Active Surveillance of Iodinated Contrast Media-Induced Reactions and Associated Risk Factors Among Patients Undergoing Radiologic Procedures in Tertiary Hospitals in Tanzania: A Prospective Cohort Study
Riziki S Shemula, Manase Kilonzi, Elias Bukundi, Mathias E Mlugu, Ritah F Mutagonda

TL;DR
This study in Tanzania found that nearly 40% of patients had reactions to iodinated contrast media during radiologic procedures, with acute reactions being more common than delayed ones.
Contribution
The study provides new insights into the incidence and risk factors of ICM-induced reactions in a Tanzanian tertiary hospital setting.
Findings
Acute ICM-induced reactions occurred in 39.2% of patients, with gastrointestinal, neurological, and dermatological symptoms being most common.
Stage 2 renal failure was the strongest risk factor for ICM-induced reactions, with an adjusted risk ratio of 2.143.
Diabetes mellitus was associated with a lower risk of ICM-induced reactions (adjusted risk ratio = 0.540).
Abstract
Background: Exposure to iodinated contrast media (ICM), particularly at higher doses, carries significant risks of acute hypersensitivity and organ toxicity, especially involving the kidneys and cardiovascular system. Documenting these reactions is vital for patient safety, risk management, and medico-legal considerations. This study aimed to determine the incidence of ICM-induced adverse reactions and to identify associated risk factors among patients undergoing radiologic imaging in tertiary hospitals in Tanzania. Materials and methods: This prospective cohort study enrolled 283 patients undergoing contrast-based radiologic procedures between March and May 2024 at two tertiary hospitals in the Ilala district, Tanzania. Data on demographics, drug history, comorbidities, and prior contrast exposure were collected through structured questionnaires and patient files. Blood pressure and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
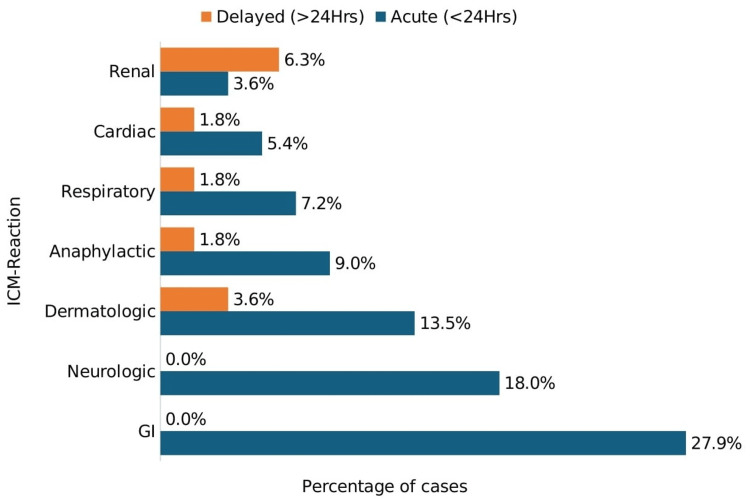 Figure 1
Figure 1| Variable | Frequency (n) | Percent (%) |
| Sex | ||
| Male | 137 | 48.4 |
| Female | 146 | 51.6 |
| Age (median = 56) | ||
| 18-40 | 83 | 29.3 |
| 41-65 | 135 | 47.7 |
| >65 | 65 | 23.0 |
| Residency | ||
| Inside Dar es Salaam | 157 | 53.4 |
| Outside Dar es Salaam | 126 | 46.6 |
| BMI (median = 26.84) | ||
| Underweight | 4 | 1.4 |
| Normal weight | 84 | 29.7 |
| Overweight | 132 | 46.6 |
| Obesity | 63 | 22.3 |
| Allergic to any medications | ||
| Yes | 16 | 5.7 |
| No | 267 | 94.3 |
| Indication for radiologic study | ||
| Cardiopulmonary | 45 | 15.9 |
| Gastrointestinal and abdominal | 47 | 26.5 |
| Oncological | 53 | 18.7 |
| Neurological | 25 | 8.8 |
| Vascular and procedural | 85 | 30.0 |
| Dose of contrast (ml) <100 | 246 | 86.9 |
| 100-200 | 36 | 12.7 |
| >200 | 1 | 0.4 |
| Medical history | ||
| Heart problem | 51 | 18.0 |
