Diagnostic Accuracy of Point-of-Care Ultrasound in Detecting Pneumothorax: A Systematic Review and Meta-Analysis
Lavanya Ranganath, Deepti Gowda, Manjunath G.N.

TL;DR
This study reviews and analyzes the accuracy of using point-of-care ultrasound to detect pneumothorax in emergency settings.
Contribution
The paper provides an updated meta-analysis of POCUS diagnostic accuracy for pneumothorax using PRISMA-DTA guidelines.
Findings
POCUS has a pooled sensitivity of 74.3% and specificity of 99.1% for detecting pneumothorax.
Higher sensitivity is observed with prospective studies, non-trauma patients, and experienced operators.
Specificity remains consistently high across all subgroups, with no significant publication bias detected.
Abstract
Point-of-care ultrasound (POCUS) is increasingly used in emergency departments for the rapid detection of pneumothorax. While POCUS offers bedside convenience, its diagnostic accuracy compared with standard imaging remains variable, necessitating an updated synthesis of evidence. We conducted a systematic review and meta-analysis following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Diagnostic Test Accuracy (PRISMA-DTA) guidelines. Databases including PubMed, Scopus, Web of Science, and Google Scholar were searched for studies evaluating POCUS for pneumothorax detection in emergency settings. Data on sensitivity, specificity, and operator characteristics were extracted. Study quality was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2), and a bivariate random-effects model was used to pool diagnostic accuracy metrics.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
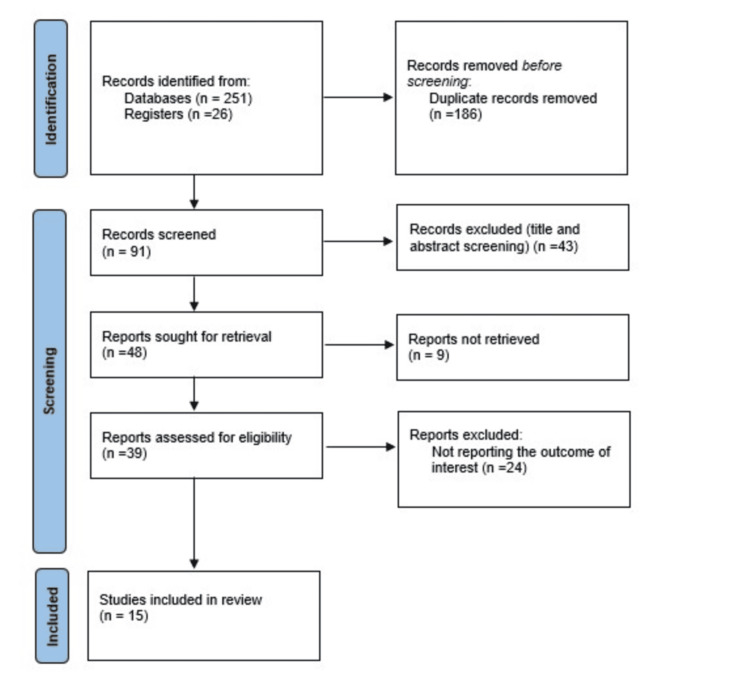 Figure 1
Figure 1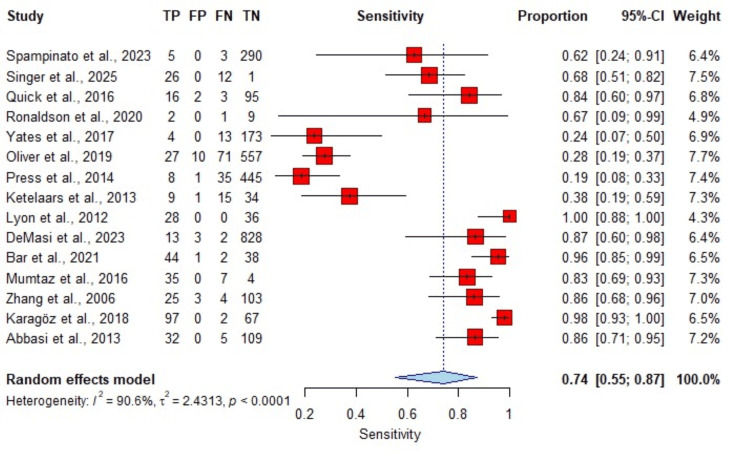 Figure 2
Figure 2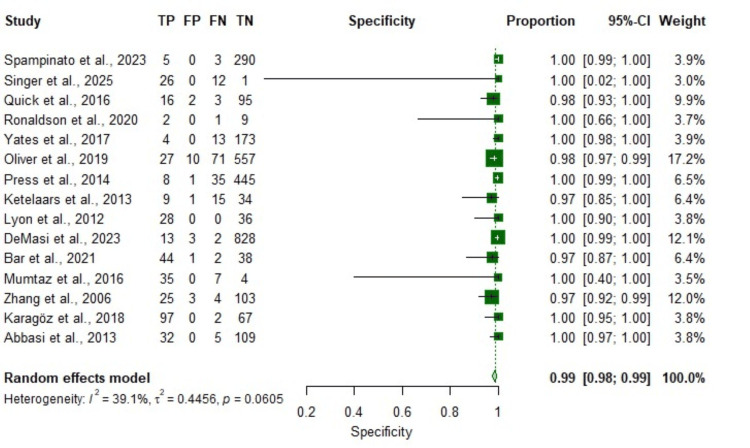 Figure 3
Figure 3| Author and Year | Country | Study Design | Population | Sample Size | Pneumothorax | Ultrasound Operator | QUADAS-2 |
| Spampinato et al. (2023) [ | Italy | Retrospective cohort | Adult | 844 | 8 | Emergency physician | Low risk |
| Singer et al. (2025) [ | USA | Retrospective cohort | Adult | 541 | 40 | Emergency physician | Low risk |
| Quick et al. (2016) [ | USA | Cross-sectional | Adult | 149 | 19 | Other | Low risk |
| Ronaldson et al. (2020) [ | UK | Cross-sectional | Adult | 12 | 3 | Nurse paramedic | Low risk |
| Yates et al. (2017) [ | USA | Cross-sectional | Adult | 190 | 17 | Nurse paramedic | Low risk |
| Oliver et al. (2019) [ | UK | Cross-sectional | Adult and pediatric | 361 | 98 | Other | High risk |
