Clinical Characteristics of Patients With Patent Foramen Ovale and Pyogenic Brain Abscess
Khalid Abu-Zeinah, Pansachee Damronglerd, Hussam Tabaja, Zachary A Yetmar, Mark J Enzler, Guy S Reeder, Daniel C DeSimone, Larry M Baddour, Omar M Abu Saleh, Cristina Corsini Campioli, Supavit Chesdachai

TL;DR
This study found that adults with pyogenic brain abscess and a patent foramen ovale had different abscess features but similar mortality rates.
Contribution
The study reports a high prevalence of PFO in PBA patients and identifies distinct abscess characteristics associated with PFO.
Findings
PFO prevalence in PBA patients was 40.5%, higher than the general population.
PFO was associated with distinct abscess characteristics but not with increased mortality.
No significant difference in 1-year mortality was observed between PFO and non-PFO PBA patients.
Abstract
Patent foramen ovale (PFO) has a prevalence of approximately 25%. Its association with pyogenic brain abscess (PBA) is unclear. We reviewed adults with PBA and known PFO status from 1 January 2009 through 31 December 2021 at Mayo Clinic. High PFO prevalence (40.5%) was seen. PBA patients with PFO had distinct abscess characteristics but unchanged 1-year, all-cause mortality. Graphical AbstractCreated in BioRender [1]. Created in BioRender [1].
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
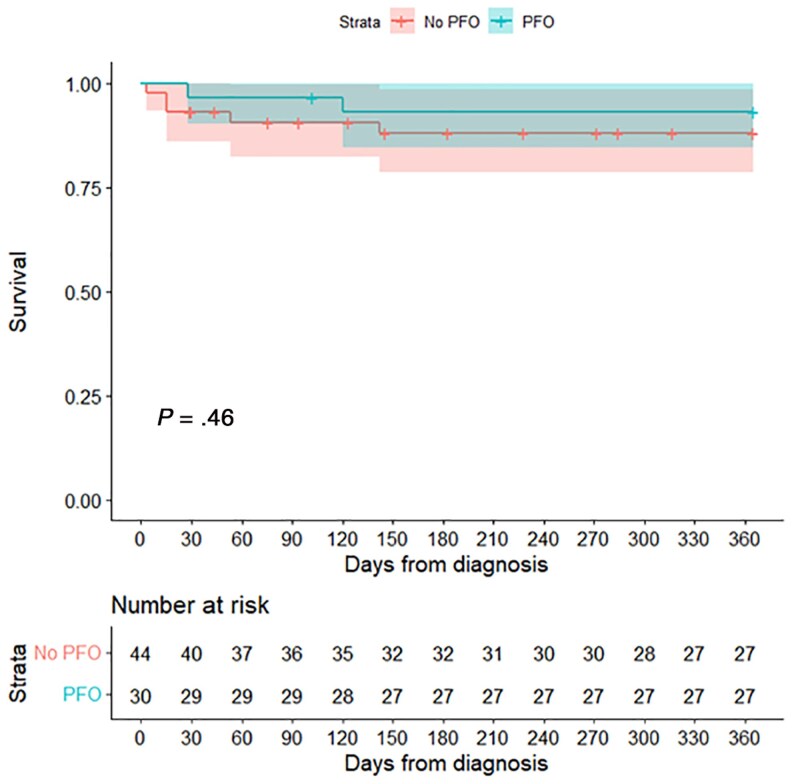 Figure 1
Figure 1| Characteristic | Total (N = 74) | No PFO (n = 44) | PFO (n = 30) |
|
|---|---|---|---|---|
| Age, y | 55.5 (43.2–66.5) | 51.5 (42.5–63.5) | 59.0 (46.0–67.8) | .288 |
| Female sex | 25 (33.8) | 14 (31.8) | 11 (36.7) | .665 |
| White race | 70 (94.6) | 41 (93.2) | 29 (96.7) | .515 |
| Comorbidities | ||||
| Diabetes mellitus | 18 (24.3) | 13 (29.5) | 5 (16.7) | .205 |
| Chronic kidney disease | 13 (17.6) | 10 (22.7) | 3 (10.0) | .158 |
| Heart failure | 19 (25.7) | 14 (31.8) | 5 (16.7) | .143 |
| Active malignancy | 7 (9.5) | 3 (6.8) | 4 (13.3) | .347 |
| Prior stroke | 8 (10.8) | 3 (6.8) | 5 (16.7) | .180 |
| Immunosuppressive therapy | 4 (5.4) | 2 (4.5) | 2 (6.7) | .692 |
| HSCT | 1 (1.4) | 1 (2.3) | 0 (0.0) | .406 |
| Hypertension | 21 (28.4) | 12 (27.3) | 9 (30.0) | .798 |
| Peripheral vascular diseases | 23 (31.1) | 15 (34.1) | 8 (26.7) | .498 |
| Dementia | 3 (4.1) | 2 (4.5) | 1 (3.3) | .795 |
| COPD | 11 (14.9) | 6 (13.6) | 5 (16.7) | .719 |
| Connective tissue disease | 4 (5.4) | 1 (2.3) | 3 (10.0) | .149 |
| Charlson Comorbidity Index score | 4.0 (2.0–6.0) | 4.0 (2.0–6.0) | 4.0 (2.0–7.8) | .748 |
| Positive blood culture at the time of diagnosis | 29 (39.2) | 22 (50.0) | 7 (23.3) | . |
| Organisms in blood culture | ||||
|
| 14 (18.9) | 11 (25.0) | 3 (10.0) | .106 |
| CoNS | 1 (1.4) | 1 (2.3) | 0 (0.0) | .406 |
| Viridans group | 12 (16.2) | 8 (18.2) | 4 (13.3) | .579 |
| Group C | 1 (1.4) | 1 (2.3) | 0 (0.0) | .406 |