| Thyroid disorders | 2 | 0.7 |
| Previous use of contrast media | 20 | 7.1 |
| Cigarette smoking | 18 | 6.4 |
| High cholesterol | 3 | 1.1 |
| Diabetes mellitus | 17 | 6.0 |
| Asthma | 5 | 1.8 |
| Alcohol consumption | 38 | 13.4 |
| Anemia | 10 | 3.5 |
| Hypertension | ||
| Stage 1 | 21 | 7.4 |
| Stage 2 | 29 | 10.2 |
| Stage 3 | 19 | 6.7 |
| Renal failure | ||
| Stage 2 | 11 | 3.9 |
| Stage 3 | 15 | 5.3 |
| Previous medication use | ||
| Diuretics | 61 | 21.6 |
| Angiotensin 2 receptor blockers | 40 | 14.1 |
| Calcium channel blockers | 7 | 2.5 |
| Angiotensin-converting enzyme inhibitor | 2 | 2.5 |
| NSAIDs | 20 | 7.1 |
| Over-the-counter/other medications | 11 | 3.9 |
| Clopidogrel | 25 | 8.8 |
| Atorvastatin | 21 | 7.4 |
| Variable | Categories | n (%) | Univariate analysis CRR (95% CI) | P-value | Multivariate analysis ARR (95% CI) | p-value |
| Age (years) | 18-40 | 35 (48.6) | 3.21 (1.21-8.75) | 0.013 | 1.12 (0.71-1.77) | 0.613 |
| 41-65 | 54 (40.3) | 1.16 (0.90-1.49) | 0.161 | 1.16 (0.90-1.49) | 0.261 | |
| >65 | 22 (28.6) | Ref | Ref | |||
| BMI (kg/m²) | Underweight | 2 (50.0) | 1.21 (1.08-5.91) | 0.193 | 1.38 (0.74-2.59) | 0.310 |
| Normal weight | 43 (51.2) | 0.45 (0.05-2.20) | 0.040 | 1.45 (1.047-2.0) | 0.025 | |
| Overweight | 70 (53.0) | 3.15 (1.13-4.27) | 0.031 | 1.31 (0.99-1.73) | 0.043 | |
| Obese | 19 (20.2) | Ref | Ref | |||
| Indication for radiologic procedure | Cardiopulmonary | 20 (54.1) | 1.06 (0.70-2.37) | 0.104 | 1.36 (1.01-1.77) | 0.045 |
| Gastrointestinal | 30 (42.9) | 1.25 (1.03-1.76) | 0.159 | 1.25 (0.93-1.67) | 0.138 | |
| Oncological | 24 (53.3) | 1.20 (1.11-2.92) | 0.082 | 1.35 (1.02-1.80) | 0.039 | |
| Neurological | 13 (72.2) | 2.19 (0.92-5.10) | 0.013 | 1.50 (1.12-2.00) | 0.007 | |
| Vascular and procedural | 24 (21.2) | Ref | Ref | |||
| Contrast dose (ml) | <100 | 92 (37.4) | 0.77 (0.28-2.74) | 0.021 | 1.767 (0.98-3.54) | 0.120 |
| 100-200 | 16 (45.4) | 3.43 (1.30-6.63) | 0.015 | 2.36 (1.00-4.68) | 0.055 | |
| >200 | 0 (0.0) | Ref | Ref | |||
| Hypertension | No | 91 (49.2) | 0.14 (1.43-3.11) | 0.017 | 1.34 (0.84-2.15) | 0.217 |
| Stage 0 (elevated) | 5 (14.3) | 1.24 (0.88-1.91) | 0.151 | 0.97 (0.51-1.86) | 0.925 | |
| Stage 1 | 10 (28.6) | Ref | Ref | |||
| Renal failure (KDIGO stage) | Stage 1 | 102 (40.5) | 0.99 (0.72-2.11) | 0.041 | 1.59 (0.91-2.79) | 0.104 |
| Stage 2 | 5 (71.4) | 1.03 (1.01-2.50) | 0.109 | 2.14 (1.21-3.81) | 0.009 | |
| Stage 3 | Ref | Ref | ||||
| Anemia | Yes | 5 (100.0) | 1.1 (0.95-2.23) | 0.119 | 1.49 (1.14-1.95) | 0.003 |
| No | 96 (34.5) | Ref | Ref | |||
| Diabetes mellitus | Yes | 3 (10.0) | 3.15 (1.31-6.05) | 0.112 | 0.54 (0.31-0.95) | 0.033 |
| No | 109 (43.1) | Ref | Ref | |||
| Alcohol use | Yes | 12 (15.5) | 1.02 (0.89-1.55) | 0.178 | 1.02 (0.77-1.36) | 0.878 |
| No | 99 (41.9) | Ref | Ref | |||
| Heart conditions | Yes | 18 (24.0) | 2.12 (0.91-3.14) | 0.106 | 1.02 (0.68-1.53) | 0.907 |
