Engineering the mind-body medicine: making a case for a trauma-informed primary care system
Satish Boregowda, Inga Eanes, Rodney Handy

TL;DR
This paper suggests integrating trauma screening into primary care to improve patient outcomes through a structured, value-based system.
Contribution
The novel contribution is an engineering framework for a trauma-informed primary care system using ACEs screening and stress response data.
Findings
A trauma-informed primary care system can be modeled using ACEs screening and psychophysiological data.
Mental health professionals embedded in primary care settings can improve trauma evaluation and treatment referral processes.
An engineering-based design methodology is proposed to guide the implementation of trauma-informed care.
Abstract
This narrative study proposes an engineering framework to model a value-based, trauma-informed primary care system. It is based on the premise that effective patient outcomes could be achieved by screening for adverse childhood experiences (ACEs). The protocol involves the administration of the ACE survey and an in-person trauma evaluation by mental health professionals embedded within the primary care settings. The ACE evaluation is then followed by the collection of psychophysiological stress response data. Depending on the level of symptomatic somatization, patients are then referred to appropriate treatment modalities. An engineering-based robust design methodology is utilized to demonstrate a model of a trauma-informed primary care system. To be deployed, the proposed value-based systems model of medicine warrants further investigation with clinical and empirical studies.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
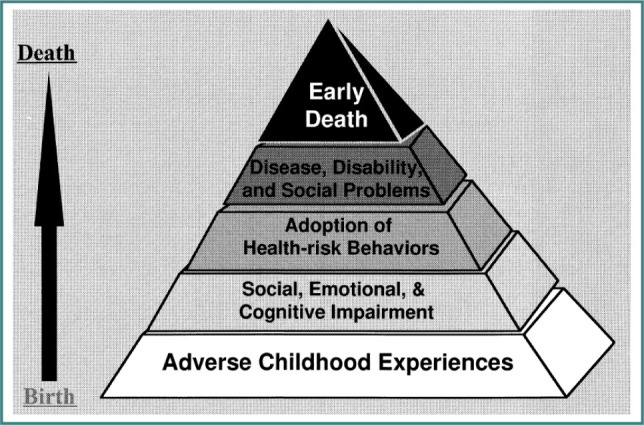 Figure 1
Figure 1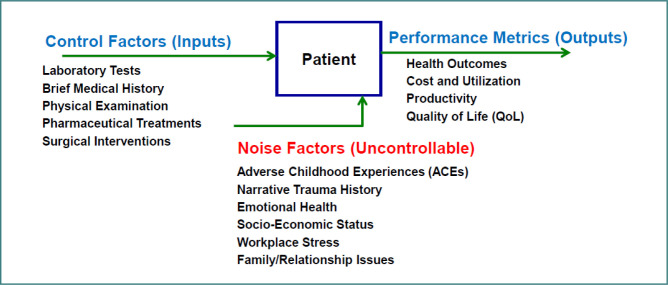 Figure 2
Figure 2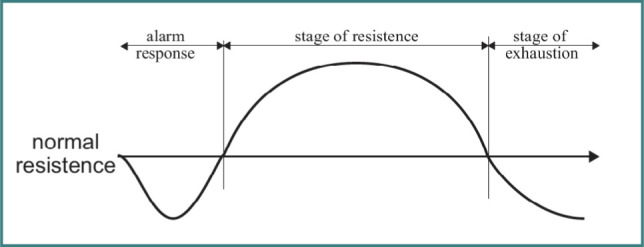 Figure 3
Figure 3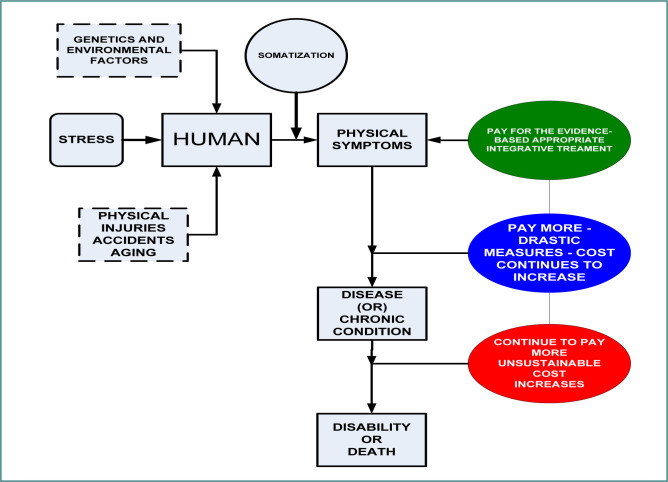 Figure 4
Figure 4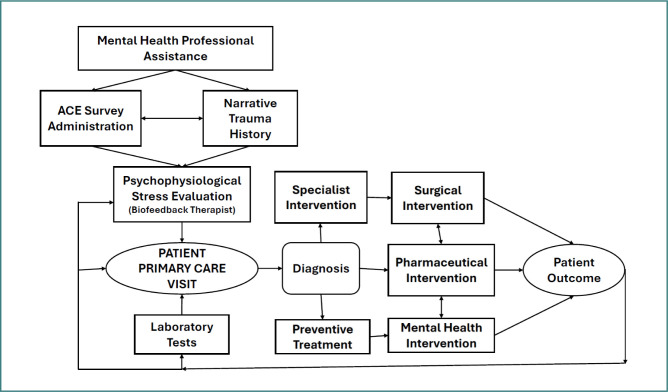 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsychotherapy Techniques and Applications · Psychosomatic Disorders and Their Treatments · Posttraumatic Stress Disorder Research
INTRODUCTION
The primary healthcare system is the entry point for all patients who exhibit a spectrum of physical symptoms resulting from acute to chronic illnesses. Some of these chronic illnesses include, but are not limited to, cancer, diabetes, heart conditions, autoimmune disorders, psychiatric conditions, and other related morbidities. The current system involves screening patients with results from pre-ordered