Avacopan as an add-on therapy in a paediatric patient with new-onset granulomatosis with polyangiitis and acute kidney injury: a case report
Robin Mørk, Pernille Bøyesen, Ingvild Andrea Kindem, Jacob Lilleby, Ragnar Gunnarsson, Øyvind Molberg, Vibke Lilleby

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
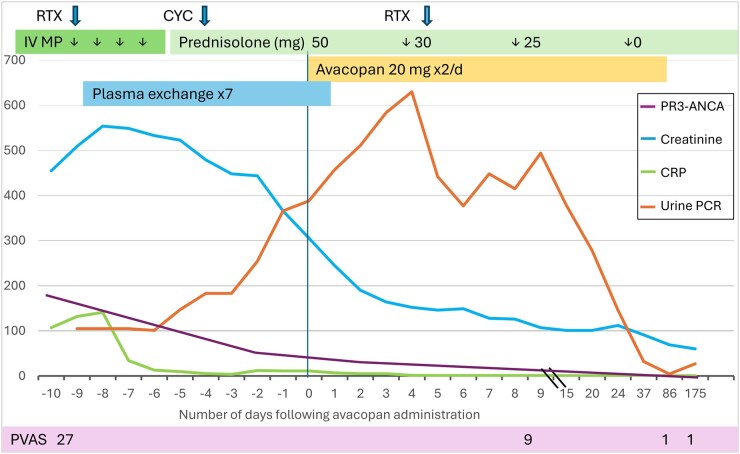 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVasculitis and related conditions · Inflammasome and immune disorders · Neutrophil, Myeloperoxidase and Oxidative Mechanisms
Dear Editor, Childhood-onset anti-neutrophilic cytoplasmatic antibody (ANCA)-associated vasculitis (AAV) is a rare disease with few paediatric data published. Despite advances in treatment, AAV remains a severe disease with frequent relapses and high cumulative morbidity. In a French study on childhood-onset AAV, 90% of the patients achieved remission after induction treatment, but after about 5 years of follow-up, 6% had died and 34% developed end-stage kidney disease [1]. Treatment-related adverse events, especially infections, are a major cause of mortality. The European vasculitis study (EUVAS) group reported a 1-year mortality rate of 11%, with 59% of deaths being therapy-related [2]. Highlighting the need for both effective and safe treatment alternatives.
The complement factor C5a plays an important role in the pathogenesis of AAV. Avacopan is an orally administered selective antagonist of the C5a receptor (C5aR) and has been shown to improve remission rates and kidney function in adults with AAV compared with oral glucocorticoids [3, 4]. There is limited experience with the use of avacopan in childhood-onset AAV. In our case, we initiated avacopan with the aim of preventing end-stage kidney injury.
We report the case of a 12-year-old girl diagnosed with granulomatosis with polyangiitis (GPA). She presented with a 2–4-weeks history of fever, sore throat, dry cough, recurrent epistaxis, nasal congestion and unilateral secretory otitis media. Initial antibiotic treatment for suspected pneumonia was ineffective. She was referred to our hospital following a rapid increase in serum creatinine from 134 to 350 µmol/l (ref.range 40–72) over four days and a markedly elevated PR3-ANCA IgG of >176 x10E3 IU/l (ref. <3). On admission, she exhibited haemoptysis. Blood tests showed anaemia (haemoglobin 8.4 g/dl; ref.range 11.7–15.3), elevated inflammatory markers (CRP 107 mg/l [ref. <4], ESR >100 mm/h [ref.range 1–10]) and severe kidney injury with creatinine 455 µmol/l, eGFR 12 ml/min/1.73m^2^, urea 20.3 mmol/l (ref.range 2.6–6.4), hypertension, proteinuria (total protein/creatinine ratio 105 mg/mmol, ref. range <30) and haematuria (10–30 erythrocytes/HPF), see Fig. 1.
Kidney biopsy revealed crescents in 23/24 glomeruli and acute tubulointerstitial inflammation. Chest CT showed multiple nodular lung consolidations and findings suggesting alveolar haemorrhage. Minor changes were found in her ethmoidal sinuses, mastoid cells and left middle ear. Otoscopy showed a ruptured tympanic membrane. The Paediatric vasculitis activity score (PVAS) was 27/63 points, reflecting high disease activity.
Induction therapy included intravenous methylprednisolone pulses, rituximab (RTX) and prednisolone. Due to rapid-progressive glomerulonephritis with creatinine reaching 509 µmol/l and eGFR 11 ml/min/1.73m^2^, plasma exchange was added with a total of 7 exchanges over 10 days (Fig. 1) [5]. Haemodialysis was required once due to oliguria and uraemia. A single cyclophosphamide (CYC) dose (15 mg/kg) was administered (day-4), both due to the severity of the disease and the potential RTX depletion that follows plasma exchange.
Due to rapid-progressive, severe kidney involvement, C5aR inhibition therapy with avacopan was approved for off-label use by the local health authorities. Avacopan was dosed 20 mg bid [4]. Kidney improvement was observed within two weeks after the start of induction therapy with decreasing creatinine (Fig. 1). Prednisolone was rapidly tapered from 50 mg qd (1 mg/kg) to discontinuation within 4 weeks (Fig. 1). By day 37 after introducing avacopan, PVAS improved to 9, CRP was normalised, and PR3-ANCA, creatinine and urine PCR were nearly normalised (Fig. 1).
