Diagnostic accuracy of an enzyme-based point-of-care test versus Nugent score for bacterial vaginosis among pregnant women attending routine antenatal care in Zambia
Sumire Sorano, Enesia Banda Chaponda, Massimo Mirandola, Ephraim Chikwanda, Vivian Mwewa, Joyce M. Mulenga, Mike Chaponda, Ludovica Ghilardi, Emma M. Harding-Esch, Chris Smith, Mitsuaki Matsui, Daniel Chandramohan, Mohamed Mahmoud Ali, Karel Blondeel, Magnus Unemo, Igor Toskin

TL;DR
A study in Zambia found that a point-of-care test for bacterial vaginosis among pregnant women had high specificity but low sensitivity compared to a standard diagnostic method.
Contribution
This study evaluates the diagnostic accuracy and operational feasibility of a point-of-care test for bacterial vaginosis in a resource-limited setting.
Findings
The OSOM® BVBlue® test had a sensitivity of 41.3% and specificity of 93.1% compared to the Nugent score.
Most pregnant women were willing to wait up to 20 minutes for test results.
Cold-chain requirements and short shelf life were identified as significant implementation challenges.
Abstract
Bacterial vaginosis (BV) is associated with adverse pregnancy outcomes. OSOM® BVBlue® is a chromogenic point-of-care (POC) test that detects sialidase, an enzyme produced by Gardnerella vaginalis and some other anaerobic bacteria associated with BV. This study, part of the World Health Organization’s global ProSPeRo study, aimed to evaluate the performance of this POC test compared with the Nugent score reference standard among pregnant women in Zambia. Additionally, the operational characteristics and patient acceptability of the POC test were evaluated. Pregnant women attending four health centres in Nchelenge, Zambia, for antenatal care between 15 February and 26 May 2023 participated. Clinician-collected vaginal swabs for OSOM® BVBlue® and Nugent scoring were obtained from each participant. POC test results were read independently by two staff members. Study staff completed a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
