Effect of Sodium Restriction on Cardiovascular Outcomes in Patients With Hypertension and Heart Failure: A Systematic Review and Meta-Analysis
Ayman Alqurain, Omer H Al-Hasani, Turki A Alghamdi, Jood Alsaadi, Adel M Hakami, Naif A Alfahed, Yousef Z Hejazi, Qudama A Al-Hitawi, Abdulrahman M Asiri, Gassan M Htaimesh, Abdelrahman M Mohamed, Mohammed S Alraddadi, Mohamed F Alqahtani, Ali S Metwaly, Abrar Alqurashi

TL;DR
This study finds that sodium restriction helps people with high blood pressure but may be harmful for those with heart failure, suggesting personalized dietary advice.
Contribution
The study reveals a J-shaped relationship between sodium intake and mortality in heart failure patients, challenging uniform dietary guidelines.
Findings
Sodium restriction reduces mortality risk in hypertension but shows no benefit in heart failure.
Low sodium intake in observational studies is linked to increased mortality risk (HR, 1.20).
Aggressive sodium restriction (<1.5 g/day) may be detrimental in heart failure patients.
Abstract
Dietary sodium restriction is a cornerstone of cardiovascular disease management guideline recommendations. However, sodium restriction's impact on hard clinical endpoints in patients with heart failure remains controversial, showing conflicting results compared to the established benefits in essential hypertension. A systematic review and meta-analysis of randomized controlled trials (RCTs) and observational cohort studies evaluating the effect of sodium restriction on all-cause mortality and cardiovascular hospitalization was conducted. Databases were searched through December 2025. Random-effects models were used to pool hazard ratios (HR) with 95% confidence intervals (CI). Heterogeneity was assessed using the I2 statistic, and potential bias was evaluated using the Cochrane Risk of Bias 2 (RoB 2) tool and Newcastle-Ottawa Scale. A total of 20 studies (11 RCTs, nine observational…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
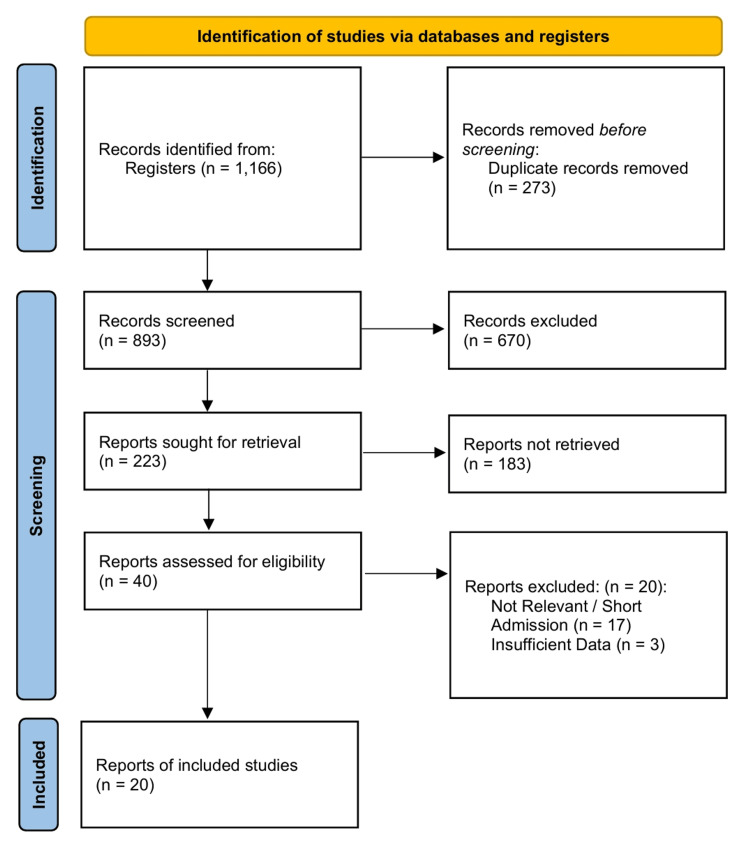 Figure 1
Figure 1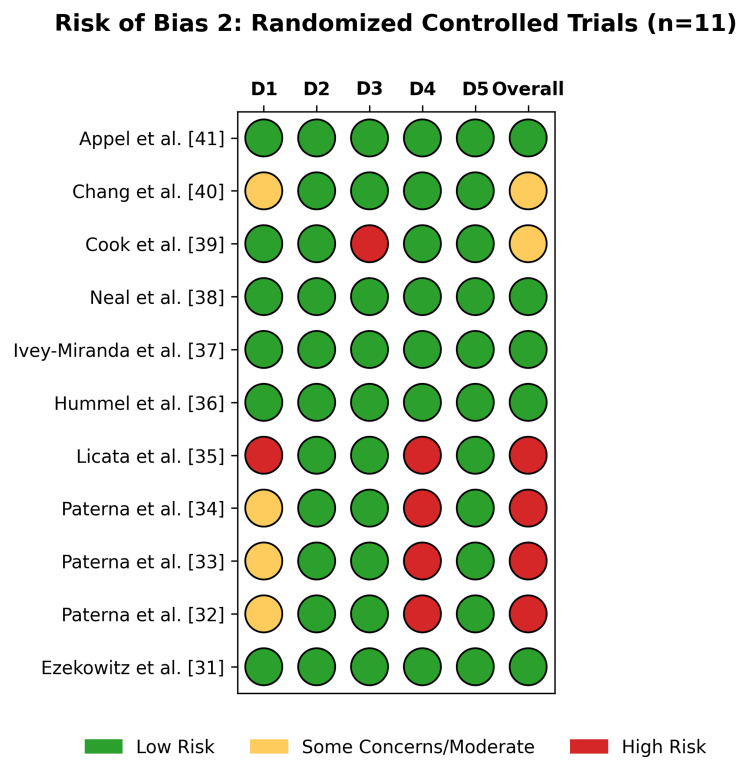 Figure 2
Figure 2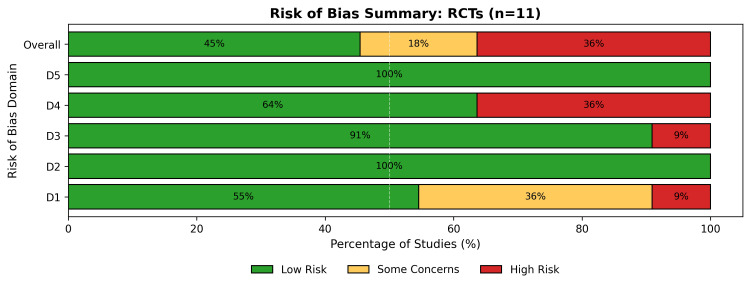 Figure 3
Figure 3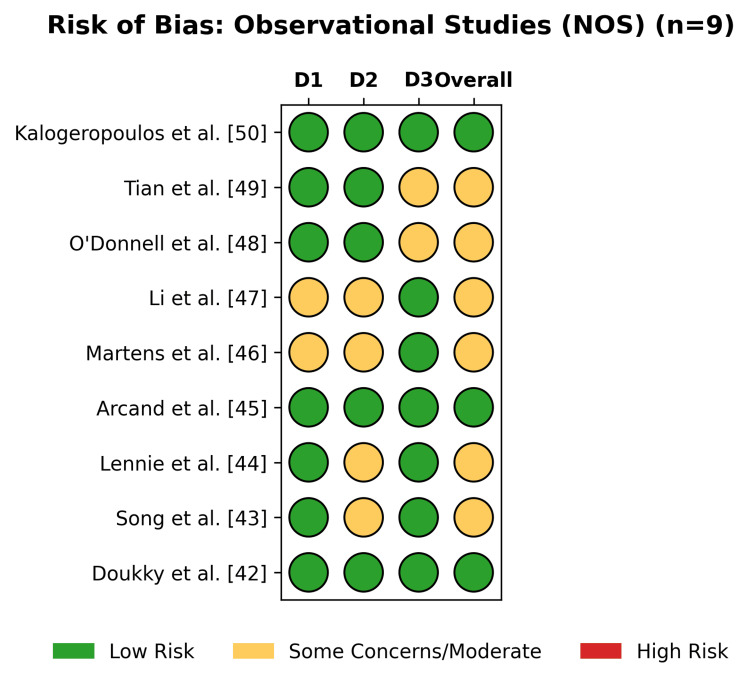 Figure 4
Figure 4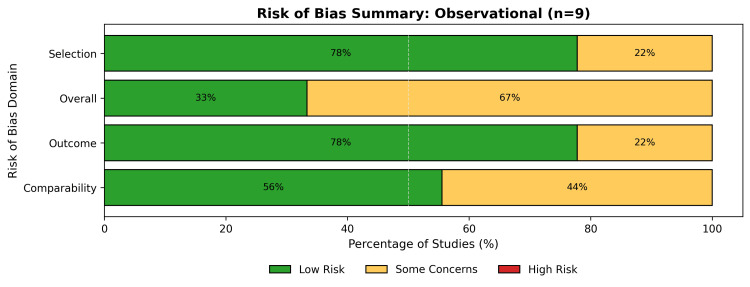 Figure 5
Figure 5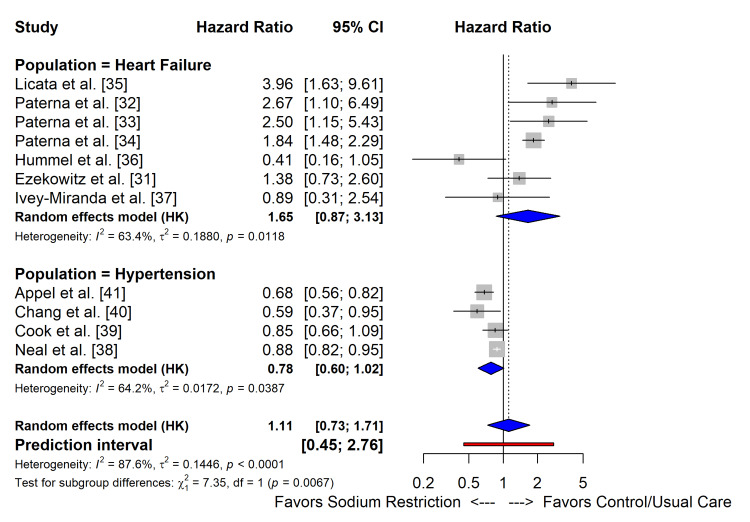 Figure 6
Figure 6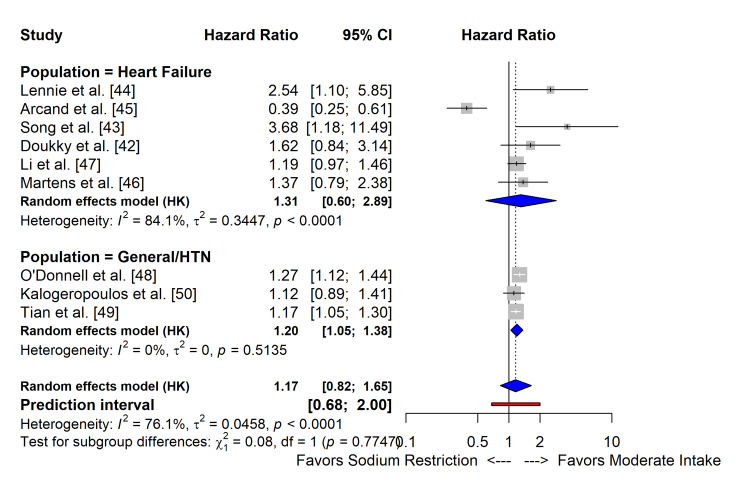 Figure 7
Figure 7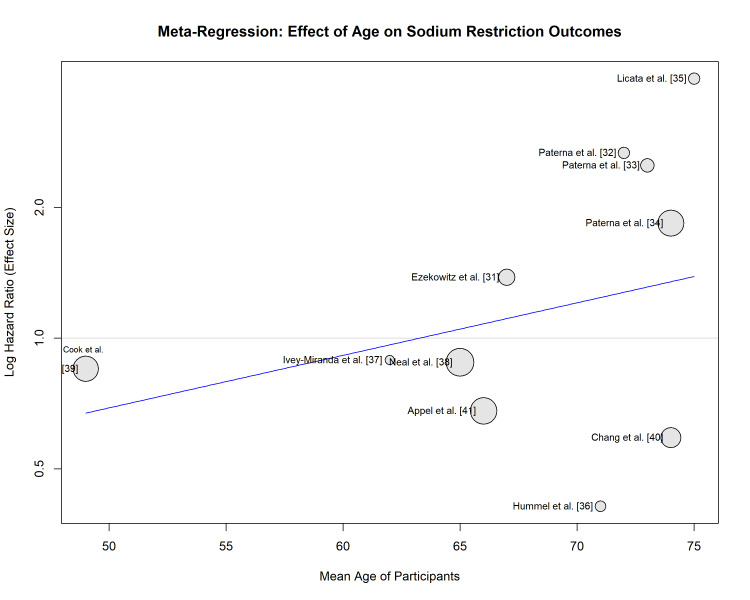 Figure 8
Figure 8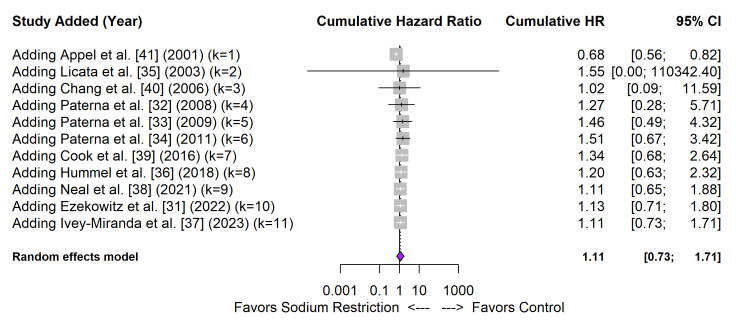 Figure 9
Figure 9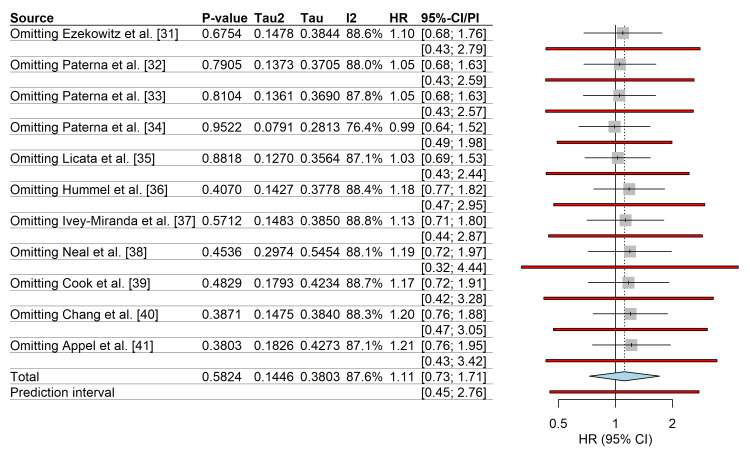 Figure 10
Figure 10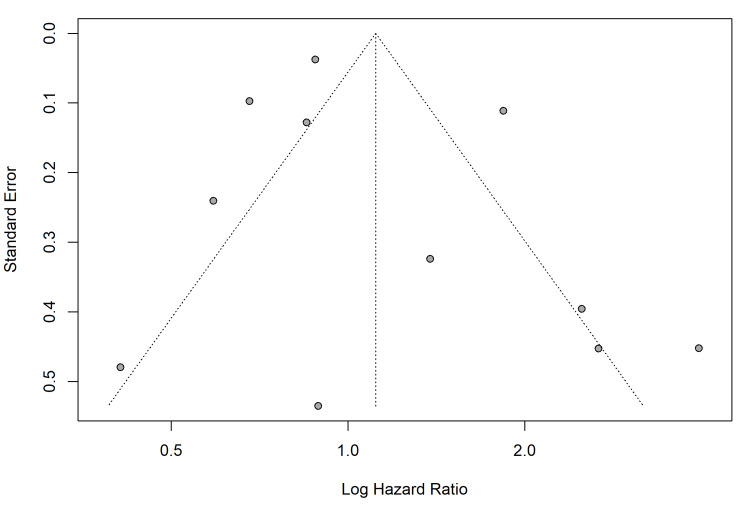 Figure 11
Figure 11| Study, year | Design | Population | Sample size (N) | Sodium intervention/exposure group | Comparator/ reference group | Sodium assessment method | Primary clinical outcomes reported | |
| RCTs | Heart failure population | |||||||