laboratory tests and an office visit, followed by a referral to a specialist depending on the patient’s condition. While this system works, it falls short in terms of patient outcomes, cost, and utilization. In addition to physical examination of symptoms, it is critical to evaluate patients’ biopsychosocial history. It is hypothesized that the hidden biopsychosocial history plays a critical role in the development of symptoms leading to chronic illnesses. A large-scale (approximately 18,000 subjects) longitudinal study conducted by the Kaiser-Permanente/Center for Disease Control (KP/CDC) has established a strong correlation between adverse childhood experiences (ACEs) or household dysfunction and adult-onset chronic illnesses leading to early death, as shown in Figure 1. The ACE survey questions are provided in Appendix A, and the readers are encouraged to refer to the CDC/KP study [1] for further details.
Another study by Felitti [2] demonstrated that screening for ACEs, along with a detailed health appraisal process followed by appropriate therapeutic modalities, has contributed to reduced healthcare costs and utilization. It is suggested that 70% of diagnoses stem from the narrative patient history [3], which is captured in a 350-question questionnaire. While it is possible to implement this approach in an experimental setting, it would become cumbersome to deploy a 350-question health appraisal process in an operational primary care environment due to time and operational constraints. Furthermore, implementing this online might also lead to ethical, privacy, and technical data breach issues. Instead of a detailed health appraisal, it is easier to implement an in-person ACE evaluation. It has been shown that there is a relationship between ACEs and the victim’s self-perception and character [4]. With the help of this trauma narrative history, childhood information can be captured in an in-person interview by a mental health professional. The interview protocol is provided in Appendix B and can be further refined using the reference [5].
Potential influences throughout the lifespan of adverse childhood experiences (ACEs) [1]
Parameter (P) diagram for trauma-informed primary care
This proposed systems model would support physicians and mental health professionals embedded within the primary care system working together as a team to address and treat the root causes of illness, rather than focusing on physical symptoms. A framework for implementing this holistic approach using a quality engineering-based robust design methodology is described in the next section.