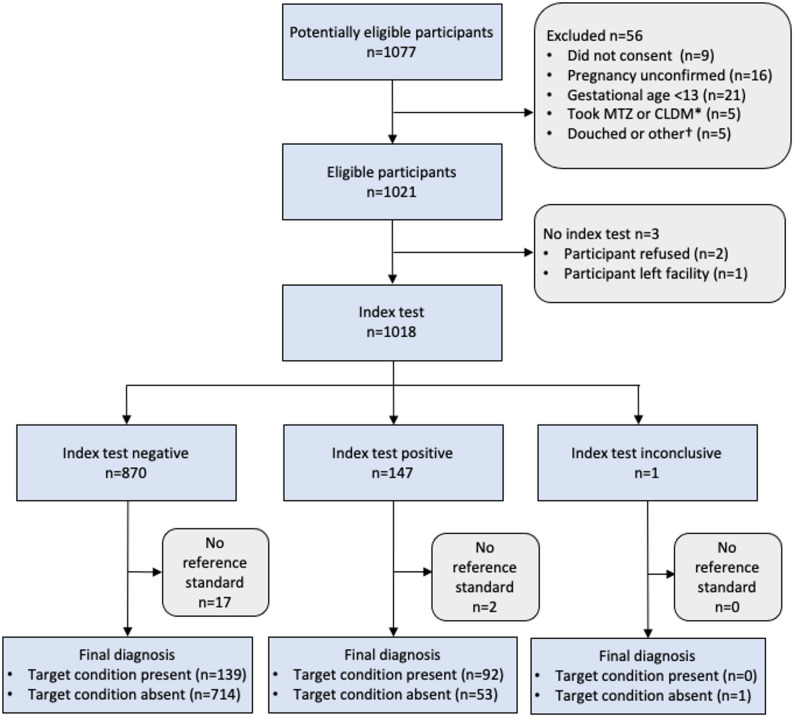 Figure 1
Figure 1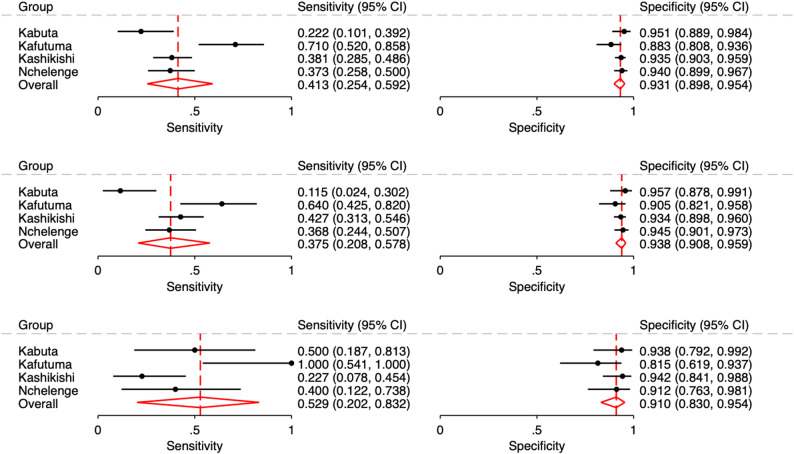 Figure 2
Figure 2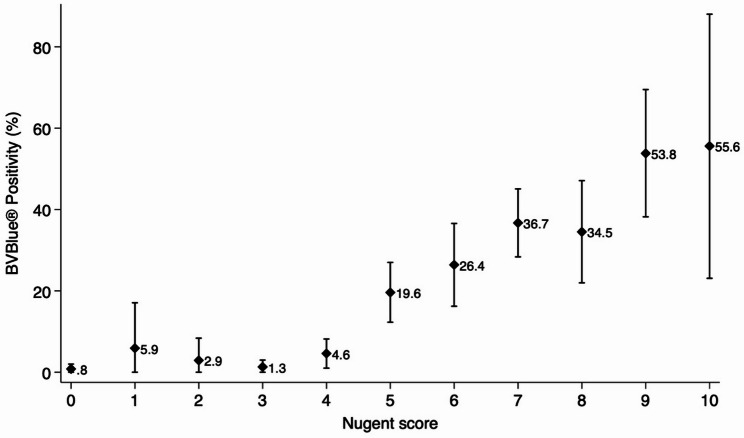 Figure 3
Figure 3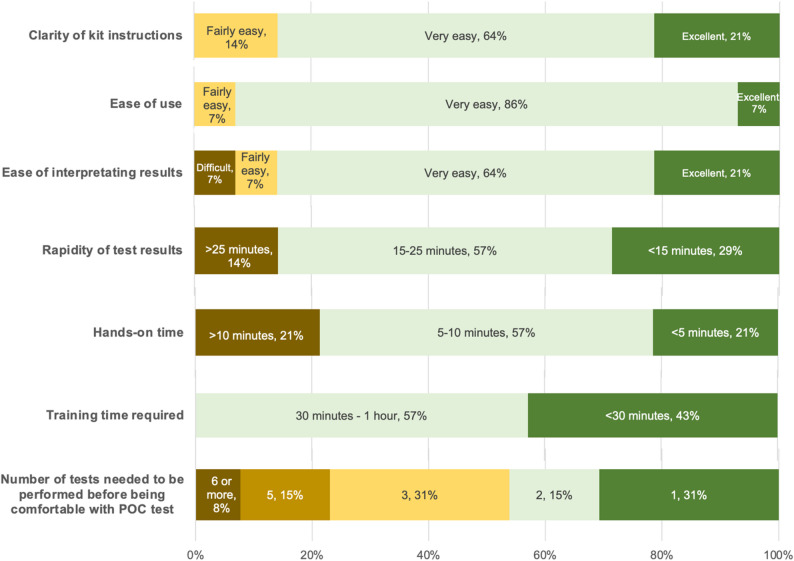 Figure 4
Figure 4- —Ministry of Education, Culture, Sports, Science and Technology, Japan
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsReproductive tract infections research · Neonatal and Maternal Infections · Bacterial Identification and Susceptibility Testing
Introduction
Bacterial vaginosis (BV), the most common urogenital condition in the world, is a vaginal dysbiosis that results from a depletion of commensal Lactobacillus species and an overgrowth of anaerobic bacteria [1, 2]. A recent systematic review and meta-analysis estimated that 25.1% (95% CI: 17.5–33.6%; N = 23,028) of pregnant women have BV in sub-Saharan Africa [3]. BV is associated with an increased risk of preterm delivery and spontaneous abortion [4], postpartum endometritis, and the acquisition and transmission of HIV and several other sexually transmitted infections (STIs) [5–7]. BV has also been associated with Human Papillomavirus infection and subsequent cervical pathology [8–10].
Despite these associations between BV and adverse pregnancy outcomes, screening and treatment of asymptomatic BV during pregnancy remain controversial. Meta-analyses of randomised controlled trials suggest that treating asymptomatic BV does not significantly lower the rates of preterm birth [11]. However, certain groups of women, especially those at higher risk for preterm birth, might benefit from treatment [12, 13].
