Factors contributing to medication non-adherence in a hypertensive Saudi population: a literature review
Ahmed Alenazi, Wejdan Alhajri, Waroud Alruwili, Sokaina Alnowiser, Ohud Alsudyyes, Sara Hijazi, Ibtisam Alotaibi, Manal Albukami, Madhwi Aldhfere, Shima Daak, Lujain Alhomaid, Mona Alshamery

TL;DR
This paper reviews factors affecting medication adherence in Saudi patients with hypertension, highlighting demographic, psychosocial, and healthcare-related influences.
Contribution
The study synthesizes existing literature to identify key factors influencing medication adherence in Saudi hypertensive patients.
Findings
Adherence rates among Saudi hypertensive patients range from 33% to 86.1%, influenced by measurement tools and regional differences.
Higher adherence is linked to older age, female gender, higher education, marriage, and higher income.
Psychosocial factors like medication beliefs, social support, and physician-patient relationships significantly impact adherence.
Abstract
Hypertension is a leading non-communicable disease both globally and in Saudi Arabia. Poor adherence to antihypertensive medications remains a major challenge in managing this condition, contributing to higher morbidity, mortality, and healthcare costs. This study aimed to review and synthesize the literature on factors contributing to medication nonadherence among hypertensive patients in Saudi Arabia. A structured literature review was conducted using the PubMed and Scopus databases. Inclusion criteria include English-language studies conducted in Saudi Arabia from 2010 to 2024 involving hypertensive adult Saudi patients. A total of 84 studies were identified. Eleven studies met the final inclusion criteria. All were cross-sectional studies using different validated adherence assessment tools. Adherence rates varied widely, from 33% to 86.1%, influenced by the choice of measurement…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
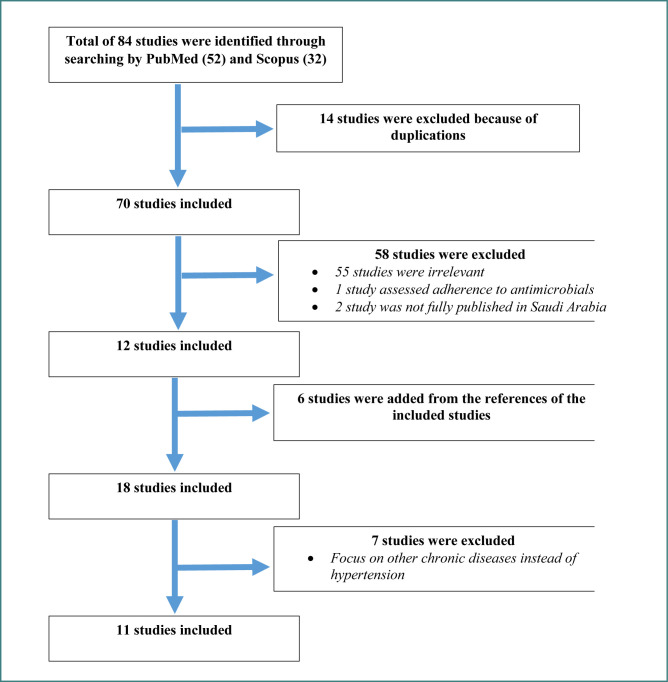 Figure 1
Figure 1| Categories | Factors |
|---|---|
| Patient-related factors [ | Demographic factors: age, ethnicity, gender, education, marital status |
| Therapy-related factors [ | Route of administration |
| Healthcare system factors [ | Lack of accessibility |
| Social and economic factors [ | Inability to take time off work |
| Disease factors [ | Disease symptoms |
| Scale | Items | Domains | Focus | Scoring | Strengths | Limitations |
|---|---|---|---|---|---|---|
| Hill-Bone Medication Adherence Scale (HBMAS) | 9 | Medication-taking behavior | Hypertension medication adherence | Likert (1–4) | Simple; validated in HTN settings | Limited to HTN; cultural adaptation needed |
| Malaysian Medication Adherence Score (MALMAS) | 8 | Intentional and unintentional non-adherence | Chronic diseases (Malaysia) | Mixed (Yes/No + Likert) | Culturally tailored; validated | Country-specific; limited generalizability |
| Morisky Green and Levine adherence scale (MGL) | 4 | Forgetfulness, stopping when better/worse, carelessness | General adherence | Yes/No (0–4) | Very quick; widely used | Oversimplified answers |
| Morisky Medication Adherence Scale-4 (MMAS-4) | 4 | Unintentional & intentional non-adherence | General medication adherence | Yes/No | Easy to administer | Less detailed than MMAS-8 |
| Morisky Medication Adherence Scale-8 (MMAS-8) | 8 | Unintentional & intentional non-adherence | General medication adherence | Mixed (7 Yes/No + 1 Likert) | Comprehensive; distinguishes behavior types; validated across diseases | Requires permission/licensing; longer to administer |