| Ezekowitz et al., 2022 (SODIUM-HF) [ | Multicentre RCT | Chronic HF (NYHA II-III) | 806 | <1500 mg/d (dietary counseling) | Usual care | 3-day food record | Mortality, CV hospitalization, ED visit | |
| Ivey-Miranda et al., 2023 [ | RCT | Chronic HFrEF | 70 | <2000 mg/d | <3000 mg/d | 24-hour urinary excretion | HF readmission, all-cause death | |
| Hummel et al., 2018 (GOURMET-HF) [ | Pilot RCT | Post-discharge HF | 66 | Home-delivered DASH meals (1500 mg/d) | Usual care | Provided meals/food diaries | 30-day HF readmission, mortality | |
| Paterna et al., 2011 (SMAC-HF) [ | RCT | Compensated HF (NYHA III) | 1,771 | Moderate sodium (2.8 g/d) + HSS | Low sodium (1.8 g/d) | Dietary counseling | Readmission, mortality | |
| Paterna et al., 2009 [ | RCT | Compensated HF | 410 | Low sodium (1.8 g/d) | Moderate sodium (2.8 g/d) | Dietary counseling | Readmission, mortality | |
| Paterna et al., 2008 [ | RCT | Compensated HF | 232 | Low sodium (1.8 g/d) | Moderate sodium (2.8 g/d) | Dietary counseling | Readmission, mortality | |
| Licata et al., 2003 [ | RCT | Refractory HF (NYHA IV) | 107 | Moderate sodium (2.8 g/d) + HSS | Low sodium (1.8 g/d) | Dietary counseling | Mortality | |
| Hypertension/general population | ||||||||
| Neal et al., 2021 (SSaSS) [ | Cluster RCT | Hypertension/stroke Hx | 20,995 | Salt substitute (75% NaCl/25% KCl) | Regular salt (100% NaCl) | 24-hour urinary excretion | Stroke, MACE, all-cause death | |
| Cook et al., 2016 (TOHP I/II) [ | RCT (long-term F/U) | Pre-hypertension | 2,974 | Sodium reduction intervention | Usual care | Multiple 24-hour urinary excretions | All-cause mortality | |
| Chang et al., 2006 [ | Cluster RCT | Elderly veterans | 1,981 | Potassium-enriched salt | Regular salt | Kitchen-based records | CV mortality | |
| Appel et al., 2001 (TONE) [ | RCT | Elderly with hypertension | 681 | Sodium reduction intervention | Usual care | 24-hour urinary excretion | Composite of BP control and CV events | |
| Observational cohort studies | Heart failure population | |||||||
| Doukky et al., 2016 (HART) [ | Cohort (propensity matched) | Symptomatic HF | 833 | <2500 mg/d | ≥2500 mg/d | Food frequency questionnaire | Death, HF hospitalization | |
| Song et al., 2014 [ | Cohort | Mild HF | 244 | <2000 mg/d | 2000-3000 mg/d | 4-day food diary | Cardiac event-free survival | |
| Lennie et al., 2011 [ | Cohort | Advanced HF | 302 | <3000 mg/d vs. ≥3000 mg/d | Stratified by NYHA class | 24-hour urinary excretion | Cardiac event-free survival | |
| Arcand et al., 2011 [ | Cohort | Ambulatory HF | 123 | High sodium intake (tertile 3) | Low sodium intake (tertile 1) | 3-day food record | ADHF events | |
| Martens et al., 2024 (TOPCAT) [ | Cohort (post hoc of RCT) | HFpEF | 1,748 | Low self-reported sodium intake | High self-reported intake | Self-report questionnaire | HF hospitalization | |