| No | 93 (44.7) | Ref | Ref | |||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Kidney Injury Research · Ultrasound and Hyperthermia Applications · Central Venous Catheters and Hemodialysis
Introduction
Iodinated contrast media (ICM) are widely used in radiology to enhance visualization of internal structures [1]. They are primarily administered intravenously, although intra-arterial and intrathecal routes are also employed [2]. Despite their diagnostic utility, ICMs can cause a range of adverse reactions, from mild allergic responses to severe life-threatening events [3]. The safety profile of ICMs depends on properties such as ionicity, iodine concentration, osmolarity, and viscosity. Non-ionic agents are generally preferred because their lower osmolality reduces the likelihood of hypersensitivity reactions [4].
Adverse reactions to ICM are typically classified as acute or delayed. Acute reactions, including anaphylactoid responses and contrast-associated acute kidney injury (CA-AKI), are more common with high-osmolar contrast agents, particularly in patients with pre-existing renal dysfunction [5]. CA-AKI is a significant complication caused by renal vasoconstriction, oxidative stress, and direct tubular toxicity, potentially leading to reversible or irreversible kidney damage [6]. Cardiovascular complications may range from mild hypotension to severe arrhythmias [2,3]. Delayed reactions, often immunologically mediated, can occur hours to days after ICM administration and may involve dermatological or systemic manifestations [7].
From a medico-legal perspective, healthcare providers face growing obligations related to informed consent, documentation, and risk mitigation in the administration of contrast agents. Inadequate management of ICM reactions can result in liability, underscoring the necessity of adherence to clinical guidelines and the implementation of proactive safety measures [8,9].
In Tanzania, the use of contrast-enhanced diagnostics has increased rapidly; however, there is limited research on ICM-related complications beyond nephrotoxicity. [10,11]. This study aimed to determine the incidence of ICM-induced adverse reactions and to identify associated risk factors among patients undergoing radiologic imaging in tertiary hospitals in Tanzania.
Materials and methods
Study design and setting
A hospital-based, single-arm prospective cohort study was conducted from March to May 2024 at two tertiary care centers in Dar es Salaam: Muhimbili National Hospital (MNH) and Jakaya Kikwete Cardiac Institute (JKCI). These hospitals serve as national referral centers, receiving patients requiring advanced radiologic imaging for diagnostic and therapeutic purposes. Both institutions follow standardized radiology protocols and routinely use non-ionic low-osmolality ICM for contrast-enhanced imaging procedures.