Robust design in the primary care system
A robust design methodology is a quality-engineering-based tool used in design and manufacturing to integrate quality into product design at an early stage of the production process. This is based on the premise that early intervention or prevention is better than cure, as advocated by the renowned quality management expert Edward Deming [6]. The production professionals on the factory floor who are well-informed about the supplier parts or raw materials can transform them into a valuable final product with less rework, scrap, and lower costs. By applying this value-based Quality Management principles to the healthcare system, the patients are analogous to machine parts or raw materials with detailed SOW (statement of work or work history) being supplied to the production personnel on the factory floor, who are like physicians, physician assistants, nurses, mental health professionals, and specialized physicians in the healthcare system [6,7]. In robust design, the control factors are the inputs to the system and are within the control of the physicians and other primary care health professionals. The ACEs, emotional health, workplace stress, and family and relationship issues are some of the noise factors that contribute to a larger portion of negative effects on the performance metrics or outputs (patient outcomes, cost, and utilization). The performance metrics (outputs) include health outcomes, cost, utilization, and productivity. These three factors are shown in the parameter diagram, commonly called the P-diagram, shown in Figure 2.
In this robust design, the word ‘parameter’ is equivalent to ‘factor’, and thus, we have the parameter (P) diagram. Several parameters (or factors) can influence the product’s quality characteristic or response [8,9]. With the implementation of robust design, physicians would work with supplier parts or materials (the patients in this case) with full information about their concealed defects, the hidden traumatic experiences.
STRESS AND ADVERSE CHILDHOOD EXPERIENCE
Stress has been defined as a nonspecific response of the body to any demand, and the ability of the body to mount a stress response without causing negative health effects requires adequate levels of adaptation energy [10]. Using the adaptation energy, the human physiological system adapts to stressful conditions, a process defined as the general adaptation syndrome (GAS), as illustrated in Figure 3.
General adaptation syndrome (GAS) [8]
There is a period of alarm response followed by a stage of resistance, resulting in a final stage of exhaustion. The nervous system responds to external stimuli by altering physiological responses. One’s ability to respond and overcome stressful events is controlled by the hypothalamic-pituitary-adrenal (HPA) axis, which plays a major role in triggering stress response and affecting numerous other bodily functions. This HPA axis is greatly affected by adverse childhood experiences (ACEs), which can deplete adaptive energy, thereby reducing the individual’s capacity to cope with daily stressors in both work and living environments. Furthermore, there has been a surge in studies examining the impact of childhood adversity on the HPA axis and individual stress reactivity. Several studies have shown a strong relationship between childhood trauma and the alteration of the HPA axis that, in turn, affects the stress response [11,12]. Several biomarkers of adverse childhood experiences (ACEs) are summarized in a study that included peripheral physiological indicators such as blood pressure and heart rate [13].
Furthermore, repeated activation of the HPA system increases cortisol production and, over time, negatively affects brain circuitry and brain volume development [14,15]. It has also been linked to dysregulation of blood pressure and blood sugar, as well as reduced cognitive functioning [16]. Just as the brain interprets our level of safety to generate an internal state of calm or an excited response that prompts the body to release more cortisol for energy, the process of discerning safety also involves an exchange of energy—information—between individuals and their environment, particularly with the people with whom children have relationships [17]. The quality of the energetic exchange in familial relationships is a critical element of the adverse childhood experience. Children are born into the world ready to connect. Children living in stressful environments absorb the emotional energy of their parents, who are authority figures [17]. This adaptation to survival in childhood leads to an altered vagus nerve, as explained in polyvagal theory [18]. The undiagnosed disorders and illnesses attributed to stress from ACEs lead to a degradation of human performance and ultimately workplace productivity, eventually resulting in huge economic losses [19]. Socio-economic and family system conditions dictate one’s physiological stress response to daily life stressors. The chronic psychological distress transforms into a physiological condition that later becomes a disease state, which is called somatization [20].It is critical to have a mental health system within the primary care to diagnose and treat patients at different levels of somatization [21]. Humans are complex systems characterized by biopsychosocial dynamics of both the present and the past. The lack of complete information regarding patient medical history and mental health status leads to ineffective treatments and subsequent suboptimal patient outcomes, increased costs and utilization, and loss of human productivity, contributing to major economic losses to society, as depicted in Figure 4.
