Frequency of work-related musculoskeletal disorders among physical therapists: a systematic review
Tahir Mahmood, Waqar Afzal, Wajeeha Mahmood, Umer Maqsood, Alberto Sumiya

TL;DR
Physical therapists often suffer from work-related musculoskeletal disorders, with low back pain being the most common.
Contribution
This systematic review provides updated prevalence data on musculoskeletal disorders among physical therapists from 2015 to 2021.
Findings
75.27% of physical therapists experience work-related musculoskeletal disorders.
Low back pain is the most prevalent disorder, affecting 54.97% of therapists.
Neck, shoulder, and knee pain are also commonly reported among physical therapists.
Abstract
Musculoskeletal disorders are common among physical therapists because of constant physical work and mechanical stress during interventions. The aim is to synthesize the information of work-related musculoskeletal disorders among physical therapists. A systematic review of observational studies was conducted on PubMed and Google Academics, considering for searching the period of 2015 and 2021. The methodological quality of the studies included were appraised using the Critical Appraisal Skills Programme. The average percentages were calculated by adding the percentages of individual studies for each region and divided by the total number of studies. A total of 74 articles was screened, and 20 of which were assessed. In general, the frequency of work-related musculoskeletal disorders was high (75.27%), with low back pain (54.97%) in first, followed by neck pain (36.16%), upper back pain…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
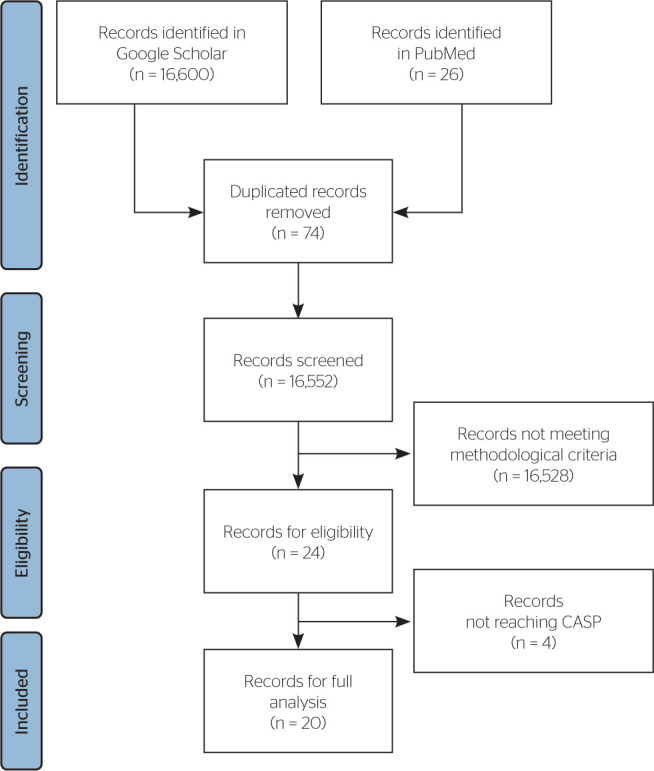 Figure 1
Figure 1| First author | Clear statement of research aim | Appropriate qualitative methodology | Appropriate research design | Appropriate recruitment | Data collected addressing specific issue | Researcher–participant considerations | Ethical considerations | Rigorous data analysis | Clear statement of findings | Valuable Results |
|---|---|---|---|---|---|---|---|---|---|---|
| Narendrasinh JU | Yes | Yes | Yes | None | Yes | None | Yes | Yes | Yes | Yes |
| Sagahutu JB | Yes | Yes | Yes | None | Yes | None | Yes | Yes | Yes | Yes |
| Anyfantis I | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes | Yes | Yes |
| Balakrishnan R | Yes | Yes | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes |
| Kutty RK | Yes | Yes | Yes | None | Yes | None | Yes | Yes | Yes | Yes |
| Prerana S | Yes | Yes | Yes | None | Yes | None | Yes | Yes | Yes | Yes |
| Pfumojena CC | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes | Yes | Yes |
| Mondal A | Yes | Yes | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes |
| Nazari H | Yes | Yes | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes |
| Happy SM | Yes | Yes | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes |
| Iqbal Z | Yes | Yes | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes |
| Vieira ER | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Islam M | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Muaidi QI | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Abaraogu UO | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Alnaser MZ | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Rahimi F | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Ezzatvar Y | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Bae Y-H | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Nasir A | Yes | Yes | Yes | None | Yes | Yes | Yes | Yes | Yes | Yes |
| First author | Country | Size of study sample | Total WMSDs (n [%]) | WMSD by gender | Age (mean ± SD) | |
|---|---|---|---|---|---|---|
| Male (n [%]) | Female (n [%]) | |||||
| Narendrasinh JU | India | 60 | 41 (68.0) | * | * | 30 ± 9 |
| Sagahutu JB | Nigeria (Kigali) | 49 | 38 (77.0) | 65.7 (25.0) | 34.3 (13.0) | 30.89 ± 5.7 |
| Anyfantis I | Greece | 252 | 224 (89.0) | 42.18 ± 9.2 | ||
| Balakrishnan R | Malaysia | 70 | 49 (70.0) | 20 (14.0) | 50 (35.0) | 28.02 ± 5.9 |
| Kutty RK | Kerala (India) | 190 | 119 (67.3) | * | * | * |
| Prerana S | South Gujarat (India) | 271 | 170 (62.73) | 31 (52.0) | 69 (118.0) | 25.38 ± 3.2 |
| Pfumojena CC | Zimbabwe | 261 | 224 (86.1) | * | * | 34.5 ± 9.5 |
| Mondal A | Bangladesh (Dhaka) | 61 | 28 (46.0) | * | * | 34.5 ± 14.5 |
| Nazari H | Hamedan (Iran) | 45 | 30 (65.9) | * | * | 36.49 ± 7.4 |
| Happy SM | Bangladesh | 60 | 57 (95.0) | 36.84 (21.0) | 63.16 (36.0) | 26.91 ± 3.5 |
| Iqbal Z | Delhi (India) | 75 | 67(92.0) | 24 (16.0) | 43 (29.0) | 30.00 ± 10 |
| Vieira ER | USA(Florida) | 121 | 116 (96.0) | * | * | 43 ± 12 |
| Islam MS | Bangladesh (Dhaka) | 101 | 96 (95.0) | * | * | 27.8 ± 4.5 |
| Muaidi QI | KSA (Dammam) | 690 | 329 (47.7) | * | * | * |
| Abaraogu UO | Nigeria | 126 | 100 (80.0) | * | * | 31.98 ± 4.9 |
| Alnaser MZ | Kuwait | 312 | 150 (48.0) | * | * | 34. 25 ± 7.2 |
| Rahimi F | Iran | 319 | 300 (94.0) | Less | More | 47.00 ± 26 |
| Ezzatvar Y | Spain | 981 | 560 (57.0) | * | * | 34.3 ± 8 |
| Bae Y-H | South Korea | 788 | 745 (94.5) | Less | More | 35.0 ± 15 |
| Nasir A | Pakistan | 56 | 52 (93.02) | 27.30 ± 5.3 | ||
| First author | Country | Size of study sample (n) | Low back pain | Upper back pain | Neck pain | Shoulder pain | Hand pain | Wrist pain | Elbow pain | Hip pain | Knee pain | Ankle pain |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Narendrasinh JU | India | 60 | 25 (41.6) | 10 (16.6) | 16 (26.66) | 9 (15.0) | 4 (6.66) | 4 (6.66) | 6 (10.0) | 1 (1.66) | 3 (5.0) | 10 (16.66) |
| Sagahutu JB | Nigeria | 49 | 38 (77.1) | 28 (57.1) | 39 (79.0) | 25 (51.1) | 15 (31.4) | 15 (31.4) | 3 (5.7) | 3 (5.7) | 7 (14.6) | 0 (0.00) |
| Anyfantis I | Greece | 252 | 124 (49.0) | 63 (25) | 48 (19.0) | 76 (30.0) | 60 (24.0) | 60 (24.0) | 35 (14.0) | 48 (19) | 48 (19.0) | — |
| Balakrishnan R | Malaysia | 70 | 31 (44..0) | 10 (14) | 14 (20.0) | 6 (8.0) | 4 (5.0) | 4 (5.0) | 0 | 1 (1.0) | 8 (11.0) | 2 (3.0) |
| Kutty RK | India | 190 | 70 (36.6) | 15 (8) | 27 (14.0) | — | 13 (7.0) | 13 (7.0) | — | 10 (5.0) | — | — |
| Prerana S | India | 271 | 177 (65.3) | 43 (15.9) | 113 (41.8) | 72 (26.5) | 43 (15.9) | 43 (15.9) | 16 (5.9) | 11 (4.1) | 30 (11.2) | 11 (4.1) |