Study participants and eligibility criteria
The study included consenting adult patients who underwent radiologic procedures involving iodinated contrast agents at either MNH or JKCI. Patients were eligible if they had no prior contraindications to ICM and could be followed up for adverse event monitoring. Patients who were unwilling/unable to provide consent or complete follow-up were excluded. Patients with documented prior severe contrast reactions were not routinely scheduled for contrast-enhanced imaging and were therefore not enrolled. Muhimbili University of Health and Allied Sciences Institutional Review Board issued approval MUHAS-REC-03-2024-2120
Sample size and sampling technique
A sample size of 283 patients was determined using Cochran’s formula, accounting for a 20% nonresponse rate, a 5% precision error, and a 1.96 confidence level [12]. The initial proportion of contrast media reactions was estimated at 19% in a study in Tanzania [11]. Participants were recruited using consecutive sampling. This approach minimized selection bias by enrolling all eligible patients in sequence as they presented for procedures.
Data collection process
Data were collected by three trained research assistants (registered nurses) and the principal investigator (a pharmacovigilance expert pharmacist). A pretested structured questionnaire covering key domains, including sociodemographic characteristics, medical history, medication use, comorbidities, prior ICM exposure, and history of medication allergy, was used. The questionnaire was informed by the literature review, expert consultation, and the investigator's experience. Pretesting was conducted among approximately 10% of the expected sample size to ensure clarity, internal consistency, and feasibility in the study setting.
Additional data, including laboratory findings (e.g., serum creatinine, hemoglobin) and clinically documented complications, were extracted from patient medical files. Participants were actively followed up at 0-60 minutes (acute phase), 24 hours, 72 hours, and 7 days post-procedure. Patients discharged before day 7 were followed up via phone. Physical assessments (height, weight, blood pressure) were conducted using standardized equipment and procedures.
BMI was categorized using WHO standards: underweight (<18.5 kg/m²), normal (18.5-24.9 kg/m²), overweight (25.0-29.9 kg/m²), and obese (≥30.0 kg/m²). All contrast-enhanced procedures utilized intravenously administered non-ionic low-osmolality ICM, with volumes typically ranging from <100 mL to 200 mL, depending on procedure type and clinical indication. Contrast agent selection was guided by institutional procurement policies and availability during the study period. Delayed adverse events among patients discharged before day 7 were assessed using a standardized phone-based checklist focusing on dermatological symptoms, renal symptoms, hospital re-attendance, and clinician-diagnosed adverse events.
Statistical analysis
Data were analyzed using SPSS Statistics version 27 (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp.). Renal function was classified using estimated glomerular filtration rate (mL/min/1.73 m²) according to KDIGO guidelines: stage 2 (60-89) and stage 3 (30-59). Descriptive statistics were summarized using frequencies and percentages.
A multi-stage analytical approach was used to identify factors associated with ICM-induced reactions. First, bivariate associations were assessed using chi-square tests. Variables with a p-value <0.20 in bivariate analysis were entered into univariate Poisson regression models. Variables meeting this threshold, together with clinically relevant covariates (e.g., age, BMI, renal function, comorbidities), were considered for inclusion in the multivariate Poisson regression model. Variables retained in the final model were selected based on statistical significance and clinical relevance, with p-values <0.05 considered significant. Adjusted risk ratios (ARRs) with 95% confidence intervals were reported to quantify independent associations.
Results
Sociodemographic and clinical characteristics
Out of the 283 participants, 146 (51.6%) were female, and 135 (47.7%) were aged between 41 and 65 years. Based on BMI, 132 (46.6%) participants were classified as overweight. Most participants, 267 (94.3%), reported no prior history of medication-related allergic reactions, while 16 (5.7%) had a documented history of medication allergy. The majority received a contrast dose of less than 100 mL (246, 86.9%). Regarding indications for imaging, vascular and interventional procedures were the most common (85, 30.0%), followed by gastrointestinal and abdominal imaging (75, 26.5%) (Table 1).
Incidence of ICM-induced reaction
Overall, 111 of 283 participants (39.2%) experienced ICM-induced reactions. Figure 1 shows the distribution of acute and delayed reactions. Among acute events, gastrointestinal complications were most frequent (27.9%), followed by neurological (18.0%) and dermatological reactions (13.5%). Delayed events were less common and primarily included CA-AKI (6.3%) and delayed cutaneous reactions (3.6%).