| Gram-negative bacteria | 2 (2.7) | 2 (4.5) | 0 (0.0) | .236 |
| Multiple abscesses | 25 (33.8) | 19 (43.2) | 6 (20.0) | . |
| Largest abscess diameter, mm | 19.5 (11.2–30.0) | 15.5 (10.0–28.0) | 25.0 (15.8–37.5) | . |
| Location of abscess | ||||
| Frontal lobe | 38 (51.4) | 28 (63.6) | 10 (33.3) | . |
| Parietal lobe | 24 (32.4) | 12 (27.3) | 12 (40.0) | .251 |
| Temporal lobe | 13 (17.6) | 10 (22.7) | 3 (10.0) | .158 |
| Occipital lobe | 15 (20.3) | 11 (25.0) | 4 (13.3) | .220 |
| Thalamus | 4 (5.4) | 1 (2.3) | 3 (10.0) | .149 |
| Midbrain | 1 (1.4) | 0 (0.0) | 1 (3.3) | .223 |
| Cerebellum | 8 (10.8) | 6 (13.6) | 2 (6.7) | .343 |
| Brainstem | 3 (4.1) | 1 (2.3) | 2 (6.7) | .347 |
| Potential source of abscess | ||||
| Cryptogenic | 24 (32.4) | 8 (18.2) | 16 (53.3) | . |
| Odontogenic | 18 (24.3) | 14 (31.8) | 4 (13.3) | .069 |
| Infective endocarditis | 16 (21.6) | 11 (25.0) | 5 (16.7) | .393 |
| Seeding from distant sources | 6 (8.1) | 5 (11.4) | 1 (3.3) | .214 |
| Sinusitis | 3 (4.1) | 3 (6.8) | 0 (0.0) | .144 |
| TBI including subdural and epidural spreading | 3 (4.1) | 3 (6.8) | 0 (0.0) | .144 |
| Postcranial surgery | 2 (2.7) | 0 (0.0) | 2 (6.7) | .083 |
| Otitis or mastoiditis | 1 (1.4) | 0 (0.0) | 1 (3.3) | .223 |
| Thrombophlebitis of neck vein | 1 (1.4) | 0 (0.0) | 1 (3.3) | .223 |
| Positive culture from abscess | 50 (67.6) | 27 (61.4) | 23 (76.7) | |
| Monomicrobial | 35 (70.0) | 18 (66.7) | 17 (73.9) | .167 |
| Polymicrobial | 15 (30.0) | 9 (33.3) | 6 (26.1) | .577 |
| Organisms in abscess culture | ||||
|
| 5 (6.8) | 3 (6.8) | 2 (6.7) | .980 |
| CoNS | 2 (2.7) | 1 (2.3) | 1 (3.3) | .782 |
| Viridans group | 37 (50.0) | 21 (47.7) | 16 (53.3) | .636 |
|
| 2 (2.7) | 1 (2.3) | 1 (3.3) | .782 |
|
| 4 (5.4) | 3 (6.8) | 1 (3.3) | .515 |
| Gram-negative bacteria | 5 (6.8) | 3 (6.8) | 2 (6.7) | .980 |
| Anaerobes | 15 (20.3) | 8 (18.2) | 7 (23.3) | .588 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiovascular and Diving-Related Complications · Infective Endocarditis Diagnosis and Management · Cerebrospinal fluid and hydrocephalus
Patent foramen ovale (PFO) is the most prevalent congenital cardiac anomaly persisting after birth [2]. Reported prevalence varies by population and diagnostic method, from 14% using transthoracic echocardiography (TTE) with agitated saline (“bubble study”), to 23.7% using transesophageal echocardiography (TEE), and 31.3% with transcranial doppler [3, 4]. Autopsy studies report similar prevalence of 27.3% [5].
PFO is the most common cause of right-to-left shunting in the general population [6], but its clinical relevance is debated. PFO is associated with cryptogenic stroke [7], likely from paradoxical embolization during transient right-to-left shunting. Additionally, limited evidence in the form of case series suggests an association between PFO and pyogenic brain abscesses (PBAs), although this relationship remains poorly understood [8–10]. PBAs are focal, suppurative infections of brain parenchyma arising from contiguous spread or hematogenous dissemination, or classified as cryptogenic when no source is identified [11].