| Pfumojena CC | Zimbabwe | 261 | 207 (79.3) | 135 (51.7) | 97 (37.0) | 141 (54.0) | 109 (41.4) | 109 (41.4) | 27 (10.3) | 15 (5.7) | 42 (16.1) | 33 (12.6) |
| Mondal A | Bangladesh | 61 | 45 (28.0) | — | 18 (30.0) | 8 (12.5) | 2 (2.5) | 2 (2.5) | — | — | 6 (10.0) | — |
| Nazari H | Hamedan | 45 | 13 (31.7) | 7 (17.1) | 11 (26.8) | 8 (19.5) | 14 (34.1) | 15 (34.1) | 5 (12.2) | 3 (7.3) | 12 (29.3) | 3 (7.3) |
| Happy SM | Bangladesh | 60 | 43 (71.7) | 26 (43.3) | 21 (35.0) | 8 (13.3) | 10 (16.7) | 10 (16.7) | 3 (6.7) | 3 (5.0) | 12 (20.0) | 9 (15.0) |
| Iqbal Z | India | 75 | 38 (51.0) | 6 (7) | 13 (17.0) | 9 (12.0) | 5 (7.0) | 5 (7.0) | 11 (15.0) | 11 (15.0) | 11 (15.0) | 11 (15.0) |
| Vieira ER | United States of America | 121 | 80 (66.0) | 43 (35) | 74 (61.0) | 51 (42.0) | 44 (36.0) | 44 (36.0) | 18 (15.0) | 28 (23.0) | 44 (36.0) | 30 (25.0) |
| Islam MS | Bangladesh | 101 | 91 (90.0) | 82 (82) | 73 (72.0) | 56 (55.0) | 25 (24.0) | 25 (24.0) | 23 (23) | 21 (21.0) | 54 (53.0) | 46 (45.0) |
| Muaidi QI | Kingdom of Saudi Arabia | 690 | 321 (46.5) | 20 (2.9) | 18 (26.5) | 84 (12.2) | — | — | 70 (10.2) | 55 (8.0) | 75 (10.9) | 24 (3.5) |
| Abaraogu UO | Nigeria | 126 | 73 (58.0) | 38 (29.8) | 53 (41.9) | 38 (30.1) | 36 (28.3) | 36 (28.3) | 14 (10.8) | 21 (16.1) | 26 (20.7) | 12 (10.0) |
| Alnaser MZ | Kuwait | 312 | 172 (55.0) | — | 34 (11.0) | 22 (7.0) | 62 (20.0) | 62 (20.0) | — | — | — | — |
| Rahimi F | Iran | 319 | 207 (65.0) | 156 (49) | 183 (57.4) | 160 (50.2) | — | — | 69 (21.6) | 39 (12.2) | 145 (45.5) | 63 (19.7) |
| Ezzatvar Y | Spain | 981 | 485 (49.0) | 345 (36.1) | 56 (57.0) | 332 (33.8) | 323 (32.7) | 323 (32.7) | 164(16.7) | — | — | — |
| Bae Y-H | South Korea | 788 | 179 (23.0) | 179 (22.7) | 11 (14.0) | 184 (23.3) | 179 (22.7) | 179 (22.7) | 73 (9.3) | 63 (8.0) | 63 (8.0) | 63 (8.0) |
| Nasir A | Pakistan | 56 | 31 (56.0) | 22 (39.5) | 35 (62.8) | 13 (23.3) | 5 (9.3) | 5 (9.3) | 4 (7.0) | 8 (14.0) | 7 (11.6) | 3 (4.7) |
| Job risk factors | Authors | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Shiba | Sagahutu | Anyfantis | Balakrishnan | Prerana | Pfumojena | Happy | Islam | Alnaser | Aiza Nasir | |
| Repetitive tasks | 26 (43.3) | 5 (11.0) | 226 (90.0) | 38 (54.3) | 132 (48.8) | 144 (55.2) | 25 (41.7) | 277 (40.1) | 2 (5.0) | 22 (37.2) |
| Number of patients treated per day | 33 (55.0) | 15 (31.1) | — | 52 (74.3) | 185 (68.2) | 162 (62.1) | — | 209 (30.3) | — | 21 (34.9) |
| Limited breaks during work | 33 (55.16) | 10 (20.0) | — | - | 148 (54.7) | 63 (24.1) | 42 (70.0) | 129 (18.7) | — | 27 (44.2) |
| Manual therapies | 32 (53.33) | 9 (17.8) | — | 48 (68.6) | 110 (40.6) | 136 (52.2) | 204 (29.6) | 81 (26.0) | 20 (32.6) | |
| Awkward/cramped working posture | 24 (40.0) | 14 (28.9) | 175 (70.0) | 43 (61.4) | 172 (63.6) | 87 (33.3) | 14 (23.3) | 316 (45.9) | — | 20 (39.5) |
| Reaching/working away from body | 29 (48.33) | 4 (8.9) | — | 39 (55.7) | 144 (53.0) | 66 (25.3) | — | 166 (24.1) | — | 8 (14.0) |
| Back twisting/bending awkwardly | 25 (41.66) | 14 (28.9) | — | 54 (77.1) | 178 (65.8) | 102 (39.1) | 18 (30.0) | 129 (18.7) | — | 23 (37.2) |