Symptoms of BV may vary; some individuals remain asymptomatic, whereas others may experience thin, grey or white vaginal discharge with a strong fishy odor, itching, or burning during urination. Diagnosing BV in resource-limited settings is a challenge [14]. Use of Nugent scores, which involves microscopic examination of a vaginal swab, is considered the “gold standard” for laboratory diagnosis of BV, but it requires laboratory expertise that is uncommon in many resource-limited settings [15]. Syndromic-based diagnosis and treatment algorithms have been developed to aid the management of symptomatic cases of vaginal discharge in these settings [16]. However, because BV symptoms are non-specific and many affected women are asymptomatic, this approach cannot effectively identify all BV cases. In antenatal care, the sensitivity of these algorithms for treating BV among women with vaginal discharge ranges from 13% to 50%, whereas specificity spans 54% to 84% [17–19].
Point-of-care (POC) tests for BV are available and may facilitate rapid antenatal case-detection and treatment [15]. OSOM^®^ BVBlue^®^ (Sekisui Diagnostics, LLC, Massachusetts, USA) POC tests have a Clinical Laboratory Improvement Amendments (CLIA) waiver from the United States Food and Drug Administration, and have been used in clinics as part of sexual and reproductive services among women presenting with symptoms associated with BV. However, there is a lack of research evaluating this POC test for screening pregnant women. As part of the World Health Organization’s (WHO) global ProSPeRo study (Project on STI POC Testing), the primary objective of our study was to evaluate the clinical performance of an enzyme-based point-of-care technology in an antenatal care (ANC) setting in Zambia using OSOM^®^ BVBlue as an index test. We also assessed the operational characteristics and acceptability of this technology for patients and healthcare providers.
Methods
We registered this evaluation in the Pan African Clinical Trials Registry (PACTR202302766902029, dated 13/09/2022) and prepared this report in accordance with the Standard for Reporting Diagnostic Accuracy (STARD) guidelines [20]. We evaluated the performance of OSOM^®^ BVBlue^®^ compared with the Nugent score reference standard (≥ 7 indicating BV) for diagnosis of BV in pregnant women in rural Zambia. The study also evaluated the performance of an antigen-based POC test for trichomoniasis, the results of which have been reported elsewhere [21]. In brief, we present here the methods that are specific to the evaluation of OSOM^®^ BVBlue^®^. OSOM^®^ BVBlue^®^ is an enzyme-based POC test that includes a chromogenic substrate to detect sialidase, an enzyme produced by bacterial pathogens associated with BV, including Gardnerella vaginalis, Bacteroides, Prevotella and Mobiluncus. The POC test turns the sample swab blue or green in the presence of high levels of sialidase, whereas yellow indicates a negative result (absence of sialidase). Nugent scoring, the reference standard used in our study, is based on the presence of three bacteria morphotypes: Lactobacillus, Gardnerella, and Mobiluncus. It is the most commonly used diagnostic method in research settings, allowing for slides to be preserved and revisited, providing a quantitative analysis.
Study site
The study was conducted in four health centres that provide ANC in the Nchelenge District in Zambia: Kabuta, Kafutuma, Kashikishi, and Nchelenge. All centres were within the catchment area of Saint Paul’s Mission Hospital in Luapula Province, located in northern Zambia along the eastern shore of Lake Mweru [22].
Study participants
We recruited women attending ANC who were pregnant for no less than 13 gestational weeks and self-reported having: (i) not received metronidazole or clindamycin during their current pregnancy; (ii) not having a known allergy or other contraindication to metronidazole, and (iii) not used a vaginal cream or ointment product, douched or used vaginal lubricants within 72 h of recruitment. Pregnant women of all ages were eligible. Consistent with Zambian law, if potential participants were under 18 years of age, they would provide assent followed by their guardians consenting.
Procedures
The study design was aligned with the daily clinical practice of the study sites. All women who attended antenatal care were invited to participate until the target sample size was met. After obtaining written informed consent, we measured gestational age by sonography. For eligible participants, background and clinical information were collected by the study staff through participant interviews and antenatal records. Questions included self-reported vaginal symptoms (unusual vaginal discharge, pain during urination, itching or burning of the vulva) and other STI-related symptoms (sores, blisters, ulcers, warts or rashes in the genital area, lumps and bumps on the genitals, and lower abdominal pain). HIV and syphilis testing was conducted as part of routine ANC. HIV status or HIV/syphilis test results were obtained from the antenatal records. Additionally, we inquired about the patients’ willingness to wait for POC test results. This information was recorded in an electronic case report form designed in REDCap software [23].