| Press et al. (2014) [ | USA | Cross-sectional | Adult | 211 | 43 | Nurse paramedic | Low risk |
| Ketelaars et al. (2013) [ | Netherlands | Cross-sectional | Adult and pediatric | 59 | 24 | Other | High risk |
| Lyon et al. (2012) [ | USA | Cross-sectional | Adult | 64 | 28 | Emergency physician | High risk |
| DeMasi et al. (2023) [ | USA | Retrospective cohort | Adult | 846 | 15 | Resident | Low risk |
| Bar et al. (2021) [ | Israel | Prospective cohort | Adult | 85 | 46 | Resident | Low risk |
| Mumtaz et al. (2016) [ | Pakistan | Cross-sectional | Adult | 46 | 42 | Other | Low risk |
| Zhang et al. (2006) [ | China | Prospective cohort | Adult | 135 | 29 | Emergency physician | Low risk |
| Karagöz et al. (2018) [ | Turkey | Cross-sectional | Adult | 166 | 99 | Emergency physician | Low risk |
| Abbasi et al. (2013) [ | Iran | Cross-sectional | Adult | 146 | 37 | Emergency physician | High risk |
| Parameter | Coefficient | Std. Error | 95% Confidence Interval |
| Bivariate model | |||
| E(logitSe) | 3.6258 | 0.6537 | 2.3446-4.9069 |
| E(logitSp) | 2.6758 | 0.5389 | 1.6195-3.7320 |
| Var(logitSe) | 2.6091 | 1.8534 | 0.6484-10.4989 |
| Var(logitSp) | 3.8818 | 1.6706 | 1.6700-9.0232 |
| Corr(logits) | -0.3218 | 0.3504 | -0.8004-0.4073 |
| HSROC model | |||
| Lambda | 6.4272 | 0.7223 | 5.0115-7.8429 |
| Theta | 0.7908 | 0.6555 | -0.4940-2.0756 |
| Beta | 0.1986 | 0.4075 | -0.6000-0.9973 |
| s2 alpha | 4.3166 | 2.5812 | 1.3370-13.9361 |
| s2 theta | 2.1033 | 1.1412 | 0.7262-6.0918 |
| Summary point estimates | |||
| Sensitivity (Se) | 0.9741 | 0.0165 | 0.9125-0.9927 |
| Specificity (Sp) | 0.9356 | 0.0325 | 0.8347-0.9767 |
| Diagnostic odds ratio (DOR) | 545.4 | - | - |
| Positive LR (LR+) | 15.1208 | 7.5771 | 5.6629-40.3751 |
| Negative LR (LR-) | 0.0277 | 0.0175 | 0.0081-0.0954 |
| 1/LR- | 36.0702 | 22.7498 | 10.4783-124.1677 |
| Covariance | -1.0241 | - | - |
| Subgroup Variable | Subgroup | N Studies | Sensitivity (95% CI) | I2 | Specificity (95% CI) | I2 |
| Study design | Retrospective cohort | 3 | 0.730 (0.570-0.860) | 0.412 | 0.987 (0.958-0.998) | 0.210 |
| Cross-sectional | 10 | 0.510 (0.390-0.630) | 0.975 (0.952-0.990) | |||
| Prospective cohort | 2 | 0.845 (0.705-0.940) | 0.981 (0.955-0.994) | |||
| Population | Adult | 13 | 0.590 (0.470-0.700) | 0.362 | 0.976 (0.960-0.989) | 0.240 |
| Adult and pediatric | 2 | 0.680 (0.510-0.800) | 0.987 (0.969-0.996) | |||
| Patient condition | Trauma | 8 | 0.550 (0.420-0.680) | 0.501 | 0.977 (0.954-0.991) | 0.430 |