| Unanticipated/sudden movements | 27 (45.0) | 3 (6.7) | 88 (35.0) | 17 (24.3) | 128 (47.1) | 51 (19.5) | — | 171 (24.8) | — | 4 (7.0) |
| Assisting in gait training/activities | 28 (46.66) | 5 (11.0) | — | 33 (47.1) | 110 (40.6) | 54 (20.7) | — | 289 (41.9) | — | 12 (18.61) |
| Lifting/transferring patients | 27 (45.0) | 15 (31.1) | — | 57 (81.4) | 155 (57.0) | 129 (49.4) | — | 0 (0.00) | 137 (44.0) | 10 (16.3) |
| Managing agitated/confused patients | 25 (41.66) | 8 (15.6) | — | 28 (40.0) | 100 (37.0) | 42 (16.1) | — | 103 (14.9) | — | 4 (7.0) |
| Carrying/lifting heavy equipment | 26 (43.33) | 7 (13.3) | — | 43 (61.4) | 128 (47.1) | 45 (17.2) | — | 119 (17.2) | — | 6 (9.4) |
| Working at physical limit | 23 (38.33) | 10 (20.0) | — | 42 (60.0) | 136 (50.0) | 51 (19.5) | 235 (34.1) | — | 10 (16.3) | |
| Working despite pain/injury | 21 (35.0) | 13 (26.7) | — | 43 (61.4) | 173 (63.6) | 114 (43.7) | 16 (26.7) | 143 (20.7) | — | 18 (30.2) |
| Long shifts or overwork | 23 (38.33) | 4 (8.9) | — | 41 (58.6) | 150 (55.3) | 63 (24.1) | 33 (55.0) | 216 (31.3) | — | 18 (32.6) |
| Inadequate training for injury prevention | 19 (31.66) | 8 (15.6) | — | 37 (52.9) | 134 (49.4) | 24 (9.2) | — | 136 (19.7) | — | 7 (11.6) |
| Prolonged static posture | — | 20 (40.0) | — | 58 (82.9) | 209 (77.0) | 117 (44.8) | 36 (60.0) | 300 (43.5) | 31 (10.0) | — |
| Significant forces | — | — | 76 (30.0) | — | — | — | — | — | — | — |
| Workplace environmental conditions | — | — | 38 (15.0) | — | — | — | — | — | — | — |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleistocene-Era Hominins and Archaeology · Archaeology and ancient environmental studies · Pacific and Southeast Asian Studies
INTRODUCTION
Work-related musculoskeletal disorders (WMSDs) are common among health care professionals, who are frequently exposed to physically demanding environments and excessive biomechanical stress. These conditions can lead to poor physical functioning and the development of inflammatory disorders affecting tendons, ligaments, nerves, soft tissues, and joints as well as degenerative diseases.^1^
Among health professionals, physical therapists are particularly vulnerable due to the physical demands of their practice, which often exceed those of other health-related occupations. This increased physical burden has been associated with absenteeism, reduced quality of life, and potentially slower patient recovery.^2,3^ The Global Burden of Disease study showed a prevalence of 1.71 billion for musculoskeletal disorders, with low back pain among the most prevalent.^4^ A number of studies have examined the risks, causes, prevalence, and ergonomic factors associated with such conditions.^2-11^
For physical therapists, WMSDs tend to be more prevalent during the early stages of their careers and may decrease over time as professionals adopt improved posture and ergonomic techniques.^5,6^ Understanding these trends can inform future discussions on prevention strategies and workload management. Therefore, the aim of this systematic review was to synthesize the current evidence on the prevalence and characteristics of WMSDs among physical therapists.