At 3 and 6 months after initiating avacopan, she exhibited no active disease, with no proteinuria, creatinine at 60 µmol/l and eGFR at 94 ml/min/1.73m^2^. Hypertension was absent. PVAS improved further to 1, and the Paediatric Vasculitis Damage Index (PVDI) was 1 (ENT—hearing loss). Avacopan was well tolerated, with the only potential side effects being mild neutropenia and lymphopenia, which did not necessitate discontinuation of the treatment.
Discussion
This case highlights avacopan’s potential as a steroid-sparing agent in childhood-onset GPA with severe kidney involvement. The rapid prednisolone taper and sustained remission suggest its efficacy and tolerability, though there are few published data on the use of avacopan in children.
To the best of our knowledge, this is the first report describing the successful use of avacopan as part of induction therapy in new-onset paediatric GPA, together with a description of the early clinical course and outcome. There are only three previous case reports published on avacopan use in paediatric patients [6–8]. All patients received 30 mg bid, and one developed severe liver function abnormalities which led to treatment discontinuation [7]. Results from an ongoing phase 3 trial on avacopan in childhood-onset AAV in combination with rituximab or cyclophosphamide are estimated in 2030 (NCT06321601).
While our patient demonstrated significant clinical improvement, the efficacy of the treatment could not solely be attributable to avacopan, given the concurrent administration of rituximab, plasma exchange and one course of cyclophosphamide. Nevertheless, avacopan facilitated rapid glucocorticoid (GC) tapering, consistent with its established steroid-sparing effect and recent incorporation in international consensus guidelines on adult-onset AAV [5].
GCs remain essential in AAV management for rapid disease control, but adverse events, including infections, cardiometabolic disease and therapy-related mortality, are well recognised. In recent years, there has been growing recognition of the benefits associated with the utilisation of lower induction doses or shorter courses of GCs in combination with CYC or RTX [5].
Avacopan add-on therapy offers the potential for substantially reduced GC exposure compared with the current standard of care. As observed in our patient, avacopan may serve as a steroid-sparing, effective and safe treatment option for paediatric AAV in the future. However, the access to both avacopan and rituximab might be limited globally, and alternative treatment strategies to reduce GC exposure are of clinical importance. Further research is warranted to determine optimal GC tapering strategies in conjunction with avacopan and other combination therapies, thereby ensuring patient safety and providing clear, evidence-based guidance for clinicians.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sacri A-S , Chambaraud T, Ranchin B et al Clinical characteristics and outcomes of childhood-onset ANCA-associated vasculitis: a French nationwide study. Nephrol Dial Transplant 2015;30(Suppl 1):i 104–12.25676121 10.1093/ndt/gfv 011 · doi ↗ · pubmed ↗
- 2Little MA , Nightingale P, Verburgh CA et al; European Vasculitis Study (EUVAS) Group. Early mortality in systemic vasculitis: relative contribution of adverse events and active vasculitis. Ann Rheum Dis 2010;69:1036–43.19574233 10.1136/ard.2009.109389 · doi ↗ · pubmed ↗
- 3Cortazar FB , Niles JL, Jayne DRW et al; ADVOCATE Study Group. Renal recovery for patients with ANCA-associated vasculitis and low e GFR in the ADVOCATE trial of avacopan. Kidney Int Rep 2023;8:860–70.37069984 10.1016/j.ekir.2023.01.039PMC 10105055 · doi ↗ · pubmed ↗
- 4Jayne DRW , Merkel PA, Schall TJ, Bekker P; ADVOCATE Study Group. Avacopan for the treatment of ANCA-associated vasculitis. N Engl J Med 2021;384:599–609.33596356 10.1056/NEJ Moa 2023386 · doi ↗ · pubmed ↗
- 5KDIGO 2024. Clinical Practice Guideline for the Management of Antineutrophil Cytoplasmic Antibody (ANCA)-associated vasculitis. Kidney Int 2024;105:s 71–s 116.38388102 10.1016/j.kint.2023.10.008 · doi ↗ · pubmed ↗
- 6Ennis D , Yeung RS, Pagnoux C. Long-term use and remission of granulomatosis with polyangiitis with the oral C 5a receptor inhibitor avacopan. BMJ Case Reports 2020;13:e 236236.10.1136/bcr-2020-236236 PMC 759747733122227 · doi ↗ · pubmed ↗
- 7Nishino T , Tomori S, Haruyama M, Takahashi K, Mimaki M. A case of rapid avacopan-induced liver injury in pediatric granulomatosis with polyangiitis. Pediatr Nephrol 2024;39:2919–22.38619581 10.1007/s 00467-024-06376-8 · doi ↗ · pubmed ↗
- 8Zotta F , Diomedi-Camassei F, Gargiulo A et al Successful treatment with avacopan (CCX 168) in a pediatric patient with C 3 glomerulonephritis. Pediatr Nephrol 2023;38:4197–201.37306717 10.1007/s 00467-023-06035-4 · doi ↗ · pubmed ↗