| Author(s) (Year) | Region of KSA | Study design | Number of participants | Adherence measurement tool | Key non-adherence factors identified (summarized) |
|---|---|---|---|---|---|
| Alsolami | Not Specified | Cross-sectional | 200 | MMAS-8 | Low belief in necessity, high concern about side effects, weak physician-patient relationship |
| Elbur (2015) [ | Taif | Cross-sectional | 200 | MGL | Younger age, lower education level, absence of comorbidities |
| Abdelhalim | Dammam | Cross-sectional | 303 | HBMAS | Younger age, male gender, lack of reminders/cues to action |
| Algabbani | Riyadh | Cross-sectional | 340 | MMAS-8 | Polypharmacy, frequent clinic visits |
| Alsofyan | Taif | Cross-sectional | 231 | MMAS-4 | Female gender, older age, being married, higher education |
| Thirunavukkarasu | Abha | Cross-sectional | 400 | MMAS-8 | Being unmarried, low monthly income |
| Innab | Multiple | Cross-sectional | 549 | MMAS-8 | Younger age, lower patient activation |
| Fallatah | Jeddah | Cross-sectional | 384 | MMAS-8 | Younger age, lower education |
| Alfhaid | Majmaah | Cross-sectional | 144 | MMAS-8 | Male gender, low adherence overall |
| ALruwaili (2024) [ | Aljouf | Cross-sectional | 303 | HBMAS | Employment status (private sector linked to higher adherence) |
| Almaghamsi | Jeddah | Cross-sectional | 500 | MALMAS-8 | Lower education, lack of social support, being a government employee |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMedication Adherence and Compliance · Blood Pressure and Hypertension Studies · Pharmaceutical Practices and Patient Outcomes
INTRODUCTION
Hypertension is one of the most prevalent non-communicable diseases, currently affecting nearly 1.3 billion people worldwide. It is a major risk factor for cardiovascular diseases, stroke, and kidney failure. The number is expected to rise to 1.5 billion by 2025 [1-3]. In Saudi Arabia, the prevalence of hypertension varies according to several factors, including age, gender, education level, region, occupation, and access to healthcare services. Reported prevalence rates range from 22% to 25.5% [4,5], while the estimated average across Middle Eastern countries is around 29.5% [3].
The growing burden of hypertension in Saudi Arabia is primarily attributed to an aging population and the increasing prevalence of lifestyle-related risk factors, including unhealthy diets and physical inactivity. In response, the Saudi government has prioritized health improvement through its Vision 2030 initiative, particularly the Health Sector Transformation Program, which aims to increase average life expectancy to 80 years by strengthening healthcare quality, promoting preventive care, and encouraging healthier lifestyles. Despite these efforts, poor medication adherence remains a major challenge in the effective management of hypertension, contributing significantly to its role as one of the leading causes of death and disability in the country [6-8].
Non-adherence to medication and other aspects of the treatment plan can adversely affect treatment outcomes, leading to additional and unnecessary tests, dosage adjustments, treatment plan changes, revisits to the emergency department, or hospitalization, which ultimately result in increased health care service costs, morbidity, and mortality [9,10]. Non-adherence to medication can be intentional or unintentional on the part of the patient. Intentional non-adherence refers to a patient’s purposeful decision not to follow the treatment plan, often influenced by their motivations or beliefs. In contrast, unintentional non-adherence is typically the result of a lack of the capacity, resources, or understanding required to take medications as prescribed [11].