METHODS
This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) under protocol code CRD42021243974. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Cochrane Handbook for Systematic Reviews to ensure methodological rigor and transparency.
STUDY DESIGN AND PARTICIPANTS
This systematic review included observational studies investigating WMSDs among physical therapists.
INCLUSION CRITERIA
Studies were included if they were available in full text, written in English, and published between 2015 and May 30, 2021.
EXCLUSION CRITERIA
Studies were excluded if they were review articles, case reports, focused on other health professionals, or addressed variables not related to the frequency, risk factors, or prevention of WMSDs.
SEARCH STRATEGY
A total of two databases — Google Scholar and PubMed — were searched for relevant articles. Boolean operators “AND” and “OR” were applied to combine the following search terms: “risks,” “work-related musculoskeletal disorders,” “musculoskeletal disorders,” and “physical therapist.”
SELECTION OF STUDIES
After an initial screening of titles, two independent authors applied the inclusion and exclusion criteria to the selected studies. Disagreements between the authors were resolved by a third author.
DATA EXTRACTION
The following data were extracted from the included studies: country of study, participants’ age, year of publication, type of WMSD or discomfort, affected body region, and prevalence rate.
ASSESSMENT OF QUALITY
Assessment of quality of included studies was performed using the Critical Appraisal Skills Programme, which consists of 10 general questions. Each question could be answered as “yes,” “cannot tell,” or “no.” A total score of up to 10 points was assigned to each study based on how many criteria were fully met.^12^ No classification system was applied based on the total score.
QUANTITATIVE ANALYSIS
A descriptive analysis was conducted. Average prevalence rates were calculated by summing the percentages reported in individual studies for each body region and dividing by the total number of studies included in the final analysis.
RESULTS
A total of 16,626 studies were identified, of which 20 were included for full analysis after applying the inclusion and exclusion criteria (Figure 1). Data were organized into four four tables covering quality assessment, demographic characteristics, WMSDs by body region, and job-related risk factors.
Flowchart of the study. CASP: Critical Appraisal Skills Programme.
ASSESSMENT OF QUALITY
Among the 20 studies analyzed, 8 received a total score of 10 points, 7 studies scored 9 points, and 5 studies scored 8 points. The most common methodological issues were related to recruitment procedures and lack of consideration for researcher-participant dynamics. Overall, studies demonstrated good methodological quality (Table 1).
WMSDs BY GENDER
A study from Nigeria reported a WMSD prevalence of 77.8% (38 individuals) among physical therapists, with higher prevalence in men (25 [65.7%]) compared to women (13 [24.3%]).^13^ In contrast, data from Bangladesh showed women were more affected (64.4%) than men (58.8%).^28^ Another Bangladeshi study found a higher proportion of WMSDs among women (63.16%) than men (36.84%).^18^
In India, women were generally more prone to WMSDs.^2^ A study reported that even a 1 kg increase in body weight was associated with a 29% higher risk of developing musculoskeletal pain, with women being more vulnerable to spine-related issues.^11^ Low back pain (LBP) was the most prevalent WMSD among women (64.1%) compared to men (67.9%) in a sample of 160 physical therapists^14^ (Table 2).