Stress and somatization in primary care patients
SYSTEMS MODEL OF MEDICINE
The integration of mental health into primary care requires systems thinking [22]. This would provide a quantitative framework to better understand the impact of biopsychosocial factors on health and healing. Furthermore, systems thinking not only provides a quantitative framework for developing data-driven models but also aids in developing an operational plan to better integrate mental health processes within primary care, as shown in Figure 5. The proposed process involves the following three major steps: the collection of ACE survey data and a narrative trauma history by a mental health professional, and a psychophysiological stress evaluation by a mental health professional certified in biofeedback.
Systems model of primary care with embedded mental health professionals to diagnose and treat the effects of ACEs
Step I: Adverse Childhood Experience (ACE) Survey
The ACE questionnaire, shown in Appendix A, is administered by mental health professionals. Patients must trust and feel comfortable with their care providers during this process.
Step II: Narrative trauma history
Mental health professionals collect a narrative trauma history of the patient in an in-person interview using the protocol in Appendix B. During this interview, patients would answer questions, interacting with social workers and/or clinical psychologists to do so in a safe environment. Patients should feel comfortable talking about their internal life struggles that are impacting their physiological conditions with mental health professionals more than with their physicians [23]. This is a very important step in diagnosing and treating a patient. In this regard, mental health professionals embedded within the primary care would play a critical role in transforming patient care.
Step III: Psychophysiological stress evaluation
Elevated stress levels lead to increased cortisol and other biochemical responses, resulting in cardiovascular metabolic dysregulation. This need needs to be quantitatively evaluated in terms of measurable peripheral physiological stress reactions in a medical setting. It involves collecting blood pressure, heart rate, finger skin temperature, electromyogram, and skin conductance level as shown in Appendix C (Figure S1) using the psychophysiological stress evaluation system. This step would be conducted by a mental health professional trained as a biofeedback therapist within the primary care setting. The protocol involves stress measurements at the end of three stages: relaxation (5 minutes), stressful Stroop task (10 minutes), and finally, recovery (5 minutes). Readers are encouraged to refer to the references [24,25] for details of the protocol.
CONCLUSION
The current review article proposes a value-based systems model of medicine to integrate a three-step assessment of patients entering the primary care system. This approach involves an evaluation of adverse childhood experiences and psychophysiological stress evaluation by mental health professionals embedded within the primary care system. It has been well established in the studies cited in this paper that adverse childhood experience leads to adult-onset illnesses. Furthermore, it has been recognized that ongoing psychosocial stressors exacerbate the stress-related illnesses that lead to chronic health conditions. The treatment of these conditions requires a comprehensive evaluation of patients followed by a multitude of therapeutic approaches involving mental health professionals embedded within the primary care system. It is critical that a narrative trauma history of patients, in addition to the laboratory test results, is considered in tandem for the diagnosis and subsequent treatment of health conditions. A value-based systems model of medicine is proposed as a viable replacement to the existing fee-for-service biomedical model to reduce healthcare costs, improve quality of care, and achieve better patient outcomes. However, integrating mental health professionals and sophisticated computerized data-collection technologies into the primary care system could make value-based systems medicine a reality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Felitti VJ Anda RF Nordenberg D Williamson DF Spitz AM Edwards V Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med 1998 May 1442455810.1016/s 0749-3797(98)00017-89635069 · doi ↗ · pubmed ↗
- 2Felitti VJ Health Appraisal and the Adverse Childhood Experiences Study: National Implications for Health Care, Cost, and Utilization Perm J 2019231802610.7812/TPP/18-026PMC 632655830624193 · doi ↗ · pubmed ↗
- 3Felitti VJ Private communication 2021 Mar 14
- 4Owusu J The impact of adverse childhood experience (ACE) on victim’s self-perception and character development in adulthood [dissertation]2024 Lynchburg (VA)Liberty University Available from: https://digitalcommons.liberty.edu/doctoral/5602
- 5Creswell JW Poth CN Qualitative inquiry and research design 2018 Thousand Oaks (CA)Sage Publications
- 6Deming WE Out of the crisis 1986 Cambridge (MA)MIT Press
- 7Taguchi G Introduction to quality engineering: designing quality into products and processes 1986 Tokyo (Japan)Asian Productivity Organization
- 8Ulrich K Eppinger S Product design and development 2019 New York (NY)Mc Graw-Hill