The terms adherence and compliance are globally debated and often used interchangeably in the healthcare field [12]. At the World Health Organization (WHO) Adherence meeting in June 2001, adherence was defined as “the extent to which the patient follows the medical instructions” [13]. According to the National Health Service (NHS), adherence refers to “the extent to which the patient’s behavior matches agreed recommendations from the prescriber”, whereas compliance is defined as “the extent to which the patient’s behavior matches the prescriber’s recommendations” [12]. In this review, the compliance and adherence terms will be used interchangeably.
Numerous factors associated with non-adherence have been identified in the literature. These factors may be grouped into categories including patient-related factors, therapy-related factors, healthcare system factors, social and economic factors, and disease factors (Table 1) [14]. The impact of these factors on medication adherence is variable and controversial, with some studies identifying clear factors that enhance medication adherence, while others fail to replicate these findings.
In connection with this, numerous validated instruments have been created to assess medication adherence from various clinical viewpoints, including the Hill-Bone Medication Adherence Scale (HBMAS) [15], the Malaysian Medication Adherence Score (MALMAS) [16], the Morisky Green and Levine scale (MGL), the Morisky Medication Adherence Scale-4 (MMAS-4), and the Morisky Medication Adherence Scale-8 (MMAS-8) (Table 2) [17,18]. The selection of an appropriate scale should be influenced by the intended population, the clinical setting, and the level of behavioral insight required.
MATERIAL AND METHODS
Study design and search
The review was conducted using PubMed and Scopus to identify studies published between 2010 and 2024. The search strategy combined relevant keywords and MeSH terms to collect research on medication adherence among hypertensive patients in Saudi Arabia. The main search structure utilized was: (hypertension OR high blood pressure) AND (adherence OR compliance) AND (Saudi Arabia OR KSA). In the PubMed search, this was refined using MeSH terms: ("Hypertension"[MeSH] OR "Antihypertensive Agents"[MeSH]) AND ("Medication Adherence"[MeSH] OR "Patient Compliance"[MeSH]) AND "Saudi Arabia"[MeSH]. The search was confined to the English language and human studies only.
Flow diagram of the study selection process
Eligibility criteria
Inclusion criteria: studies published in the English language between 2010 and 2024, involving adult Saudi patients (aged ≥ 18 years) with hypertension.
Exclusion criteria: studies that included non-Saudi populations and did not focus on factors contributing to antihypertensive medication non-adherence.
Quality assessment
The quality of the included cross-sectional studies was evaluated independently by two reviewers using the Joanna Briggs Institute (JBI) critical appraisal checklist for analytical cross-sectional studies. The checklist covers key domains, including sample representativeness, methods of participant recruitment, adequacy of sample size, objectivity of measurements, and appropriateness of statistical analyses. Any differences in judgment were discussed and resolved by consensus.
Findings
We identified 84 records through PubMed (n = 52) and Scopus (n = 32). After removing 14 duplicates, 70 studies remained for title and abstract screening, of which 58 did not meet the inclusion criteria due to being irrelevant or not fully published in Saudi Arabia. We reviewed the full texts of the remaining 12 studies and, through manual reference checking, identified 6 additional relevant articles, bringing the total to 18 studies for full review. After assessing these in detail, 7 were excluded because they focused on other chronic diseases. In the end, 11 studies met all criteria and were included in this review (Figure 1). All included studies were cross-sectional and involved Saudi adults with hypertension, with sample sizes ranging from 144 to 549 participants.
Study selection
Studies were selected after screening the titles and abstracts to ensure that they met the inclusion criteria. The studies were screened for the definition of adherence, the level and prevalence of adherence, setting, population, sample size, methodology, data collection, and the instruments used to measure adherence.
RESULTS
A review of 11 cross-sectional studies conducted in multiple regions of Saudi Arabia, involving 4,194 participants, was performed to investigate adherence to antihypertensive medications (Table 3). The studies used recognized adherence evaluation tools, such as the Hill-Bone Medication Adherence Scale, the Morisky Medication Adherence Scale (MMAS-4 and MMAS-8), the Morisky-Green and Levine (MGL) scale, and the Malaysian Medication Adherence Score (MALMAS-8) [19-29]. Overall, the studies were of moderate quality. Most of these studies clearly described their study populations and used validated tools to assess adherence, which is a consistent strength across the included literature.