Table 2: Year-wise demographic distribution of work-related musculoskeletal disorders (WMSDs)
WMSDs BY COUNTRY
High WMSD prevalence was reported in countries such as Egypt (815, 97.6%),^7^ Greece (224, 89%), and India (41, 68%).^2^ In Canada, pediatric and neurological physical therapists also showed high rates of WMSDs.^2^ In Bangladesh, intensive care unit was associated with higher WMSD prevalence than general wards.^29^ These disorders were present in both developed and underdeveloped regions, such as Kuwait (150, 48%).^3^ In Iran, physical therapists had a lower WMSD prevalence (58.3%) compared to occupational therapists (76.4%).^8,9^
WMSDs BY YEARS OF EXPERIENCE
WMSDs were more prevalent among health professionals with fewer years of experience. The highest prevalence was found in those with 1-5 years of experience (52%), with a notable decrease among those with 6-15 years (13%). In Greece, 32.2% of physical therapists developed injuries within their first 5 years of practice.^8,10^
A 2015 study also observed that longer working hours increased the risk of WMSDs.^11^ Similarly, a study from Bangladesh^18^ found that 82.5% of cases occurred within the first 5 years, with a decrease to 14% in those with up to 10 years of experience and only 3.5% after 10 years. Another study reported that musculoskeletal symptoms often began within the first year of practice (65%).^9^
WMSDs BY BODY REGION
In Pernambuco, Brazil, manual therapists most frequently reported cervical and lumbar spine disorders (60%), followed by wrist/hand (56%) and shoulder (50%) complaints.^30^ A study found LBP in 44% of physical therapists who did not use armrests, followed by neck and shoulder pain (27% each).^10^ In Kigali, India, the low back was the most affected region (71.1%).^13^
In Malaysia, 70% of participants reported WMSDs, with the low back being the most affected region, followed by the neck.^10^ However, a study found that while LBP was the most prevalent issue, wrist pain also showed notable prevalence (15.5%).^11^ Similar patterns were observed in Ireland, where 49% of therapists reported LBP,^31^ with higher prevalence in women (52%) compared to men (42%)^11^ (Table 3).
Table 3: Description of work-related musculoskeletal disorders (WMSDs) by body region and pain†, n (ages in %)
JOB-RELATED RISK FACTORS
A total of 19 job-related risk factors were identified across 10 studies (Table 4). Balakrishnan et al.^10^ reported the highest number of contributing factors, while the study by Anyfantis & Biska^8^ found task repetition to be the most frequent factor (90%), followed by working in static postures (82.9%).^9^
Table 4: Job-related risk factors contributing to the development of work-related musculoskeletal disorders (WMSDs)
DISCUSSION
The aim of this systematic review was to synthesize the current evidence on the prevalence and characteristics of WMSDs among physical therapists WMSDs among physical therapists. According to the World Health Organization, WMSDs encompass a broad range of inflammatory and degenerative conditions that result in pain and functional impairment. Health professionals, particularly those in direct contact with patients, are among the professional groups with the highest rates of WMSDs due to the physical demands of their work and prolonged static or awkward postures throughout the day.^32^
WMSDs are common among health professionals, especially those involved in direct patient care.^33^ Physical therapists perform numerous physically demanding tasks, such as transferring and repositioning patients, frequent trunk flexion and rotation, and maintaining awkward postures. In addition, psychosocial factors have also been linked to the development of WMSDs. Physical therapy involves repetitive tasks, and most physical therapists report symptoms of WMSDs within the first 5 years of practice.^9^
In the current review, the overall prevalence of WMSDs among physical therapists was 75.27%, which is considered high. LBP was the most frequently reported condition (54.97%), followed by neck and upper back pain.^34^ Regarding the upper extremities, the most commonly affected regions were the shoulders and hands/wrists, while the knees were most frequently reported among lower extremity complaints.^11^ However, the prevalence may vary across different specialties.^20^
Although physical therapists are trained in ergonomics and injury prevention, their risk of developing WMSDs remains high. This can result in increased health care costs and reduced productivity. It also may also lead to career changes, decreased clinical longevity, or even premature departure from the profession. Contributing factors to WMSDs include improper biomechanics, repetitive strain, poor flexibility, and muscle overuse. Common outcomes include soft tissue injuries, sprains, strains, spondylosis, herniated discs, osteoarthritis, and neuropathies.^35^
Although LBP is the most prevalent WMSD, it does not necessarily result in absenteeism. Instead, many physical therapists continue working despite symptoms, a phenomenon known as presenteeism. This behavior may reduce work efficiency and increase the likelihood of clinical errors as well as contribute to secondary health issues such as hypertension, arthritis, migraines, insomnia, and mental health disorders. Feelings of fatigue and overload are also associated with job dissatisfaction.^36^
A study reported that 3.1% of physical therapists discontinued work due to aggravated symptoms during patient care.^19^ Pfumojena^15^ observed that approximately 66.7% of WMSDs developed within the first 5-6 years of professional practice,^20,26,37^ although this percentage may vary.^25^ The physical demands placed on the spine — particularly the lumbar region — are especially significant for physical therapists. Consequently, LBP and related symptoms are most prevalent during the early years of professional activity.^13^ However, the frequency tends to decrease after 15 years of experience.^10^ In terms of work experience, Prerana et al.^14^ also found a gradual decline in WMSD prevalence over time.^15^ This trend may be explained by the fact that professional experience enhances ergonomic awareness and the use of self-protection strategies.