Clinical staff collected four vaginal swabs from participants, one for each of the four assays: BV POC test, TV POC test (results reported elsewhere), Nugent scoring, and TV nucleic acid amplification test (NAAT) analysis (results reported elsewhere). The order of swab collection was randomised to prevent any bias related to the quantity of the vaginal sample that could arise from the sequence of collection. Considering that there were four swabs to be collected, there were 24 variations possible for sample collection. Prior to study initiation, we generated a random list of 1,100 sampling sequences. An independent researcher, not otherwise involved in the study, prepared opaque envelopes containing the sample collection order and participant IDs. Once participants were deemed eligible, they opened an envelope to reveal the swab order. For Nugent scoring, swabs were immediately rolled onto a glass slide after collection. POC test samples were promptly transported to a designated area and processed by clinical or laboratory staff in accordance with the manufacturer’s instructions. Results were independently read by two clinicians, or one clinician and one laboratory staff member, with each entering the results into REDCap sequentially without knowing the other’s reading. A separate study staff member then communicated the POC test results to participants in writing. If participants tested positive on the POC test based on at least one of the two readings, the study staff administered a 2-gram dose of metronidazole during the same visit, a recommended curative treatment for BV. To ensure that study staff used the POC tests as designed, we involved representatives of the POC test manufacturer in our onsite Investigators’ Meeting and training. The manufacturer had no further involvement. However, throughout the conduct of the study, laboratory technicians used a quality control kit as contained in each new box of OSOM^®^ BVBlue^®^ POC tests. At the end of the study, we provided a questionnaire to the clinic staff to evaluate the operational characteristics of the POC tests.
Laboratory analysis
Glass slide samples for Nugent scoring were transported to Saint Paul’s Mission Hospital where Gram staining was performed on the same day as collection. The Gram-stained slides were then sent to the Tropical Diseases Research Centre in Ndola, Zambia, (renamed as the National Health Research and Training Institute) where two laboratory staff members independently read them for Nugent scoring, blinded to all clinical information and POC test results. HIV and syphilis tests were conducted as part of routine antenatal care. Core tests^®^ ONE STEP Syphilis Test Kits (Core Technology, Atlanta, USA) were used for syphilis screening, and Determine^®^ HIV Test Kits (Abbott, Illinois, USA) were used for HIV screening.
Statistical analysis
We compared the POC test results (positive, negative, indeterminate, or invalid) against Nugent scores. Any indeterminate or invalid results, as well as instances of missing data, were excluded from the diagnostic accuracy analysis measures; we reported the number of invalid results separately. Pooled sensitivity, specificity, positive and negative likelihood ratios (LR), and positive (PPV) and negative predictive values (NPV) were estimated using a bivariate random effect meta-analysis model with logit transformation [24] which took into account the correlation between sensitivity and specificity. The model addresses both within-site variation and between-site variations. Stata midas and metadta packages [25–27] were used for the meta-analysis. Sub-group analyses were conducted based on presence of BV-associated symptoms. Additionally, PPV and NPV were estimated based on prevalence scenarios derived from study point estimates and 95% confidence intervals, a method used in other ProSPeRo studies [21]. Positive and negative LRs were plotted using Fagan’s nomogram in order to obtain post-test disease probability. Observed inter-rater agreement and Cohen’s Kappa were calculated. Additionally, we examined the relationship between Nugent scores and POC test positivity using descriptive statistics. To determine the specific bacterial morphotypes corresponding with BVBlue^®^ positivity, we employed univariate and multivariate logistic regression analysis. We used Stata 18.0 software [28] for our analyses.
Fig. 1STARD flow diagram. *Metronidazole or clindamycin use during current pregnancy; †any of the following within 72 h of visit: use of vaginal cream or ointment, spermicides, vaginal lubricants or feminine sprays, or douching
Results
We screened 1,077 potentially eligible pregnant women and enrolled 1,021 of them between February 15 and May 26, 2023. Three participants refused swab collection for both or either of the POC and reference test, and 19 glass slides were damaged accidentally in the laboratory prior to analysis. Ultimately, we obtained BV POC test results and Nugent scores from 999 women (Fig. 1). The majority of participants were aged 18–24 years with an age range of 14–46 years (Table 1). The majority of pregnant women, 71.0%, were married or living with a partner, whereas remaining participants, 29.0%, were single, separated, divorced, or widowed. In total, 56.4% of women were in their second trimester (13–27 gestational weeks), whereas 43.6% were in their third trimester (28–39 gestational weeks). Additionally, 8.7% were HIV sero-positive, and 14.9% were sero-positive for syphilis.