The reported medication adherence levels ranged widely. Overall, high adherence rates ranged from 34.3% to 86.1%, with non-adherence rates up to 67%. Alfhaid et al. in Majmaah reported the lowest adherence at 33% using the MMAS-8 scale [27], while Alsofyan et al. in Taif had the highest adherence rate at 86.1% with the MMAS-4 scale [25]. This inconsistency in reported medication adherence rates is attributed to regional variations and methodological differences, particularly the choice of adherence scale.
Various socio-demographic factors have consistently been correlated with antihypertensive medication adherence. Gender differences were noted, with women generally exhibiting higher adherence rates than men [21,25]. Older individuals, particularly those aged 60 and older, were associated with higher adherence levels [23, 25, 26]. Thirunavukkarasu and Alsofyan’s results showed that marital status appeared to play a meaningful role in adherence, with married patients generally showing better adherence to their antihypertensive medications than non-married patients [22,25]. In addition, Elbur and Almaghamsi showed that patients with higher education qualifications tended to be more adherent to and follow their treatment plans [20,29]. Alsofyan and Almaghamsi found that higher income was connected to better medication adherence [25,29]. Interestingly, Alruwaili’s research showed a significant association between private-sector employment and higher adherence rates [28].
Elbur’s study demonstrated that comorbid conditions had a substantial impact on medication adherence, indicating that patients with these conditions were more likely to adhere to their prescribed treatment regimens [20]. Algabbani et al. observed that patients prescribed fewer medications or who attended fewer clinic visits exhibited higher adherence to antihypertensive medications [24].
Psychosocial and behavioral factors were found to significantly affect medication adherence. A strong belief in the necessity of medications and low concerns about potential side effects were associated with improved medication adherence, as noted in Alsolami’s research [19]. In the same study, Alsolami also highlighted that a strong physician-patient relationship was significantly associated with better medication adherence [19]. Social support was also recognized as a key factor, with individuals who perceive higher levels of support showing improved adherence, as demonstrated in Almaghamsi’s study [29]. Abdelhalim et al. found that reminders and other cues to action were especially helpful for those who perceived more barriers, suggesting that external prompts can make a real difference when internal motivation is challenged [21].
Abdelhalim et al., in a study that implemented the Health Belief Model (HBM), which predicts health/disease risk and preventive behavior [30], identified several psychological constructs as important predictors of medication adherence. Greater perceived severity of hypertension, susceptibility to complications, and perceived advantages of medication were all linked to improved adherence. Notably, a higher perception of treatment barriers was also positively correlated with adherence, suggesting that patients who recognized more challenges might be more driven by external cues such as reminders. This finding emphasizes the role of behavioral signals in navigating perceived obstacles and boosting compliance [19].
DISCUSSION
This literature review of 11 cross-sectional studies involving 4,194 participants across various regions of Saudi Arabia provides important insights into the multifaceted nature of adherence to antihypertensive medications. Reported adherence levels varied widely, with high adherence rates ranging from 34.3% to 86.1% and non-adherence reaching 67%. This variability is in line with the international literature and appears to be influenced by both patient-related and methodological factors, including the type of adherence measurement tool used.
A key finding is the substantial heterogeneity in adherence rates, partly due to the use of different validated tools (e.g., MMAS-4, MMAS-8, MGL, Hill-Bone, and MALMAS-8). Eventually, variations in measurement tools also affected the observed adherence rates. MMAS-8, which includes a wide range of items and can distinguish between intentional and unintentional non-adherence, in general, provides more comprehensive insights. On the other hand, shorter tools like the MMAS-4 and MGL deliver simpler evaluations that may overlook the complexities of patient behavior. An 86.1 percent adherence rate was the highest achieved with the MMAS-4, while 33 percent was the lowest with the MMAS-8, highlighting how the choice of scoring scale can strongly impact study findings.
The association between socio-demographic factors and medication adherence was consistently highlighted in the studies reviewed. Gender-related results were somewhat conflicting. Some studies found that women were more adherent [21,25-27,31], whereas other studies by Khayyat and Mahmoud reported lower adherence among female patients [32,33]. Furthermore, other studies by Alsolami, Almaghamsi, and Algabbani did not establish any link between sexuality and medication adherence [19, 24, 29]. This aligns with global trends where gender is not a consistent predictor of adherence. The reasons for this gender discrepancy remain unclear. This issue may contribute to differences in health consciousness, health literacy, or cultural aspects of health. However, more research is needed to validate these hypotheses and identify the best approaches to improving medication adherence rates among both men and women with chronic diseases.
