Feasibility of bioabsorbable polyglycolic acid sheet and fibrin glue therapy for ulcer sealing after gastric endoscopic submucosal dissection
Tomoyuki Shibata, Takamitsu Ishizuka, Keishi Koyama, Hyuga Yamada, Noriyuki Horiguchi, Kohei Funasaka, Ryoji Miyahara, Tomomitsu Tahara, Yoshiki Hirooka

TL;DR
This study shows that using a bioabsorbable sheet and fibrin glue after a gastric procedure helps prevent bleeding and promotes healing without needing extra treatments.
Contribution
The study demonstrates the feasibility of using BAPGAS and FG for sealing ulcers after gastric ESD, reducing the need for endoscopic hemostasis.
Findings
No bleeding occurred in any patient, and endoscopic hemostasis was not required.
Seven out of nine patients achieved scar healing by day 56 without complications.
BAPGAS covering time did not correlate with ESD procedure time or resected area.
Abstract
Combined therapy using a bioabsorbable polyglycolic acid sheet (BAPGAS) and fibrin glue (FG) has been employed to prevent postoperative perforation. More recently, this therapy has been applied to ulcers that develop after endoscopic submucosal dissection (ESD) for early digestive tract tumors. This study was performed to evaluate the sealing effect of this combined therapy on ulcers that develop after ESD for early gastric tumors. This study included nine patients with early gastric cancer or adenoma who were treated with ESD. Ulcers that developed after ESD were covered with BAPGAS and sealed with FG spray. To assess ulcer bleeding and healing status, endoscopy was performed on postoperative days 1, 7, 28, and 56. On days 1 and 7, clots were observed in only two patients, and no bleeding occurred in any patient. As a result, endoscopic hemostasis was not required. In one patient,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
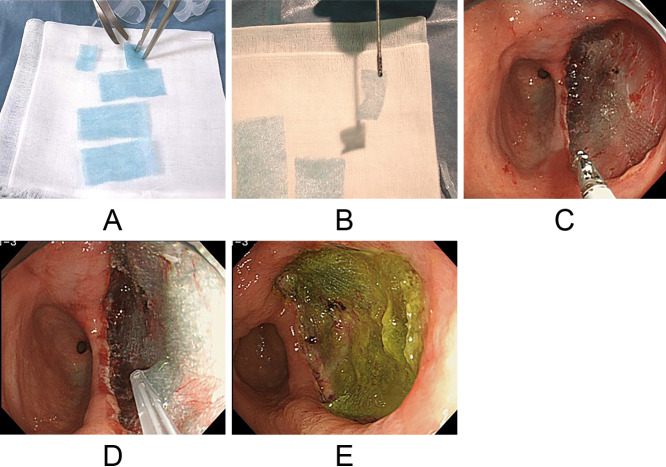 Figure 1
Figure 1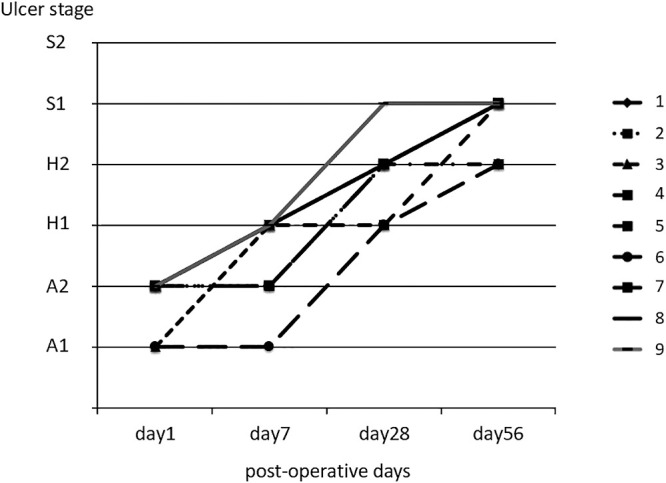 Figure 2
Figure 2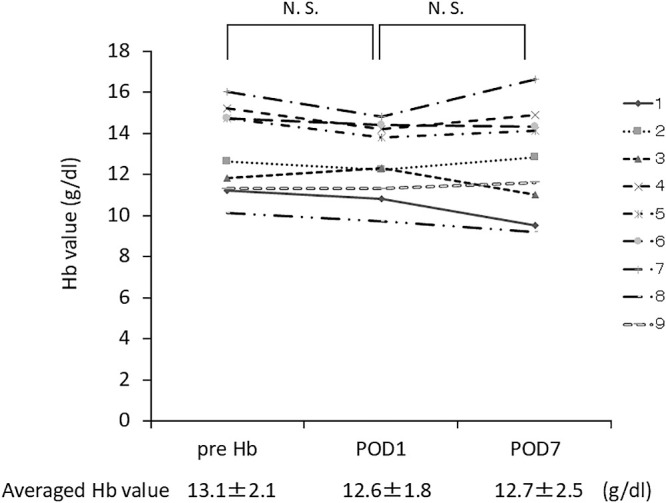 Figure 3
Figure 3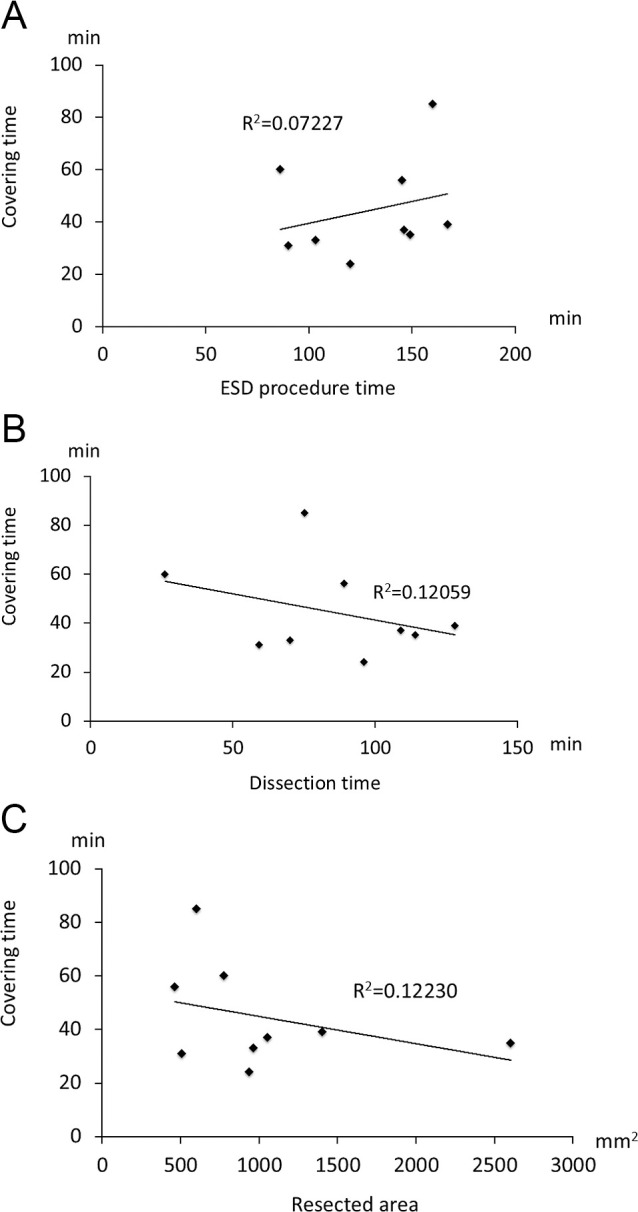 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastric Cancer Management and Outcomes · Gastrointestinal Tumor Research and Treatment · Helicobacter pylori-related gastroenterology studies