Table 1. Basic characteristics and clinical variables of participating pregnant women in Nchelenge, ZambiaBasic characteristics (N = 999)NumberPercentageFacility Kabuta13813.8% Kafutuma14314.3% Kashikishi43643.6% Nchelenge28228.2%Age group (years) 14–17353.5% 18–2454254.3% 25–3431931.9% 35–4610310.3%Marital status Single28028.1% Married or living with a partner70971.0% Separated, divorced or widowed90.9%Number of previous pregnancies 030130.1% 122222.2% 217717.7% 3+29929.9%Gestational age (in weeks) 13–2756356.4% 28–3943643.6%Symptoms associated with BV Unusual vaginal discharge626.2% Pain during urination434.3% Itching or burning of the vulva*15315.3% At least one symptom above†19319.4%HIV status Positive878.7% Negative90290.3% Unknown101.0%Syphilis point-of-care test Positive14914.9% Negative84684.7% Unknown40.4%*One participant was missing a value for this symptom†Two participants were missing values for at least one symptom
The POC test results and Nugent scores by facility are provided in Additional file 1 Table S2. Table 2 shows prevalence estimates based on Nugent score and diagnostic accuracy measures of the OSOM^®^ BVBlue^®^ compared with Nugent score. BV prevalence estimates ranged from 21.8% in Kafutuma to 26.1% in Kabuta. One sample produced indeterminate or invalid POC test results which was negative by Nugent score.
Figure 2 shows forest plots of sensitivity and specificity of the POC test, overall and by presence of symptoms. Sensitivity ranged from 22.2% in Kabuta to 71.0% in Kafutuma, and specificity ranged from 88.3% in Kafutuma to 95.1% in Kabuta. Pooled prevalence, sensitivity and specificity across facilities were 23.1% (95% CI 20.5–26.2%), 41.3% (95% CI 25.4–59.2%) and 93.1% (95% CI 89.8–95.4%), respectively. There was no evidence of a statistical difference in prevalence between individuals with and without BV-associated symptoms (24.4% [95%CI 18.3–30.4] versus 22.7% [95%CI 19.8–25.5]; relative ratio [RR] 1.08, 95% CI 0.78–1.48; P = 0.645). Similarly, there was no evidence of a significant difference in sensitivity between pregnant women with and without BV-related symptoms (52.9% [95%CI 20.2–83.2] versus 37.5% [95%CI 20.8–57.8], RR 1.41, 95% CI 0.69–2.87; P = 0.342). Table 3 shows PPV and NPV of the BV POC test based on prevalence scenarios of the minimum, maximum, and pooled prevalence of the study sites. Overall, PPV ranged from 61.5% to 67.8%, and NPV ranged from 81.9% to 85.7%. Fagan’s nomogram, plotted based on prevalence scenario and positive and negative LR (Additional file 1 Figure S1), illustrates these results. Observed inter-rater agreement of POC test results was 99.6% (995/999), with a Cohen’s Kappa of 0.984.
Table 2. Performance of OSOM^®^ BVBlue^®^ compared to Nugent score for bacterial vaginosis among pregnant women attending antenatal care overall and among asymptomatic and symptomatic participantsParticipant characteristics N Prevalence (%)(95% CI)†Sensitivity (%)(95% CI)Specificity (%)(95% CI) Overall (symptomatic and asymptomatic participants) Kabuta13826.1 (19.0–34.2)22.2 (10.1–39.2)95.1 (88.9–98.4) Kafutuma14221.8 (15.3–29.5)71.0 (52.0–85.8)88.3 (80.8–93.6) Kashikishi43622.2 (18.4–26.4)38.1 (28.5–48.6)93.5 (90.3–95.9) Nchelenge28223.8 (18.9–29.2)37.3 (25.8–50.0)94.0 (89.9–96.7)Pooled estimate99823.1 (20.5–26.2)41.3 (25.4–59.2)93.1 (89.8–95.4)Positive likelihood ratio = 6.0 (4.3–8.3)Negative likelihood ratio = 0.63 (0.48–0.83)Diagnostic odds ratio = 10 (6–16) Asymptomatic participants Kabuta9527.4 (18.7–37.5)11.5 (2.4–30.2)95.7 (87.8–99.1) Kafutuma10922.9 (15.4–32.0)64.0 (42.5–82.0)90.5 (82.1–95.8) Kashikishi36120.8 (16.7–25.3)42.7 (31.3–54.6)93.4 (89.8–96.0) Nchelenge23823.9 (18.7–29.9)36.8 (24.4–50.7)94.5 (90.1–97.3)Pooled estimate80322.7 (19.8–25.5)37.5 (20.8–57.8)93.8 (90.8–95.9)Positive likelihood ratio = 6.1 (3.9–9.4)Negative likelihood ratio = 0.67 (0.50–0.89)Diagnostic odds ratio = 9 (5–18) Symptomatic participants Kabuta4223.8 (12.1–39.5)50.0 (18.7–81.3)93.8 (79.2–99.2) Kafutuma3318.2 (7.0–35.5)100 (54.1–100.0)81.5 (61.9–93.7) Kashikishi7429.7 (19.7–41.5)22.7 (7.8–45.4)94.2 (84.1–98.8) Nchelenge4422.7 (11.5–37.8)40.0 (20.2–83.2)91.2 (76.3–98.1) Pooled estimate193*24.4 (18.3–30.4)52.9 (20.2–83.2)91.0 (83.0–95.4)Positive likelihood ratio = 5.9 (2.9–11.7)Negative likelihood ratio = 0.52 (0.24–1.10)Diagnostic odds ratio = 11 (3–42)Symptomatic participants had at least one of the following: unusual vaginal discharge, pain during urination, itching or burning of the vulva; *The sum of symptomatic and asymptomatic cases is not equal to the overall count; one case each in Kabuta and Kashikishi was missing symptom information†Prevalence is based on reference method. CI: confidence interval
Fig. 2. Forest plots of sensitivity and specificity of OSOM^®^ BVBlue^®^ compared to Nugent score for bacterial vaginosis among pregnant women attending antenatal care by health facility and overall in Nchelenge, Zambia
Table 3. Positive predictive value and negative predictive value of OSOM^®^ BVBlue^®^ based on prevalence scenarios among pregnant women attending antenatal care in Nchelenge, ZambiaPrevalence range (%)*Pooled sensitivity (%)Pooled specificity (%)Prevalence scenariosPositive predictive value (95%CI)Negative predictive value (95%CI) Overall (symptomatic and asymptomatic participants) 23 (21–26)41.393.12161.5 (53.6–68.8)85.7 (81.9–88.8)2364.2 (56.5–71.2)84.2 (80.1–87.5)2667.8 (60.4–74.4)81.9 (77.3–85.7) Asymptomatic participants 23 (20–26)37.593.82060.3 (49.6–70.1)85.7 (81.7–89.0)2364.4 (54.0–73.7)83.4 (78.9–87.1)2668.1 (58.0–76.7)81.0 (76.1–85.2) Symptomatic participants 24 (18–30)52.991.01856.3 (39.2–72.0)89.8 (80.5–94.9)2465.0 (48.1–78.7)85.9 (74.1–92.9)3071.6 (55.8–83.4)81.8 (67.9–90.6)*Prevalence is based on reference method; 95%CI: 95% confidence interval; Prevalence scenarios are based on the minimum and maximum of the observed site and pooled prevalence
Figure 3 shows the relationship between OSOM^®^ BVBlue^®^ positivity and Nugent scores,. The graph illustrates that BVBlue^®^ positivity increases with higher Nugent scores (0.8% [95%CI 0.0, 2.0%] for score 0, 19.6% [95%CI 12.3, 27.0] for score 5, 55.6% [95%CI 23.1, 88.8] for score 10). We analysed which bacterial morphotypes of Nugent scoring corresponded with BVBlue^®^ positivity. Table 4 presents the results of OSOM^®^ BVBlue^®^ positivity in relation to scores for each bacterial category. To differentiate the positive or negative correlation of these three bacterial categories being present, we employed multivariate logistic regression models to generate an adjusted odds ratio (aOR) that reflected a score-response relationship between Lactobacillus score and OSOM^®^ BVBlue^®^ positivity. Even a mild reduction of Lactobacillus (score 1 = 5–30 per field) was associated with increased OSOM^®^ BVBlue^®^ positivity (aOR 3.25 [95%CI 1.58, 6.66], p value = 0.001), with a more substantial increase observed in the absence of Lactobacillus (score 4: aOR 11.40 [95%CI 4.26, 30.48], p value = < 0.001). Conversely, there was no evidence of a significant increase of OSOM^®^ BVBlue^®^ positivity with a mild presence of Gardnerella (score 3 = 5–30 per field: aOR 2.25 [95%CI 0.59, 10.12], p value = 0.22), but increased sharply when Gardnerella was abundant (score 4 = > 30 per field: aOR8.47 [95%CI 2.47, 29.02], p value = 0.001). The presence of Mobiluncus showed an association with OSOM^®^ BVBlue^®^ positivity in the univariate analysis. However, this relationship was no longer detectable after adjusting with Lactobacillus and Gardnerella scores.