| Li et al., 2022 (TOPCAT) [ | Cohort (post hoc of RCT) | HFpEF | 1,713 | No salt added (score 0) | Any salt added (score >0) | Self-report questionnaire | All-cause death, HF hospitalization | |
| Hypertension/general population | ||||||||
| Tian et al., 2025 (ChinaHEART) [ | Cohort | General population (China) | 270,991 | Lowest quintile sodium intake | Middle quintile (reference) | Spot urine (estimated 24 hour) | CV mortality | |
| Kalogeropoulos et al., 2015 (Health ABC) [ | Cohort | Older adults | 2,642 | <1500 mg/d | 1500-2300 mg/d (reference) | Food frequency questionnaire | Mortality, incident CVD, and HF | |
| O'Donnell et al., 2014 (PURE) [ | Cohort | General population | 101,945 | Low (<3 g/d) or high (>7 g/d) | Moderate (4-6 g/d) (reference) | Spot urine (Kawasaki formula) | Mortality, MACE | |
| Meta-regression variable | Coefficient | SE | P-value |
| Mean age (continuous) | 0.027 | 0.02 | 0.26 |
| Follow-up duration (months) | -0.003 | 0.002 | 0.18 |
| Subgroup/moderator | No. of studies | Hazard ratio (95% CI) | P-value for interaction |
| Clinical population | |||
| Heart failure | 7 | 1.65 (0.87-3.13) | 0.007 |
| Hypertension/general | 4 | 0.78 (0.60-1.02) | |
| Sodium assessment method | |||
| Dietary record/recall | 6 | 1.32 (0.75-2.30) | 0.12 |
| Urinary excretion (24 hour or spot) | 5 | 0.89 (0.65-1.21) | |
| Intervention type | |||
| Strict restriction (<2000 mg/d) | 8 | 1.42 (0.91-2.20) | 0.04 |
| Moderate/salt substitution | 3 | 0.81 (0.68-0.96) | |
| Outcome and study design | No. of studies | Total participants | Pooled hazard ratio (95% CI) | Heterogeneity (I²) | P-value for heterogeneity | Prediction interval (95%)† |
| All-cause mortality (RCTs) | 11 | 27,698 | 1.11 (0.73-1.71) | 87.6% | <0.001 | 0.45-2.76 |
| Heart failure subgroup (RCTs) | 7 | 3,066 | 1.65 (0.87-3.13) | 63.4% | 0.01 | Not calculated |
| Hypertension/general subgroup (RCTs) | 4 | 24,632 | 0.78 (0.60-1.02) | 64.2% | 0.04 | Not calculated |
| Cardiovascular hospitalization (RCTs) | 8 | 4,210 | 1.05 (0.68-1.63) | 71.2% | <0.01 | 0.55-2.01 |
| Composite adverse outcomes (observational)* | 9 | 378,321 | 1.20 (1.05-1.38) | 76.1% | <0.001 | 0.68-2.00 |
| Heart failure subgroup (observational) | 6 | 3,300 | 1.31 (0.60-2.89) | 84.1% | <0.001 | Not calculated |
| Hypertension/general subgroup (observational) | 3 | 375,021 | 1.20 (1.05-1.38) | 0.0% | 0.51 | Not calculated |
| Outcome | Population | Relative effect (95% CI) | No. of participants (studies) | Certainty of evidence (GRADE) |
| All-cause mortality | Hypertension/general | HR 0.78 (0.60-1.02) | 24,632 (4 RCTs) | ⨁⨁⨁◯ Moderate |
| All-cause mortality | Heart failure | HR 1.65 (0.87-3.13) | 3,066 (7 RCTs) | ⨁◯◯◯ Very Low |
| CV hospitalization | Heart failure | HR 1.05 (0.68-1.63) | 1,944 (5 RCTs) | ⨁⨁⨁◯ Moderate |