In a similar mechanism to causing cryptogenic stroke, PFO has been hypothesized to increase risk of PBA. Right-left-shunting may allow bacteria and septic emboli from the venous system to bypass the pulmonary circulation [12], which normally traps and clears circulating bacteria via resident phagocytes [13], and reach the brain. Indeed, right-to-left shunting in other conditions, such as pulmonary arteriovenous malformations and cyanotic congenital heart disease (CHD), is a known risk factor for PBA, with 25%–46% of patients with unrepaired cyanotic CHD developing brain abscesses [14–17].
This study aimed to assess the prevalence of PFO in patients with PBA at our institution and to compare clinical characteristics, management, and outcomes of PBA in patients with and without a PFO. Identifying associations between PFO and PBA may improve understanding of PBA risk factors, inform when targeted echocardiographic evaluation in PBA can be considered, and prompt clinicians to consider PBA as a differential diagnosis in patients with PFOs presenting with compatible neurologic symptoms.
METHODS
We retrospectively reviewed adult patients (≥18 years) diagnosed with PBA between 1 January 2009 and 31 December 2021, at all Mayo Clinic sites (Rochester, Scottsdale, and Jacksonville). Only patients who underwent TEE or TTE with agitated saline (bubble) study were included. TTE without bubble study was excluded due to lower sensitivity for PFO detection [7]. Minnesota residents declining Minnesota research authorization were excluded. Patients were identified using International Classification of Diseases, Ninth Revision and Tenth Revision codes (324, 098.89, 006.5, G06.0, A54.82, A06.6) for brain abscess. The detailed search procedure and definitions were described in a previous study [18]. Nocardia and fungal brain abscesses were excluded, due to distinct epidemiology, host factors, and course compared with typical PBA [11]. Data abstracted from electronic medical records was stored in REDCap [19, 20].
The study was granted exempt status by Mayo Clinic Institutional Review Board (IRB 20-009299) and conducted per Helsinki Declaration guidelines. Informed consent from patients was waived as we used de-identified, retrospective data.
Descriptive statistics were used and reported as median (interquartile range [IQR]) for continuous variables and count (percentage) for categorical variables. The χ^2^ test or Fisher exact test was used for categorical variables and Kruskal–Wallis rank-sum test for continuous variables. One-year survival was assessed using Kaplan–Meier analysis. Analyses were performed using R version 4.2.2 software (R Foundation for Statistical Computing, Vienna, Austria).