Distribution of acute and delayed ICM reactions among participants (N = 111)GI: gastrointestinal, ICM: iodinated contrast media
Factors associated with ICM-induced reactions among study participants
Following multivariate analysis, the factors associated with the incidence of ICM-induced reactions were normal weight BMI (ARR = 1.45, 95% CI: 1.047-2.00, p = 0.025), overweight BMI (ARR = 1.31, 95% CI: 0.99-1.73, p = 0.043), oncological indication (ARR = 1.35, 95% CI: 1.02-1.80, p = 0.039), neurological indication (ARR = 1.50, 95% CI: 1.12-2.00, p = 0.007), stage 2 renal failure (ARR = 2.14, 95% CI: 1.21-3.81, p = 0.009), and anemia (ARR = 1.49, 95% CI: 1.14-1.95, p = 0.003). Conversely, diabetes mellitus was found to be protective (ARR = 0.54, 95% CI: 0.30-0.97, p = 0.033) (Table 2).
Discussion
This study determined the incidence and risk factors of ICM-induced adverse reactions among patients undergoing diagnostic and interventional radiology in Tanzania. Overall, a high incidence of ICM-induced reactions was observed. The most common acute reactions were gastrointestinal, neurological, and dermatological complications, while delayed reactions primarily involved renal and dermatological complications. The occurrence of these reactions was statistically significantly associated with patient BMI, renal function, and selected chronic comorbidities, including hypertension, diabetes mellitus, and other underlying conditions.
Our study observed a high incidence of ICM-induced reactions (39.2%), exceeding reports from Japan (12%) and the USA (1%) [13,14], and slightly higher than estimates from African settings with comparable socioeconomic contexts (9.9-35.9%) [15-17]. This relatively high incidence should be interpreted in light of the prospective active-surveillance design, multiple follow-up time points, and broad outcome definition, which were intended to enhance detection of both mild and clinically significant events but may limit direct comparability with studies using passive surveillance or stricter definitions. Acute reactions predominated, with gastrointestinal (27.9%) and neurological (18.0%) symptoms most frequent, in line with global patterns [18,19]. Anaphylactic reactions (10.8%) were not uncommon; while some literature cites lower rates (≈0.2%) [20], such variation may reflect differences in population risk profiles, contrast formulations, case definitions, and intensity of monitoring. Delayed reactions were primarily renal (6.3%) and dermatologic (3.6%), within the global range (0.5-30%) [18,19]. Underreporting remains a concern in many sub-Saharan African settings due to limited post-procedure follow-up systems [15]. Our estimates also exceed those from Mexico (acute 26.3% and delayed 10.1%) [21], likely reflecting differences in study design and surveillance intensity; the single-arm prospective design used here facilitated real-time detection and improved event capture. These findings underscore the value of strengthened post-procedure follow-up to enhance detection and management of ICM-related reactions.
Several patient factors influenced ICM reactions. Overweight (53%) and normal-weight (51.2%) patients had higher reaction rates than obese patients (20.2%), a pattern consistent with findings from previous studies conducted in Tanzania (19). Similarly, a study conducted in Australia found that BMI is a risk factor for CA-AKI [22]. Stage 2 renal failure significantly increased the risk (RR = 2.14, p = 0.009), consistent with studies conducted in South Africa, Nigeria, and Kenya, which show that elevated creatinine levels double the risk [16,17,23]. Patients with neurological, cardiopulmonary, and oncological conditions had higher susceptibility, likely reflecting disease severity, immune compromise, and treatment-related vulnerability. The findings align with previous studies, which support that neurological risks may stem from blood-brain barrier compromise [24]. While other studies support that oncological patients had a 0.3-2.3% risk of getting ICM reactions, of which 11% develop AKI [25,26]. Anemia was also independently associated with ICM-induced reactions (RR = 1.49, p = 0.003), possibly due to impaired oxygen delivery, reduced physiological reserve, and vascular instability [27].