A positive finding was observed in older adults. Several studies have reported a significant association between age and improved medication adherence, especially among those over 50 years [21,23,25,26]. This could be due to increased health awareness, the severity of the disease, or the presence of caregivers. This finding is in line with earlier research suggesting that improvements in adherence related to age may be influenced by factors such as assistance with medication management and greater involvement in healthcare systems [34]. Another possible reason is holding different opinions and beliefs about medication adherence, influenced by cultural and socio-economic aspects. Furthermore, other studies have indicated that being younger than 50 years is a risk factor for low medication adherence [19,21-24,29].
Mixed results regarding the relationship between marital status and medication adherence were noticed. A weak association was found between being married and adherence to medications [25, 29, 32]. This was further supported by findings from Thirunavukkarasu et al., who indicated that unmarried patients had significantly lower adherence to antihypertensive medication compared to their married counterparts [22]. A further study by Khayyat et al. also confirmed that married patients were more likely to adhere to their medication than others [32]. Conversely, a finding by Alkhamis et al. observed that marriage did not significantly help patients in following their medication regimens [35]. However, married individuals generally demonstrated better adherence, likely due to the emotional and logistical support received from their partners [25,29].
Education was positively linked to adherence in several studies. Patients with higher levels of education may have a better understanding of the consequences of uncontrolled hypertension and the benefits of adherence [19,20,26,29]. In support of this, Alsofyan et al. reported that patients with low education levels and those who were illiterate showed lower adherence to their medications [25]. Moreover, Abdelhalim et al. found that patients who were aware of their treatment plans and knowledgeable about their conditions were more likely to adhere to their medication regimens [21]. It is important to note that, in some cases, highly educated individuals may also question the need for medication due to their greater awareness of potential side effects [19, 29, 36]. Despite this, many studies have shown that higher levels of education were not necessarily associated with medication adherence [24, 27, 28]. This observation is similar to other Saudi studies published earlier [31,37,38].
A significant contradiction in research related to medication adherence occurred when patients were diagnosed with multiple chronic conditions and comorbidities. Our review shows that most of the included studies reported no significant association between comorbidities and medication adherence [22, 24-26]. This may be due to possible comorbidities associated with old age and polypharmacy medications, which possibly increase the chance of forgetting the time of taking the medication. Other possibilities include being careless with their medications or not being accessible most of the time. This finding was also supported by earlier studies by Khayyat and Alkhamis, which showed that patients with multiple comorbidities were less likely to be adherent to medication than patients with a single disease [32,35].
Occupation and monthly income were positively associated with adherence in several studies. Employees in the private sector showed better adherence in the Alruwaili study [28]. However, the Almaghamsi study reported that government employees showed higher medication adherence compared to others [29]. This may reflect both increased health literacy and access to employer-sponsored healthcare benefits. The relationship between income and adherence is complex, and most reviewed studies found no significant association between patients’ monthly income and medication adherence [19,20,22-24,26-28]. Interestingly, Alkhamis et al.’s study reported that patients with low monthly income (<5,000 SR) were more likely to have lower medication adherence, whereas those with high monthly income (>10,000 SR) had higher medication adherence [35]. We assume that higher monthly income facilitates better access to healthcare resources, consequently improving adherence. This finding was consistent with a study conducted in Makkah among patients with various chronic diseases, which found that those with a low monthly income (< 6,000 SR) had twice the risk of non-adherence to medications [37]. Non-adherence was also two times detected in patients who purchased their medication at their own expense compared to those who had insurance or governmental coverage [37].
Future directions
This review points out several critical gaps in the current understanding of antihypertensive medication adherence in Saudi Arabia. To fortify future research, there is a necessity for study designs that go beyond simple cross-sectional snapshots. Longitudinal studies would help monitor adherence trends over time and identify authentic predictors, while qualitative and mixed-methods approaches are vital for revealing the cultural, social, and personal factors that lead to non-adherence—insights that cannot be fully captured by surveys alone. Future initiatives should also transition towards creating and assessing culturally tailored interventions. Examples include faith-aligned strategies to facilitate medication adherence during Ramadan, family-oriented educational programs, and digital health tools tailored to local communication platforms and Arabic dialects. Standardizing adherence measurement with validated instruments such as the MMAS-8, or a culturally adapted equivalent, would enhance comparability across studies and regions. Ultimately, targeted research is necessary for under-explored groups—such as younger men, individuals with limited health literacy, and residents of less-represented regions—to better comprehend their unique challenges and guide the development of focused interventions.