RESULTS
PFO Proportion
A total of 222 patients developed PBA during the study period. Of these, 74 patients (33.3%) had known PFO status and comprised the study cohort (Supplementary Figure 1). Compared to patients with unknown PFO status, those in the study cohort more frequently had bacteremia and cryptogenic or odontogenic sources of infection (Supplementary Table 1); however, there was no difference in 1-year all-cause mortality between the groups (Supplementary Figure 2).
PFO was detected in 30 of the 74 patients (40.5%). Among those with PFO, intracardiac shunting was demonstrated in 22 patients (73.3%): 12 (54.5%) with right-to-left, 6 (27.3%) with bidirectional, and 4 (18.2%) with left-to-right shunting.
Most patients (n = 52 [70.3%]) underwent echocardiography within 30 days of PBA diagnosis, prompted by the PBA diagnosis itself, suspected infective endocarditis (IE), or bacteremia. Eight (10.8%) patients underwent echocardiography prior to diagnosis, and 14 (18.9%) >30 days after diagnosis (for other indications like valvular assessment, suspected IE, and cryptogenic stroke workup).
Baseline and Clinical Characteristics
Table 1 demonstrates demographic and clinical characteristics of the study cohort. The median age was 55.5 years; 25 (33.8%) were female. Baseline demographics were similar between PFO and non-PFO groups.
Bacteremia at time of diagnosis was less common in the PFO group compared to the non-PFO group (23.3% vs 50.0%, P = .021). The presence of multiple abscesses was less common in the PFO group (20.0% vs 43.2%, P = .038). Median abscess diameter was larger in the PFO group (25.0 mm vs 15.5 mm, P = .038).
Frontal lobe abscesses were more common in the non-PFO group (63.6% vs 33.3%, P = .010). The most common PBA etiology was cryptogenic (n = 24 [32.4%]) followed by odontogenic (n = 18 [24.3%]) and IE (n = 16 [21.6%]). Cryptogenic abscesses were more frequent among PFO patients (53.3% vs 18.2%, P = .002).
Diagnostic procedures were performed in 54 (73.0%) patients: 30 (40.5%) underwent stereotactic aspiration and 24 (32.4%) underwent craniotomy with aspiration. Of those 54 patients, 50 (92.6%) had positive abscess cultures, most often monomicrobial. Viridans group streptococci were most commonly implicated (n = 37 [50%]). Among culture-positive cases, pathogen distribution did not differ between groups. Of the 20 patients who did not undergo diagnostic procedures, 19 (95%) had positive blood cultures. Among PFO patients, comparisons by shunt direction revealed no significant differences in most PBA characteristics, but patients with right-to-left shunting tended to have more frontal lobe abscesses (P = .007).
Management and Outcomes
Management strategies were similar between both groups. Thirty-four (45.9%) patients underwent neurosurgical therapy, including aspiration or surgical excision. The remainder were treated with medical therapy. No difference in 1-year all-cause mortality between PFO and non-PFO groups was noted (P = .46; Figure 1). Nine patients underwent PFO closure after indentification, typically prompted by a history of stroke or performed concurrently with repair of another structural cardiac abnormality.
Kaplan–Meier analysis demonstrating no difference in 1-year all-cause mortality between the patent foramen ovale (PFO) and non-PFO groups. Figure generated in R (v4.2.2) [21].
DISCUSSION
In our descriptive study of patients with PBA and known PFO status, 40.5% had PFO. This frequency is higher than prior reports in the general population of 14% using the less sensitive TTE with bubble study [3] and 23.7% using TEE [2, 3]. Although stroke prevalence was similar between the 2 groups, we observed a greater proportion of cryptogenic PBAs in patients with PFO.
PFO patients were more likely to have single, larger abscesses, a pattern consistent with the proposed mechanism of paradoxical embolization, whereby a septic embolus or bacterial inoculum travels through a cerebral arterial territory and leads to solitary abscess. Similarly, PFO-associated strokes have been more frequently described as single cortical infarcts [22]. In contrast, bacteremia, a known risk factor for multiple brain abscesses [23], was more common in the non-PFO group. Given the small absolute number of bacteremic cases and modest absolute differences, these descriptive associations should mostly be considered hypothesis-generating.