Although a prior history of medication allergy was not independently associated with ICM-induced reactions after adjustment, a higher proportion of reactions was observed among patients with documented drug allergies. While limited by small reported numbers, this finding remains clinically relevant and supports guideline recommendations for careful pre-procedure allergy assessment and heightened monitoring in this subgroup. In contrast with global studies linking high HbA1C (≥8.8%) with increased risk of ICM-induced reactions, our study found that participants with diabetes mellitus had a protective effect [28]. The observed association between diabetes mellitus and reduced risk of ICM-induced reactions should be interpreted cautiously. This finding is not suggestive of a protective biological effect. Still, it is more likely explained by unmeasured confounding, particularly the routine implementation of preventive measures such as hydration protocols in patients with diabetes mellitus [29,30], which were not systematically documented in this study.
Several limitations should be considered when interpreting these findings. The single-arm observational design restricts causal inference, and results should be interpreted as associative. The relatively high incidence of ICM-induced reactions may reflect the prospective active-surveillance approach, multiple follow-up time points, and inclusion of both mild and clinically significant events. Adverse reactions were not graded using international severity scales (e.g., American College of Radiology or European Society of Radiology), which may limit comparability; however, reactions were consistently classified by timing and organ system, and CA-AKI was defined using KDIGO criteria. Outcome assessment partly relied on interviews and phone follow-up, which may have introduced reporting bias, although standardized tools and trained data collectors were used. Preventive measures such as hydration protocols were not systematically documented, which may have influenced renal outcomes, including the observed protective association with diabetes mellitus. Finally, the study was conducted in two urban tertiary hospitals, which may limit generalizability beyond similar referral settings.
Conclusions
This study demonstrates that reactions to ICM are frequent and clinically significant, particularly in tertiary hospitals in Tanzania. Acute reactions were more common than delayed events, with gastrointestinal, neurological, and dermatological symptoms being most frequently reported, while delayed reactions primarily affected renal function. Key risk factors included normal and overweight BMI, neurological, oncological, and cardiopulmonary conditions, anemia, and stage 2 renal impairment. The association observed with diabetes mellitus should be interpreted cautiously and likely reflects unmeasured preventive practices rather than a true protective effect.
These findings support the need for context-specific risk assessment protocols, improved documentation of contrast exposure and preventive measures, and structured post-procedure monitoring, particularly for patients at high risk. Future studies incorporating standardized severity grading and broader, multicenter designs are warranted to improve comparability and support the development of context-specific contrast safety guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hypersensitivity reactions to iodinated contrast media Russ J Allergy Khludova LG Myasnikova TN Smirnov VV Latysheva TV Khaitov MR 8591162019
- 2Iodinated contrast media 7 2025 Murphy A 2017 https://radiopaedia.org/articles/iodinated-contrast-media-1
- 3Contrast media adverse reactions Radiopaedia 7 2025 Bell DJ 2024 https://radiopaedia.org/articles/contrast-media-adverse-reactions
- 4Clinical safety evaluation of contrast agents based on real-world evidence J Clin Pharm Ther Jiang C Li J Huang Y Huang D Lin J Jiang X 160016054620213429319410.1111/jcpt.13485 · doi ↗ · pubmed ↗
- 5American College of Radiology. Manual on contrast media Manual on Contrast Media ACR Committee on Drugs and Contrast Media Reston (VA)American College of Radiology 2023 https://www.acr.org/Clinical-Resources/Contrast-Manual
- 6The incidence of contrast-induced nephropathy and the need for dialysis in patients receiving angiography: a systematic review and meta-analysis Front Med (Lausanne) Wu MY Lo WC Wu YC Lin TC Lin CH Wu MS Tu YK 862534920223557300810.3389/fmed.2022.862534 PMC 9091353 · doi ↗ · pubmed ↗
- 7Adverse reactions to contrast material: a Canadian update Can Assoc Radiol J Morzycki A Bhatia A Murphy KJ 1871936820172774598810.1016/j.carj.2016.05.006 · doi ↗ · pubmed ↗
- 8Medico-legal cases in breast imaging in Canada: a trend analysis Can Assoc Radiol J Seely JM Payant L Zhang C 3693767520243754239610.1177/08465371231193366 · doi ↗ · pubmed ↗