positive resection margin. Patients were more likely to receive adjuvant chemotherapy if they had a T4 tumor, poor grade tumor, or positive resection margins. Receipt of AC was associated with improved 5‐year postoperative survival in patients with inadequate lymphadenectomy and any additional high‐risk feature but not in patients with no additional high‐risk feature. Multiple patient and pathologic variables should be considered in decisions regarding AC in this patient population.
Conflicts of Interest
The authors declare no conflicts of interest.
Synopsis
Among patients with upfront resection for stage II small bowel adenocarcinoma, 35% had an inadequate lymphadenectomy. Receipt of adjuvant chemotherapy was associated with improved 5‐year postoperative survival in patients with inadequate lymphadenectomy and any additional high‐risk feature (such as T4 tumor, poorly differentiated tumor, lymphovascular invasion, or positive resection margin) but not in patients with no additional high‐risk feature. Decisions regarding chemotherapy should consider multiple patient and pathologic variables.
Supporting information
Supplemental Table 1: Cox proportional hazard ratios for mortality via landmark analysis beginning 180 days after surgery among patients with pathologic stage II small bowel adenocarcinoma and inadequate lymphadenectomy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1K. Y. Bilimoria , D. J. Bentrem , J. D. Wayne , C. Y. Ko , C. L. Bennett , and M. S. Talamonti , “Small Bowel Cancer in the United States: Changes in Epidemiology, Treatment, and Survival Over the Last 20 Years,” Annals of Surgery 249, no. 1 (2009): 63–71.19106677 10.1097/SLA.0b 013e 31818 e 4641 · doi ↗ · pubmed ↗
- 2A. Alfagih , M. Alrehaili , and T. Asmis , “Small Bowel Adenocarcinoma: 10‐Year Experience in a Cancer Center‐The Ottawa Hospital (TOH),” Current Oncology 29, no. 10 (2022): 7439–7449.36290862 10.3390/curroncol 29100585 PMC 9600419 · doi ↗ · pubmed ↗
- 3M. Akce , R. Jiang , K. Zakka , et al., “Clinical Outcomes of Small Bowel Adenocarcinoma,” Clinical Colorectal Cancer 18, no. 4 (2019): 257–268.31606297 10.1016/j.clcc.2019.08.002 · doi ↗ · pubmed ↗
- 4American Cancer Society Key Statistics for Small Intestine Cancer , accessed May 27, 2024, https://www.cancer.org/cancer/types/small-intestine-cancer/about/what-is-key-statistics.html.
- 5R. D. Bojesen , L. B. Riis , E. Høgdall , O. H. Nielsen , and T. Jess , “Inflammatory Bowel Disease and Small Bowel Cancer Risk, Clinical Characteristics, and Histopathology: A Population‐Based Study,” Clinical Gastroenterology and Hepatology 15, no. 12 (2017): 1900–1907.28694132 10.1016/j.cgh.2017.06.051 · doi ↗ · pubmed ↗
- 6J. Torres , S. Mehandru , J. F. Colombel , and L. Peyrin‐Biroulet , “Crohn's Disease,” Lancet 389, no. 10080 (2017): 1741–1755.27914655 10.1016/S 0140-6736(16)31711-1 · doi ↗ · pubmed ↗
- 7L. Emilsson , C. Semrad , B. Lebwohl , P. H. R. Green , and J. F. Ludvigsson , “Risk of Small Bowel Adenocarcinoma, Adenomas, and Carcinoids in a Nationwide Cohort of Individuals With Celiac Disease,” Gastroenterology 159, no. 5 (2020): 1686–1694.e 2.32679218 10.1053/j.gastro.2020.07.007 · doi ↗ · pubmed ↗
- 8H. Bhatt and K. L. Mathis , “Small Bowel Carcinoma in the Setting of Inflammatory Bowel Disease,” Clinics in Colon and Rectal Surgery 37, no. 1 (2024): 046–052.10.1055/s-0043-1762929 PMC 1076958038188070 · doi ↗ · pubmed ↗