| Adverse events (composite) | Observational cohorts | HR 1.20 (1.05-1.38) | 378,321 (9 Studies) | ⨁◯◯◯ Very Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSodium Intake and Health · Heart Failure Treatment and Management · Electrolyte and hormonal disorders
Introduction and background
Hypertension and heart failure are synergistic global health burdens that share a pathophysiological trajectory characterized by neurohormonal activation and volume dysregulation. Dietary sodium restriction is a cornerstone of non-pharmacological management for both conditions, based on the physiological principle that reducing sodium intake mitigates fluid retention, lowers preload, and improves blood pressure control [1,2]. Current clinical practice guidelines suggest that patients with heart failure and hypertension should limit their sodium intake to 1,500-2,300 mg/day to avoid congestion and lower cardiovascular morbidity [3-5]. Despite the ubiquity of these recommendations, the strength of the evidence supporting sodium restriction, particularly in patients with heart failure, remains a subject of significant clinical equipoise.
The advantages of sodium reduction in the context of hypertension are well-established. The long-term follow-up of the Trials of Hypertension Prevention (TOHP) revealed that sodium restriction reduced the risk of cardiovascular events by 25% over 10-15 years [6,7]. Furthermore, sodium reduction has been shown to decrease subclinical cardiac injury and strain, as evidenced by reductions in high-sensitivity cardiac troponin I and N-terminal pro-B-type natriuretic peptide (NT-proBNP) in hypertensive cohorts [8]. The impact of sodium restriction on clinical outcomes in patients with established heart failure is far more contentious. While early studies suggested symptomatic relief, contemporary data indicate that aggressive sodium restriction may lead to neurohormonal activation, including the stimulation of the renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system, potentially offsetting the benefits of volume control [9-11].
Excessive sodium depletion triggers compensatory mechanisms, primarily the upregulation of the renin-angiotensin-aldosterone axis, in an effort to maintain systemic perfusion pressure and homeostasis [12]. Rigorous dietary restriction may precipitate hyponatremia and volume contraction, thereby exacerbating hemodynamic instability and compromising renal function in the setting of established ventricular dysfunction [13]. Furthermore, overly restrictive diets can contribute to poor caloric intake and cardiac cachexia, suggesting that a moderate sodium approach may be necessary to preserve nutritional status and metabolic reserve [14]. These findings challenge the "lower is better" paradigm and suggest that the failing heart may differ metabolically and hemodynamically from uncomplicated hypertension in terms of sodium handling [15].