Introduction
The mortality rate of patients with gastric cancer has gradually declined; however, gastric cancer remains the second most common cause of malignant neoplasms in Japan. In recent years, the number of early-stage gastric cancer cases has increased because of advances in endoscopic diagnosis.
Endoscopic submucosal dissection (ESD) is a relatively new technique developed for en bloc resection of lesions such as large early gastric cancers, and it offers a major advantage over endoscopic mucosal resection.^1,2^ ESD is performed and developed as a gastric function-preserving treatment and is a less radical option than surgical resection for early gastric cancer. Because ESD is often used to treat tumors with extensive surface areas, it is important to examine the frequency of bleeding complications following the procedure. Long-term outcomes, bleeding rates, en bloc resection rates, and treatment times have been studied previously.^3–6^ As a result of these studies, ESD has been recognized as a safe and reliable procedure.
Combined therapy using a bioabsorbable polyglycolic acid sheet (BAPGAS) (Neoveil; Gunze Co., Kyoto, Japan) and fibrin glue (FG) (Beriplast P combi-set; CSL Behring Pharma, Tokyo, Japan) has been employed in many cases to prevent postoperative perforation. As a bioabsorbable material, BAPGAS is hydrolyzed and absorbed approximately 15 weeks after surgical application. Consequently, this approach has been used for ulcers requiring short-term sealing.^7,8^ Recently, the combined therapy has gained attention in the field of endoscopy for its sealing effect on ulcers that develop following ESD for early-stage digestive tract tumors.^9^
This study was performed to evaluate the sealing effect of combined therapy using BAPGAS and FG on ulcers that developed after endoscopic treatment for early gastric cancer.
Methods
Patients receiving ESD treatment
This study included nine patients with early gastric cancer or adenoma (eight men, one woman; mean age, 73.0 years) who were treated with ESD at our endoscopic center.