Fig. 3. Association of OSOM^®^ BVBlue^®^ positivity and Nugent score among pregnant women attending antenatal care in Nchelenge, Zambia
Table 4. Association of OSOM^®^ BVBlue^®^ positivity and subcategories of Nugent scores among pregnant women attending antenatal care in Nchelenge, Zambia N POCT positive (%)Unadjusted OR95% CIp valueAdjusted OR95% CIp valueLactobacillus Score055214 (2.5%)11117830 (16.9%) 7.79 4.03,** 15.07** < 0.001
3.25 1.58,** 6.66** 0.001 210127 (26.7%) 14.02 7.03,** 27.95** < 0.001
4.95 2.30,** 10.64** < 0.001 313962 (44.6%) 30.94 16.52,** 57.94** < 0.001
11.67 5.82,** 23.40** < 0.001 42812 (42.9%) 28.82 11.51,** 72.14** < 0.001
11.40 4.26,** 30.48** < 0.001 Gardnerella Score02633 (1.1%)11170 (0.0%)112421 (2.4%)2.110.21, 20.810.521.250.12, 12.890.8531826 (3.3%)2.950.73, 11.970.132.250.59, 10.120.224504135 (26.8%) 31.7 9.99,** 100.64** < 0.001
8.47 2.47,** 29.02** 0.001 Mobiluncus Score085194 (11.0%)11104 (40.0%) 5.37 1.49,** 19.37** 0.01 1.390.36, 5.420.635213747 (34.3%) 4.21 2.78,** 6.35** < 0.001 1.360.86, 2.160.184
Nearly all women, 97.9% (978/999), stated they would be willing to wait up to 20 minutes for a POC test result, and 59.2% of women (591/999) up to 30 minutes. Figure 4 contains the results of the study staff questionnaire regarding the operational characteristics of OSOM^®^ BVBlue^®^. Of the 14 study staff members involved, all found the POC test easy to use and instructions clear, 13 felt the results were easy to interpret, and 12 reported test results were available within 25 minutes.
Fig. 4. Operational characteristics of the OSOM^®^ BVBlue^®^ assessed by study staff (N = 14)
Discussion
In this ANC setting in Zambia, OSOM^®^ BVBlue^®^ demonstrated sub-optimal sensitivity at 41.3%, and moderate-to-high specificity at 93.1%. Overall sensitivity in this study was at the lower end of the range compared to past studies that also used Nugent score as the reference standard (37–100%), whereas the specificity fell within the reported range (92.1–100%) [29–37] (Additional file 1 Table S1). Past studies targeted women with symptoms or risk factors and who were predominantly not pregnant, whereas our study uniquely evaluated the POC test as a general screening tool for pregnant women. Diagnostic accuracy of the POC test did not differ between symptomatic and asymptomatic participants. However, sensitivity varied significantly across different health centres, from 22.2% in Kabuta to 71.0% in Kafutuma. Kafutuma exhibited highest sensitivity at 71%, but it had the lowest specificity (88.3%) among the four health centres. In contrast, Kabuta had the highest specificity (95.1%) and lowest sensitivity (22.2%) among the centres. This suggests that Kafutuma tended to interpret POC test results more often as positive, whereas Kabuta tended to interpret them as negative. Indeed, the overall POC test positivity in Kafutuma was 24%, compared to 9% in Kabuta, despite Kabuta having a higher prevalence of BV as determined by Nugent score (Kafutuma: 22%; Kabuta: 26%). The interpretation of the colour of the liquid in the testing vessel could be influenced by factors such as room lighting or background colour. Study enrolment and testing were typically conducted in the morning, during which time the health centres relied on natural light from windows. Another potential explanation could be variation in clinical staff practices. However, there is no evidence to support this, as all staff members underwent identical instructions and collective training prior to the commencement of the study. Additionally, a single coordinator supervised the enrolment process each day across all four health centres. It is important to note that both Kabuta and Kafutuma had a relatively small number of participants (Kabuta:138, Kafutuma: 143), leading to greater uncertainty and wider confidence intervals.
Although the POC test sensitivity was sub-optimal, the functional information provided by this test still holds value. BV is characterised by a disturbance of the normally Lactobacilli-dominated vaginal flora, but its precise aetiology of causing adverse pregnancy and birth outcomes remains unknown, and current BV diagnosis based on morphological aspects might not capture the full picture. Sialidase, an enzyme produced by Gardnerella and some additional anaerobic bacteria, whose activity the OSOM^®^ BVBlue^®^ targets, cleaves terminal sialic acid residues off of vaginal mucosal glycans and might play a role in the attachment and colonisation of vaginal pathogens [38]. Sialidase is also shown to impair local immune defences, as indicated by its association with increased vaginal IL-1β and inhibition of IL8 and neutrophils [39]. A clinical study showed that among those with BV diagnosed by Nugent score, sialidase levels in early gestation correlated with the risk of preterm birth and late miscarriages [38]. Therefore, sialidase has a potential to be used as a biomarker of BV and its associated adverse pregnancy outcomes. Our study found a relatively high specificity (93.1%), with most false positive results corresponding to intermediate Nugent scores (4–6) (47/53). For diagnosing intermediate or higher Nugent score, the POC test was 98.7% sensitive.