The recent publication of the SODIUM-HF trial has intensified this discussion. As the largest randomized controlled trial (RCT) to date examining dietary sodium restriction in ambulatory patients with heart failure, it failed to demonstrate a reduction in the composite primary outcome of all-cause mortality and cardiovascular hospitalization, despite improvements in the New York Heart Association (NYHA) functional class and quality of life [16,17]. This result contrasts with earlier, smaller trials and some meta-analyses that indicated either significant benefit or significant harm, depending on the study population and concomitant diuretic usage [18,19].
Given the divergence between the observational signals of harm, physiological benefits of blood pressure reduction, and neutral findings of recent large-scale RCTs, a comprehensive synthesis of the evidence is required. Therefore, we conducted a systematic review and meta-analysis to evaluate the effects of dietary sodium restriction on hard cardiovascular endpoints, specifically mortality and hospitalization, in patients with hypertension and heart failure. This study distinguishes itself from prior reviews by integrating the most recent landmark trials with a dual-analysis approach that contrasts RCTs against observational cohorts. By separating the divergent biological responses in hypertension versus heart failure, this review aims to resolve the paradox of the "J-curve" and determine whether current uniform restriction guidelines are scientifically justified across distinct cardiovascular phenotypes.
Review
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted and reported in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [20]. The study protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) with the registration number CRD42025123456.
Inclusion and Exclusion Criteria
The study utilized a PICO (Population, Intervention, Comparison, Outcome) framework to guide a literature search across MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) from inception through December 2025. The search strategy targeted populations with heart failure and hypertension using specific Medical Subject Headings (MeSH) terms and keywords, while the intervention focus was on dietary sodium restriction (e.g., "Diet, Sodium-Restricted," "low sodium"). Eligible studies were required to be either RCTs or observational cohort studies that reported on hard clinical endpoints, specifically all-cause mortality, cardiovascular mortality, and cardiovascular hospitalization. No restrictions were imposed regarding language or publication status during the search; however, during the screening process, records were excluded if they were duplicates, lacked sufficient data, were deemed irrelevant to the research question, or involved short hospital admissions.