Patients with systemic diseases, malignancies in other organs, or those who had taken nonsteroidal anti-inflammatory drugs were excluded. Written informed consent was obtained from all participants. The study protocol was approved by our University Ethical Committee (HM13-223).
Gastric cancer treatment was conducted in accordance with the expanded criteria outlined in the national cancer treatment guidelines.^10^ All lesions were diagnosed as mucosal cancer following ESD.
ESD procedure
ESD was performed using an insulation-tipped diathermic knife (IT knife; Olympus, Tokyo, Japan) to remove tumors with a minimum lateral margin of 5 mm. A high-frequency electrosurgery device (VAIO 300D; ERBE Co. Ltd., Tübingen, Germany) was used with the following settings: argon plasma coagulation at 40 W or coagulation at 30 W for marking, endo cut effect 3 at 80 W for dissection, and endo cut effect 3 at 80 W or coagulation at 50 W for abrasion. The injection solution for local administration was prepared by mixing 2 g of glycerin (20 mL), 80 mg of 0.4% sodium hyaluronate (20 mL), and 2 mL of indigo carmine solution.
BAPGAS and FG treatment for ulcers
Ulcers that developed after ESD were covered with BAPGAS and sealed using FG spray. Specifically, the BAPGAS sheet was cut into small pieces, placed onto the ulcer surface, and then firmly adhered by spraying FG (Figure 1A–D). A proton pump inhibitor, esomeprazole (AstraZeneca Co. Ltd., Tokyo, Japan), was administered for 2 weeks, and a mucosal protective agent, rebamipide (Otsuka Pharmaceutical Co. Ltd., Tokyo, Japan), was used concurrently for 8 weeks.
To evaluate bleeding and ulcer healing status, endoscopic examinations were performed on postoperative days 1, 7, 28, and 56.
Examination of factors associated with BAPGAS therapy
Post-ESD complications, including bleeding and perforation, were assessed. Tumor locations were classified using the UML system, which divides both the lesser and greater curvatures into three equal segments: upper (U), middle (M), and lower (L), in accordance with the Japanese gastric cancer treatment guidelines.^11^ Tumor morphology was also described following these guidelines. Procedure-related data were recorded, including the total ESD time (min), endoscopic dissection time (defined as the duration of mucosal dissection only), and resected area (mm^2^). Hemoglobin (Hb) levels were measured within 1 week prior to ESD and again on postoperative days 1 and 7.
Statistical analysis
All statistical analyses were performed using JMP version 10 (SAS Institute, Cary, NC, USA). Data are expressed as mean±standard error. The Wilcoxon signed-rank test and Spearman’s rank correlation test were used for statistical evaluations. A p-value of <0.05 was considered statistically significant.
Results
Patient characteristics
Patient characteristics, tumor locations, and final diagnoses are summarized in Table 1. Only one case of adenoma was identified, and no metastases were detected by pathological examination.
Ulcer status
On days 1 and 7 after ESD, clots were observed on the ulcer in only two patients, and no bleeding was noted in any patient; thus, endoscopic hemostasis was not required (Figure 1E). In one patient, scar healing was achieved 28 days after ESD. By 56 days post-ESD, scar healing was observed in seven of the nine patients, and no bleeding was reported in any patient (Figure 2).
Changes in Hb levels after ESD
Changes in Hb levels before and after ESD were not statistically significant (from 13.1±0.7 to 12.6±0.6, p=0.0703) (Figure 3). Additionally, Hb levels 1 week after ESD (12.7±0.8) showed no change compared with those on the day 1 post-procedure (Figure 3).
Analysis of factors associated with BAPGAS covering time
The average endoscopic dissection time was 85 minutes, and the total average ESD procedure time was 130 minutes. Accordingly, the BAPGAS covering time was approximately 40 minutes (41±12 min). No factors were found to be significantly associated with the BAPGAS covering time (Figure 4A–C).
Discussion
This is the first feasibility study to evaluate the usefulness of combined therapy with BAPGAS and FG for preventing bleeding from artificial ulcers that develop after gastric ESD. In this study, we examined endoscopic treatment time, the frequency of endoscopic hemostasis, ulcer healing speed, and Hb levels following gastric ESD.
Today, ESD is widely used in the treatment of digestive tract cancers, particularly early gastric cancer. Empirically, it is considered safer than surgery. However, postoperative adverse events can still occur, including bleeding from or perforation of the ulcer that forms after ESD. The postoperative bleeding rate is approximately 5%, while the perforation rate generally ranges from 2% to 4%.