Regarding gender, female physical therapists were initially more prone to WMSDs than males, possibly due to lower body mass index (BMI) and physical demands of patient handling.^16,17^ However, with increasing years of experience, the prevalence among male professionals tends to rise, and after 15 years, the gender difference becomes negligible.^14^ Other studies suggest males are ultimately more affected by WMSDs compared to females.^21^
In relation to manual therapy, a study involving 361 physical therapists reported that the most affected regions were the wrists and hands (80.6%), followed by the back (28%).^38^ Concerning BMI, 64% of females were in the normal weight range, while 53.8% of males and 23.2% of females were overweight, and 15.2% of males and 11.6% of females were obese. These factors may negatively impact personal and family life, including physical fitness, leisure activities, and daily functioning.
Another study involving 1,232 health professionals indicated that WMSDs may be associated with moderate to high levels of occupational stress, which could contribute to sleep disturbances. However, the association between WMSDs and sleep disorders was found to be weak.^39^
Regarding ergonomic risks, 224 clinical physical therapy sessions performed by 29 physical therapists were analyzed. Among the 224 observations (132 adult and 92 pediatric sessions), physical therapists were frequently found working in sitting, standing, or kneeling postures, with 82.59% of tasks classified as presenting high or very high ergonomic risk. Pediatric sessions were associated with higher ergonomic risk than adult sessions.^40^
With regard to WMSD management strategies, physical therapists typically seek medication, consult physicians, and modify patient-handling techniques or body positioning. Preventive strategies to reduce the incidence of WMSDs among physical therapists include limiting the number of patients seen per day in clinical settings; incorporating scheduled breaks during work shifts; reinforcing proper ergonomics through ongoing training, especially in manual therapy settings; implementing assistive devices to standardize therapist posture; conducting annual health screenings in rehabilitation centers and physical therapy departments; and encouraging daily physical activity to maintain general fitness. Finally, the limitations of this study were the use of only two search engines and the time frame from 2015 to May 30, 2021. Nevertheless, we believe this review offers valuable insights for the development of future protocols aimed at preventing the occurrence of WMSDs among physical therapists.
CONCLUSIONS
Physical therapists had a high prevalence of WMSDs. The most commonly affected body region was the lower back, followed by the neck and wrist. Male professionals were more frequently affected, and the injuries were primarily associated with ergonomic risk factors and individual physical conditions — especially among those with 1-5 years of professional experience. Most of the included studies were cross-sectional, which highlights the need for longitudinal research to better understand how the prevalence of WMSDs evolves over time.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Plange EB Work-related musculoskeletal disorders among physiotherapists in Ghana: prevalence, perceived causes and coping strategiesthesis Ghana University of Ghana 2019
- 2Narendrasinh JU Mulla A Prevalence and risk factors of work-related injuries among physical therapists in Indian population Int J Sci Res.2015425758
- 3Alnaser MZ Aljadi SH Physical therapists with work-related musculoskeletal disorders in the State of Kuwait: a comparison across countries and health care professions Work 201963226183115620710.3233/WOR-192927 · doi ↗ · pubmed ↗
- 4Cieza A Causey K Kamenov K Hanson SW Chatterji S Vos T Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019 Lancet 2021396102672006173327590810.1016/S 0140-6736(20)32340-0PMC 7811204 · doi ↗ · pubmed ↗
- 5Bork BE Cook TM Rosecrance JC Engelhardt KA Thomason M-EJ Wauford IJ Work-related musculoskeletal disorders among physical therapists Phys Ther.199676882735871096210.1093/ptj/76.8.827 · doi ↗ · pubmed ↗
- 6Anghel M Argeanu V Talpo C Lungeanu D Musculoskeletal disorders (MSDS) consequences of prolonged static postures J Exper Med Surg Res.2007416772
- 7Rasha AE Amir M Elsayed SE Dawood RS Work related musculoskeletal disorders among egyptain physical therapists and years of experience South Valley Univ Int J Phys Ther Sci.20191117
- 8Anyfantis I Biska A Musculoskeletal disorders among Greek physiotherapists: Traditional and emerging risk factors Saf Health Work 20189331483037016310.1016/j.shaw.2017.09.003PMC 6130005 · doi ↗ · pubmed ↗