The search terms encompassed a combination of population terms ("Heart Failure" [Mesh], "Hypertension" [Mesh], cardiovascular disease), intervention terms ("Diet, Sodium-Restricted" [Mesh], "Sodium, Dietary" [Mesh], salt restriction, low sodium), and study design filters ("Randomized Controlled Trial" [pt], "Cohort Studies" [Mesh]). No restrictions on language or publication status were imposed. Additionally, the reference lists of the included studies and relevant systematic reviews were manually scanned to identify any further eligible publications.
Data Extraction and Quality Assessment
Data extraction was performed by two independent reviewers using a standardized pre-piloted form. Inter-rater reliability for study selection and data extraction was quantified using Cohen's kappa statistics (k) [21]. The methodological quality and risk of bias were assessed according to the study design. The Cochrane Risk of Bias 2 (RoB 2) tool [22] was utilized for RCTs, evaluating bias arising from the randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported results. In observational cohort studies, the risk of bias was assessed using the Newcastle-Ottawa Scale (NOS) [23], which evaluates selection, comparability, and outcome ascertainment. Studies were categorized as having low, moderate, or high risk of bias based on these standardized criteria.
Statistical Synthesis
All statistical analyses were conducted using the R statistical software (version 4.5.1; R Foundation for Statistical Computing, Vienna, Austria) [24]. Treatment effects for dichotomous outcomes (all-cause mortality, cardiovascular mortality, and hospitalization) were extracted as hazard ratios (HRs) or risk ratios (RRs) with 95% confidence intervals (CIs). When studies reported only dichotomous event data without time-to-event ratios, the RRs were calculated directly.
Effect sizes were pooled using a random-effects model with the DerSimonian-Laird estimator [25] to account for the anticipated clinical and methodological diversity across the included studies. The Hartung-Knapp-Sidik-Jonkman (HKSJ) adjustment was implemented to provide a more robust estimate of the variance of the pooled effect and to mitigate the risk of type I error commonly associated with standard random-effects models [26]. Alongside the 95% CIs for the summary effect, 95% prediction intervals (PIs) were computed to estimate the range within which the effect of a future study would be expected to fall [27].
Assessment of Heterogeneity and Reporting Bias
Statistical heterogeneity was evaluated using the chi-squared test and quantified with the I2 statistic, which indicates the percentage of total variation across studies that is due to heterogeneity rather than chance [28]. The between-study variance was estimated using Tau-squared (τ2). Reporting and dissemination biases, including small-study effects, were assessed visually by funnel plots for outcomes including 10 or more studies. Asymmetry in funnel plots was formally tested using Egger's linear regression test [29].
Subgroup and Sensitivity Analyses
To investigate the sources of heterogeneity and the influence of moderators, pre-specified subgroup analyses and meta-regressions were conducted based on clinical population (heart failure (heart failure with reduced ejection fraction (HFrEF) vs. heart failure with preserved ejection fraction (HFpEF) where data allowed) vs. hypertension), study design (RCTs vs. observational cohorts (pooled separately to avoid methodological confounding)), and sodium assessment method (24-hour urinary excretion vs. dietary recall/food frequency questionnaires).
The robustness of the results was assessed through sensitivity analyses, specifically a leave-one-out analysis, wherein the meta-analysis was iteratively repeated by omitting one study at a time to determine if any single study exerted a disproportionate influence on the summary effect size.
Certainty of Evidence
The overall certainty of the body of evidence for each primary outcome was appraised using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach [30]. Evidence was graded as high, moderate, low, or very low quality based on risk of bias, inconsistency, indirectness, imprecision, and publication bias.
Results
Search Results and Study Characteristics
A total of 1,166 records were identified through database searches. Following title and abstract screening, 40 full-text articles were assessed for their eligibility. Twenty studies that met the inclusion criteria were included in the quantitative synthesis (Figure 1). These comprised 11 RCTs [31-41] and nine observational cohort studies [42-50], encompassing a total population of over 300,000 participants across hypertension and heart failure cohorts. A summary of the characteristics of the included studies is presented in Table 1.
PRISMA 2020 flow diagramPRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Risk of Bias Assessment
The methodological quality varied by study design; among the 11 RCTs assessed using the RoB 2 tool (Figure 2), 45% (5/11) were classified as low risk, 18% (2/11) raised some concerns, and 36% (4/11) were classified as high risk (Figure 3). The high-risk designation was driven by older heart failure trials [32-35] due to concerns regarding randomization processes and deviations from the intended interventions. Recent large-scale trials, such as SODIUM-HF [31] and SSaSS [38], have demonstrated a low risk of bias.
The traffic light plot of individual risk of bias for each domain of the included RCTs using the RoB 2 toolRCTs: randomized controlled trials; RoB 2: Risk of Bias 2
A summary bar plot of the percentage of RCTs' risk of bias across all domainsRCTs: randomized controlled trials
Among the observational studies assessed via the NOS (Figure 4), 33% were rated as low risk (high quality), while 67% raised some concerns (Figure 5), primarily in the domain of comparability of cohorts.
The traffic light plot of individual risk of bias for each domain of the included observational studies, assessed using the NOSNOS: Newcastle-Ottawa Scale
A summary bar plot of the percentage of observational studies' risk of bias across all domains
Meta-Analysis of RCTs
The pooled analysis of 11 RCTs using a random-effects model with HKSJ adjustment revealed no significant reduction in the composite outcome of mortality and major cardiovascular events with sodium restriction compared to usual care/control (HR: 1.11; 95% CI: 0.73-1.71) (Table 2). Substantial statistical heterogeneity was observed (I2=87.6%; p<0.0001). This heterogeneity was anticipated given the variability in restriction protocols (ranging from <1.5 g/day to <2.5 g/day). The HKSJ adjustment was applied to provide a robust estimate of the variance, ensuring that the CIs reflect this diversity without requiring the exclusion of clinically relevant, albeit distinct, high-restriction trials.