We measured Hb as a marker of postoperative anemia. Hb levels did not show a significant decrease. Only a few reports have included Hb measurements in relation to endoscopic treatment, and detailed analyses of potential changes in Hb levels due to such procedures remain limited.^12,13^ Some studies have investigated delayed bleeding and its associated risk factors, identifying variables such as tumor size and location.^14–17^ However, findings on tumor location as a risk factor have been inconsistent. Only one study has examined the relationship between delayed bleeding and operation time,^14^ and it found no association between the two. In that study, operation time was measured in hours, whereas in our study, we used minutes. This difference in measurement units may explain the discrepancy in findings regarding the relationship between ESD procedure time and postoperative anemia.
Because BAPGAS and FG therapy is also known to help prevent delayed perforation,^8,9^ there is a possibility that these covering sheets could interfere with the prompt healing of ulcers. To evaluate this, we monitored ulcer healing speed and status after ESD using endoscopy on days 7, 28, and 56 post-procedure. We found that all ulcers had progressed to at least the second stage of healing, and the healing status was deemed clinically satisfactory. Takao et al. created ESD-induced ulcers in a porcine model and compared ulcer healing between a group treated with BAPGAS and FG and a control group.^18^ Although no significant differences in overall healing were observed, the BAPGAS with FG group demonstrated abundant neovascularization and good granulation tissue. These findings suggest that the use of BAPGAS with FG may positively influence the ulcer healing process. However, these results should be confirmed in a large-scale study.
In conclusion, combined therapy with BAPGAS and FG is effective for preventing bleeding from artificial ulcers that develop after ESD and may help shorten the overall procedure time by reducing the need for endoscopic hemostasis. Furthermore, because the ulcer healing speed was comparable to that achieved with conventional treatment, this method shows promise as a new approach for managing post-ESD artificial ulcers.
Notably, this study was conducted at a single facility with a small sample size. Therefore, multicenter randomized controlled trials are needed to further validate and confirm these findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Oka S, Tanaka S, Kaneko I, Mouri R, Hirata M, Kawamura T, Yoshihara M, Chayama K. Advantage of endoscopic submucosal dissection compared with EMR for early gastric cancer. Gastrointest Endosc 2006; 64: 877–883.17140890 10.1016/j.gie.2006.03.932 · doi ↗ · pubmed ↗
- 2Takeuchi Y, Uedo N, Iishi H, Yamamoto S, Yamamoto S, Yamada T, Higashino K, Ishihara R, Tatsuta M, Ishiguro S. Endoscopic submucosal dissection with insulated-tip knife for large mucosal early gastric cancer: a feasibility study (with videos). Gastrointest Endosc 2007; 66: 186–193.17591498 10.1016/j.gie.2007.03.1059 · doi ↗ · pubmed ↗
- 3Hirasaki S, Tanimizu M, Nasu J, Shinji T, Koide N. Treatment of elderly patients with early gastric cancer by endoscopic submucosal dissection using an insulated-tip diathermic knife. Intern Med 2005; 44: 1033–1038.16293912 10.2169/internalmedicine.44.1033 · doi ↗ · pubmed ↗
- 4Shimura T, Joh T, Sasaki M, Kataoka H, Tanida S, Ogasawara N, Yamada T, Kubota E, Wada T, Inukai M, Yoshioka N, Saida Y. Endoscopic submucosal dissection is useful and safe for intramucosal gastric neoplasms in the elderly. Acta Gastroenterol Belg 2007; 70: 323–330.18330087 · pubmed ↗
- 5Kakushima N, Fujishiro M, Kodashima S, Muraki Y, Tateishi A, Yahagi N, Omata M. Technical feasibility of endoscopic submucosal dissection for gastric neoplasms in the elderly Japanese population. J Gastroenterol Hepatol 2007; 22: 311–314.17295759 10.1111/j.1440-1746.2006.04563.x · doi ↗ · pubmed ↗
- 6Isomoto H, Ohnita K, Yamaguchi N, Fukuda E, Ikeda K, Nishiyama H, Akiyama M, Ozawa E, Nakao K, Kohno S, Shikuwa S. Clinical outcomes of endoscopic submucosal dissection in elderly patients with early gastric cancer. Eur J Gastroenterol Hepatol 2010; 22: 311–317.19494784 10.1097/MEG.0b 013e 32832 c 61d 7 · doi ↗ · pubmed ↗
- 7Ueda K, Tanaka T, Hayashi M, Li TS, Tanaka N, Hamano K. Mesh-based pneumostasis contributes to preserving gas exchange capacity and promoting rehabilitation after lung resection. J Surg Res 2011; 167: e 71–e 75.20097374 10.1016/j.jss.2009.11.009 · doi ↗ · pubmed ↗
- 8Uemura K, Murakami Y, Hayashidani Y, Sudo T, Hashimoto Y, Ohge H, Sueda T. Combination of polyglicolic acid felt and fibrin glue for prevention of pancreatic fistula following pancreaticoduodenectomy. Hepatogastroenterology 2009; 56: 1538–1541.19950825 · pubmed ↗