Limitations
The review presents several limitations that should be recognized. All studies included were cross-sectional, which limits the capacity to determine causal relationships between the identified factors and medication adherence. The majority of studies depended on self-reported adherence measures, which introduces potential recall and social desirability biases that could have inflated adherence estimates. Significant heterogeneity was also noted in the definitions and measurements of adherence, as well as in the characteristics of the study populations, complicating direct comparisons. Key contextual factors—such as access to medications, religious practices, and family-related influences—were inconsistently addressed across studies and may not have been comprehensively captured. Furthermore, excluding non-English publications raises concerns about language bias and may have led to the omission of pertinent findings from Arabic-language sources. Lastly, publication bias cannot be entirely dismissed, as studies that report significant results are more likely to be published and indexed in the utilized databases.
CONCLUSION
This literature review highlights the significant variability in medication adherence among hypertensive patients in Saudi Arabia, with reported adherence rates ranging from 33% to 86.1%. Regional disparities, measurement tools, and patient-related factors influence the variation. Key contributors to non-adherence include young age, low education, weak social support, and poor physician–patient relationships. The use of the Health Belief Model (HBM) adds a valuable dimension to understanding behavioral influences on adherence. To improve outcomes, healthcare providers must consider culturally sensitive strategies, reinforce patient education, and promote behavioral interventions tailored to individual beliefs and barriers. Implementing standardized tools (e.g., MMAS-8) alongside behavior-based frameworks (e.g., HBM) could improve adherence and enhance patient outcomes in hypertensive care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1NCD Risk Factor Collaboration (NCD-Ris C)Worldwide trends in blood pressure from 1975 to 2015: a pooled analysis of 1479 population-based measurement studies with 19.1 million participants Lancet 2017389375510.1016/S 0140-6736(16)31919-527863813 PMC 5220163 · doi ↗ · pubmed ↗
- 2James PA Oparil S Carter BL Cushman WC Dennison-Himmelfarb C Handler J 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)JAMA 2014 Feb 531155072010.1001/jama.2013.28442724352797 · doi ↗ · pubmed ↗
- 3Abboud M Karam S Hypertension in the Middle East: current state, human factors, and barriers to control J Hum Hypertens 2022364283610.1038/s 41371-021-00554-z 34075186 · doi ↗ · pubmed ↗
- 4Alshammari SA Alshammari AS Alshammari HS Ahamed SS Overview of hypertension in Saudi Arabia: A systematic review and meta-analysis Saudi Med J 202344109516410.15537/smj.2023.44.10.2023017837777271 PMC 10541986 · doi ↗ · pubmed ↗
- 5Saeed AA Al Hamdan NA Bahnassy AA Abdalla AM Abbas MA Abuzaid LZ Prevalence, awareness, treatment, and control of hypertension among Saudi adult population: A national survey Int J Hypertens 201120111741352191273710.4061/2011/174135 PMC 3168271 · doi ↗ · pubmed ↗
- 6Alenazi AM Alqahtani BA National and regional prevalence rates of hypertension in Saudi Arabia: a descriptive analysis using the national survey data Front Public Health 202311109290510.3389/fpubh.2023.109290537081959 PMC 10110943 · doi ↗ · pubmed ↗
- 7Al-Nuaim AR Population-based epidemiological study of the prevalence of overweight and obesity in Saudi Arabia, regional variation Ann Saudi Med 199717195910.5144/0256-4947.1997.19517377429 · doi ↗ · pubmed ↗
- 8Mc Mahon GT Alnasser M Alzouman H Aldakhil L Ababtain A Transforming Continuing Professional Development for Healthcare Professionals to Meet National Goals in Saudi Arabia J CME 2024131237861710.1080/28338073.2024.237861739011066 PMC 11249139 · doi ↗ · pubmed ↗