Although PFO status did not seem to influence the mortality outcomes or alter management strategies, its importance may instead lie in identifying patients at higher risk of PBA development. Our findings add to the limited literature regarding PBA in patients with PFO. A high frequency of PFO in our study cohort suggests that PFO may be an underrecognized risk factor for the development of PBA. Our study, however, is limited by its retrospective design, descriptive nature, the absence of a matched control group of patients without PBA, and lack of sensitivity analysis. Moreover, not all patients with PBA underwent PFO evaluation with echocardiography. PFO status was therefore not known for most cases, limiting the size of our study cohort, introducing selection bias, and limiting the interpretation of observed differences between the PFO and non-PFO groups. Additionally, our comparison of patients with and without PFO evaluation shows inherent differences between the 2 groups, including in microbiological data. In contrast to our prior institutional cohort in which Staphylococcus species predominated [18], Streptococcus species were the most frequent abscess isolates in our cohort with PFO evaluation, with minimal contribution from Staphylococcus species.
Larger multicenter prospective studies with standardized echocardiographic evaluation of all patients with PBA are needed to determine the true prevalence of PFO in PBA, define the clinical impact of echocardiographic imaging in this scenario, and clarify whether identifying PFO could influence management or outcomes of PBA. At present, no guidelines formally recommend PFO evaluation for all PBA cases. However, similar to the evaluation of cryptogenic stroke, echocardiography can be considered in patients with PBA if no clear source is identified, both to evaluate for PFO and for IE. It is unclear if establishment of an association between PFO and PBA will have definite implications to management. Limited case series have suggested PFO closure for prevention of recurrent brain abscesses [9]. However, current guidelines do not routinely recommend this for PBA, and larger studies are needed to evaluate the utility of PFO closure in prevention of PBA recurrence.
In summary, we observed a higher frequency of PFO in patients with PBA, along with distinct clinical patterns of presentation. Due to the limitations listed, further studies to evaluate the relationship between PFO and PBA are warranted.
Supplementary Material
ofag026_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abu-Zeinah K . 2026. Graphical Abstract. Created in Bio Render. https://Bio Render.com/ux 1xppw.
- 2Homma S, Messe SR, Rundek T, et al Patent foramen ovale. Nat Rev Dis Primers 2016; 2:15086.27188965 10.1038/nrdp.2015.86 · doi ↗ · pubmed ↗
- 3Koutroulou I, Tsivgoulis G, Tsalikakis D, Karacostas D, Grigoriadis N, Karapanayiotides T. Epidemiology of patent foramen ovale in general population and in stroke patients: a narrative review. Front Neurol 2020; 11:281.32411074 10.3389/fneur.2020.00281 PMC 7198765 · doi ↗ · pubmed ↗
- 4Liu F, Kong Q, Zhang X, et al Comparative analysis of the diagnostic value of several methods for the diagnosis of patent foramen ovale. Echocardiography 2021; 38:790–7.33870543 10.1111/echo.15058 · doi ↗ · pubmed ↗
- 5Hagen PT, Scholz DG, Edwards WD. Incidence and size of patent foramen ovale during the first 10 decades of life: an autopsy study of 965 normal hearts. Mayo Clin Proc 1984; 59:17–20.6694427 10.1016/s 0025-6196(12)60336-x · doi ↗ · pubmed ↗
- 6Tighe DA, Aurigemma GP. Right-to-left shunts and saline contrast echocardiography. Chest 2010; 138:246–8.20682525 10.1378/chest.10-0420 · doi ↗ · pubmed ↗
- 7Kent DM, Wang AY. Patent foramen ovale and stroke: a review. JAMA 2025; 334:1463.40720119 10.1001/jama.2025.10946 · doi ↗ · pubmed ↗
- 8Chen FC, Tseng YZ, Wu SP, Shen TY, Yang HP, Chen CC. Vegetation on patent foramen ovale presenting as a cryptogenic brain abscess. Int J Cardiol 2008; 124:e 49–50.17360058 10.1016/j.ijcard.2006.11.200 · doi ↗ · pubmed ↗