From an operational standpoint, the enzyme-based POC test for BV was user-friendly, requiring minimal training and delivering results within 25 minutes in the majority of cases. However, while 85% (12 of 14) of study staff rated the ease of interpreting the POC test results as ‘very easy’ or ‘excellent’, one staff member (7%) found it ‘difficult,’ and another described it as ‘fairly easy.’ While OSOM^®^ BVBlue^®^ is a qualitative test, we observed a spectrum of colour changes from yellow (negative) to green and blue (positive). Some results were clearly blue, while others were greenish-yellow, making some diagnoses difficult. Additional file 1 Figure S2 contains photos to illustrate the range of intermediate colours among false positive cases.
The requirement of maintaining OSOM^®^ BVBlue^®^ kits in refrigerated conditions from 2° to 8 °C proved to be costly and operationally difficult in rural Zambia. An additional challenge was the relatively short shelf-life (six months) of the OSOM^®^ BVBlue^®^ kits. This was manageable in our study setting, but could prove difficult if deployed as part of routine ANC, necessitating frequent shipments with the risk of stockouts or increased waste. Addressing these challenges will be crucial for deployment of enzyme-based POC tests in resource-limited rural settings. These challenges may be less of an issue if the kits are used in resource-limited urban areas.
To the best of our knowledge, there are no Target Product Profiles (TPPs) for POC tests to diagnose BV. Findings from this study are valuable for development of minimal and optimal product profiles for POC test for BV. The development of these profiles, in turn, may support further research and development of POC tests for this highly prevalent condition and its important sexual and reproductive health sequelae.
Conclusion
OSOM^®^ BVBlue^®^ showed sub-optimal sensitivity but relatively high specificity. Logistical challenges due to cold-chain requirements and short shelf-life need to be addressed for its effective routine use in resource-limited rural settings. The findings from this study are vital to the further development of POC tests that target BV.
Supplementary Information
Below is the link to the electronic supplementary material.
Supplementary Material 1
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gillet E, et al. Bacterial vaginosis is associated with uterine cervical human papillomavirus infection: a meta-analysis. BMC Infect Dis. 2011;11.10.1186/1471-2334-11-10PMC 302369721223574 · doi ↗ · pubmed ↗
- 2Gillet E, et al. Association between bacterial vaginosis and cervical intraepithelial neoplasia: systematic review and meta-analysis. P Lo S One. 2012;7.10.1371/journal.pone.0045201 PMC 346277623056195 · doi ↗ · pubmed ↗
- 3World Health Organization. Bacterial vaginosis. 2023. https://www.who.int/news-room/fact-sheets/detail/bacterial-vaginosis. Accessed 10 Dec 2025.
- 4World Health Organization. Laboratory and point-of-care diagnostic testing for sexually transmitted infections, including HIV. 2023. https://www.who.int/publications/i/item/9789240077089. Accessed 10 Dec 2025.
- 5World Health Organization. Guidelines for the management of symptomatic sexually transmitted infections. 2021. https://iris.who.int/bitstream/handle/10665/342523/9789240024168-eng.pdf. Accessed 10 Dec 2025.34370424 · pubmed ↗
- 6Chaponda EB, Bruce J, Michelo C, Chandramohan D, Chico RM. Assessment of syndromic management of curable sexually transmitted and reproductive tract infections among pregnant women: an observational cross- sectional study. BMC Pregnancy and Childbirth 2021;21.10.1186/s 12884-021-03573-3PMC 784701433516183 · doi ↗ · pubmed ↗
- 7Bossuyt PM, Reitsma JB, Bruns DE, Gatsonis CA, Glasziou PP, Irwig L, Lijmer JG Moher D, Rennie D, de Vet HCW, Kressel HY, Rifai N, Golub RM, Altman DG, Hooft L, Korevaar DA, Cohen JF. F. the S. G. STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies. 2015. https://www.equator-network.org/reporting-guidelines/stard/. Accessed 10 Dec 2025.
- 8Zambia Statistics Agency. 2022 Census of population and housing. 2022. https://www.zamstats.gov.zm/2022-census. Accessed 10 Dec 2025.