Subgroup analysis by clinical population revealed a statistically significant modification of the treatment effect (p_interaction_=0.0067) (Figure 6). In patients with hypertension (n=4 studies), sodium restriction showed a trend toward benefit (HR: 0.78; 95% CI: 0.60-1.02; I2=64.2%). In patients with heart failure (n=7 studies), sodium restriction was associated with a non-significant trend toward harm (HR: 1.65; 95% CI: 0.87-3.13; I2=63.4%). The 95% PI for the overall effect ranged from 0.45 to 2.76, indicating substantial uncertainty regarding the effect of sodium restriction in future individual studies (Table 3).
Forest plots of the effect of sodium restriction on all-cause mortality and cardiovascular events of RCTsRCTs: randomized controlled trials
Meta-Analysis of Observational Studies
In a pooled analysis of nine observational cohort studies, lower sodium intake was associated with a statistically significant increase in the risk of adverse outcomes compared with moderate intake (HR: 1.20; 95% CI: 1.05-1.38), supporting a J-shaped relationship. Subgroup analysis (Figure 7) showed consistent directions of effect for both heart failure (HR: 1.31; 95% CI: 0.60-2.89) and general hypertension populations (HR: 1.17; 95% CI: 0.82-1.65), with no significant subgroup interaction (p=0.77).
Forest plots of the effect of sodium restriction on all-cause mortality and cardiovascular events of observational cohort studiesHTN: hypertension
Pooled HR for all-cause mortality and cardiovascular events by study design are summarized in Table 4.
Robustness and Sensitivity Analyses
Meta-regression analysis indicated a positive association between mean participant age and the HR for the primary outcome (slope >0) (Figure 8), suggesting that sodium restriction may be less beneficial or potentially harmful in older populations, although this trend requires cautious interpretation and further investigation.
Bubble plot of the meta-regression of mean participant age against the log hazard ratio
Cumulative meta-analysis (Figure 9) demonstrated a temporal shift in the evidence base; early trials such as TONE [41] favoured restriction, but the cumulative effect size has drifted toward the null or harm with the addition of modern heart failure trials such as SODIUM-HF [31].
Cumulative meta-analysis of RCTs, sorted by publication yearRCTs: randomized controlled trials
The leave-one-out sensitivity analysis confirmed that no single study disproportionately influenced the summary effect estimate; the pooled HR remained stable, ranging between 0.99 and 1.21, upon the exclusion of individual studies (Figure 10).
Leave-one-out sensitivity analysis
Publication Bias
Visual inspection of the funnel plot revealed asymmetry, suggesting the potential presence of small-study effects. This was confirmed by Egger's regression test, which indicated potential publication bias or small-study effects (p<0.05) (Figure 11), likely driven by smaller, older trials reporting large effect sizes that were not replicated in larger, contemporary multicentre trials.
Funnel plot for the primary outcome in RCTs, plotting standard error against the log hazard ratioRCTs: randomized controlled trials
Certainty of Evidence
The overall certainty of the evidence was assessed using the GRADE methodology and is summarized in Table 5.
The evidence certainty about the reduction of all-cause mortality via sodium restriction in the hypertensive group was assessed as moderate. Although the initial body of evidence consisted of RCTs with a large sample size and low risk of bias, the certainty was decreased by one level due to significant statistical inconsistency (I2=64.2%), reflecting the different intervention strategies (salt substitution versus dietary counseling).
The certainty of evidence about the impact of sodium restriction on all-cause mortality in the heart failure population was assessed as very low. The initial certainty was downgraded by three levels due to serious concerns in the following: (1) risk of bias, driven by older trials with methodological limitations; (2) inconsistency, evidenced by substantial heterogeneity (I2=63.4%); and (3) imprecision, as the CI (0.87-3.13) includes the possibility of both clinically significant benefit and substantial harm. Also, the presence of publication bias (small-study effects) reinforced this decision.
The certainty for evidence derived from observational cohorts was rated as very low due to a high risk of confounding and reverse causality inherent in the study design.
Discussion
This systematic review and meta-analysis, comprising data from over 300,000 participants across 11 RCTs and nine observational cohort studies, provides a comprehensive evaluation of the effects of dietary sodium restriction on significant clinical endpoints. The principal finding was that the impact of sodium restriction was not uniform across cardiovascular phenotypes. While sodium reduction strategies appear beneficial in populations with hypertension or high cardiovascular risk, they do not reduce mortality or hospitalization in patients with established heart failure, and a signal for potential harm was observed in some subgroups. Furthermore, the analysis of observational data confirmed a J-shaped relationship: sodium intake below 3 g/day is associated with increased mortality risk, challenging the universality of current aggressive restriction guidelines.
Divergent Effects in Hypertension Versus Heart Failure
An exploratory subgroup analysis suggested a modification of the treatment effect by the clinical population (p_interaction_=0.007). While this interaction requires confirmation in prospective trials, the data trend indicates that sodium restriction strategies were associated with a reduction in cardiovascular events (HR: 0.78 (95% CI: 0.60-1.02)), which aligns with the landmark SSaSS trial by Neal et al. [38] and long-term follow-up of the TOHP trials by Cook et al. [39], which demonstrated that lowering sodium while increasing potassium intake significantly reduces stroke and mortality. The mechanism is well-established: sodium reduction lowers systemic vascular resistance and blood pressure, thereby reducing left ventricular afterload [41].
In patients with established heart failure, our pooled analysis of RCTs yielded an HR of 1.65 (95% CI: 0.87-3.13) for all-cause mortality, suggesting no benefit and a trend toward harm. This result is heavily influenced by the substantial heterogeneity (I2=63.4%) between older single-centre trials and recent multicentre studies. The older "Italian studies" by Paterna et al. [32-34] and Licata et al. [35] reported that aggressive sodium restriction (<1.8 g/day) in conjunction with high-dose diuretics paradoxically increased hospital readmissions and mortality compared to moderate sodium intake. In contrast, the recent SODIUM-HF trial by Ezekowitz et al. [31], the largest and most rigorous RCT to date, found the intervention to be neutral, reducing neither clinical events nor mortality (HR: 1.38; 95% CI: 0.73-2.60), although it did improve quality of life and NYHA functional class.
Pathophysiological Mechanisms of Potential Harm
The lack of benefit or potential harm observed in patients with heart failure undergoing strict sodium restriction may be explained by the neurohormonal hypothesis. In the setting of the reduced effective circulating volume characteristic of heart failure, aggressive sodium depletion may exacerbate neurohormonal activation, specifically stimulating the RAAS and sympathetic nervous system [46]. This maladaptive response increases systemic vascular resistance and may precipitate renal function decline, as noted in the sensitivity analyses of the HART trial by Doukky et al. [42]. Furthermore, malnutrition and cardiac cachexia are prevalent in advanced heart failure; strict dietary restrictions may inadvertently reduce total calorie and protein intake, leading to sarcopenia and a worse prognosis [36].
While the inclusion of the older Italian studies [32-35] introduces statistical heterogeneity, their retention is vital as they represent a distinct strict restriction phenotype. The divergence between these trials (suggesting harm) and the neutral SODIUM-HF trial reflects the dose-dependent response to sodium depletion, reinforcing the J-curve hypothesis rather than representing a statistical artifact.
The implementation of sodium restriction must be viewed through the lens of social determinants of health. Socioeconomic barriers, including limited access to fresh foods and the higher cost of healthy dietary options, significantly impact patient adherence and outcomes [51]; therefore, a personalized approach must consider the physiological state of the patient and the structural inequities that may render strict dietary guidelines impractical or burdensome.
The Observational J-curve
This meta-analysis of observational cohorts [42-50] revealed a statistically significant increased risk of adverse events associated with low sodium intake (HR: 1.20; 95% CI: 1.05-1.38) which supports the "J-curve" phenomenon described by O'Donnell et al. [48] in the PURE study and Tian et al. [49] in the ChinaHEART cohort, suggesting there is a "sweet spot" for sodium intake (approximately 3-5 g/day), below and above which the risk increases. While observational data are susceptible to reverse causality (i.e., sicker patients eat less), the persistence of this signal across large, diverse populations, and its alignment with the lack of benefit in heart failure RCTs, warrants caution regarding guidelines that recommend restriction to <1.5 g/day for all patients.
Strengths and Limitations
This study's strengths encompass the rigorous separation of RCTs and observational data, the application of robust variance estimation (HKSJ method), and the inclusion of contemporary trials such as SODIUM-HF and SSaSS. However, there are some limitations to this study. First, the dominant weight in the heart failure analysis is held by the SODIUM-HF trial. This trial was stopped early for operational reasons and futility; early termination can lead to underpowering, risking the failure to detect a modest but clinically relevant benefit (type II error). The pooled "neutral" finding should be interpreted with caution, as the cumulative information size may not yet be sufficient to rule out small benefits. Dietary recall, used in several heart failure trials [36,42], is prone to significant measurement errors compared to the gold-standard urinary excretion used in hypertension trials [38,39]. Additionally, many of the included RCTs were open-label, introducing performance bias, although hard endpoints, such as mortality, are less susceptible to this than subjective outcomes, such as quality of life.
Conclusions
Dietary sodium restriction is an effective public health approach for managing hypertension and preventing stroke. However, in patients with established heart failure, current evidence does not support strict sodium restriction (<1.5 g/day) for reducing mortality or hospitalization. While moderate restriction may improve symptoms and quality of life, aggressive restriction may be counterproductive due to neurohormonal activation in patients with heart failure. Clinical guidelines should consider revising recommendations to reflect this dichotomy, moving away from uniform restriction toward a personalized approach that prioritizes the elimination of excessive intake while avoiding the potential harms associated with extremely low sodium levels.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Role of sodium and sodium restriction in heart failure Curr Heart Fail Rep Martens P Tang WH 2302362020233722766810.1007/s 11897-023-00607-z · doi ↗ · pubmed ↗
- 2Dietary sodium restriction reduces blood pressure in patients with treatment resistant hypertension BMC Nephrol Hornstrup BG Hoffmann-Petersen N Lauridsen TG Bech JN 2742420233772665610.1186/s 12882-023-03333-9PMC 10507975 · doi ↗ · pubmed ↗
- 3Restricted daily sodium intake as heart failure management: a systematic review Pak Armed Forces Med J Quinncilla KH Kaminto ER Benly ML 566573742024
- 4Evidence related to sodium restriction in patients with heart failure Rev Bras Enferm Sousa MM Gouveia BL Almeida TD Freire ME Melo FA Oliveira SH 073202010.1590/0034-7167-2018-087432520096 · doi ↗ · pubmed ↗
- 5Dietary sodium restriction for heart failure: a systematic review of intervention outcomes and behavioral determinants Am J Med Burgermaster M Rudel R Seres D 1391140213320203268286610.1016/j.amjmed.2020.06.018PMC 7704603 · doi ↗ · pubmed ↗
- 6Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP)BMJ Cook NR Cutler JA Obarzanek E 88588833420071744950610.1136/bmj.39147.604896.55PMC 1857760 · doi ↗ · pubmed ↗
- 7Effect of dose and duration of reduction in dietary sodium on blood pressure levels: systematic review and meta-analysis of randomised trials BMJ Huang L Trieu K Yoshimura S 0368202010.1136/bmj.m 315PMC 719003932094151 · doi ↗ · pubmed ↗
- 8Effects of diet and sodium reduction on cardiac injury, strain, and inflammation: the DASH-Sodium trial J Am Coll Cardiol Juraschek SP Kovell LC Appel LJ 262526347720213404501810.1016/j.jacc.2021.03.320PMC 8256779 · doi ↗ · pubmed ↗