| Non-trauma | 7 | 0.885 (0.755-0.965) | 0.992 (0.974-0.998) | |||
| US protocol | eFAST | 6 | 0.650 (0.495-0.775) | 0.298 | 0.988 (0.968-0.998) | 0.395 |
| Other | 4 | 0.540 (0.345-0.720) | 0.977 (0.940-0.992) | |||
| Two-point | 4 | 0.780 (0.605-0.900) | 0.985 (0.967-0.996) | |||
| US operator | Emergency physician | 5 | 0.820 (0.680-0.900) | 0.420 | 0.988 (0.970-0.998) | 0.265 |
| Nurse/paramedic | 3 | 0.410 (0.240-0.600) | 0.990 (0.978-0.998) | |||
| Resident | 2 | 0.870 (0.700-0.955) | 0.987 (0.960-0.997) | |||
| Other | 4 | 0.560 (0.385-0.720) | 0.978 (0.955-0.992) | |||
| Operator experience | Trained | 6 | 0.615 (0.492-0.725) | 0.497 | 0.986 (0.968-0.997) | 0.430 |
| Experienced | 4 | 0.680 (0.505-0.810) | 0.977 (0.951-0.990) | |||
| Mixed | 3 | 0.650 (0.450-0.810) | 0.987 (0.969-0.997) | |||
| Not specified | 2 | 0.500 (0.290-0.715) | 0.985 (0.968-0.997) | |||
| QUADAS-2 risk | Low risk | 11 | 0.700 (0.555-0.820) | 0.398 | 0.977 (0.951-0.989) | 0.495 |
| High risk | 4 | 0.610 (0.490-0.720) | 0.987 (0.968-0.997) |
| Omitted Study | Sensitivity (95% CI) | P-value | Specificity (95% CI) | P-value |
| Overall Model | 0.74 (0.55-0.87) | 0.99 (0.98-0.99) | ||
| Spampinato et al. (2023) | 0.75 (0.56-0.88) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Singer et al. (2025) | 0.74 (0.55-0.87) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Quick et al. (2016) | 0.73 (0.54-0.87) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Ronaldson et al. (2020) | 0.74 (0.55-0.87) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Yates et al. (2017) | 0.77 (0.60-0.89) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Oliver et al. (2019) | 0.78 (0.62-0.89) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Press et al. (2014) | 0.78 (0.62-0.89) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Ketelaars et al. (2013) | 0.76 (0.58-0.88) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Lyon et al. (2012) | 0.72 (0.53-0.86) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| DeMasi et al. (2023) | 0.73 (0.54-0.87) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Bar et al. (2021) | 0.72 (0.53-0.86) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Mumtaz et al. (2016) | 0.73 (0.54-0.87) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Zhang et al. (2006) | 0.73 (0.54-0.86) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Karagöz et al. (2018) | 0.72 (0.53-0.86) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
| Abbasi et al. (2013) | 0.73 (0.54-0.86) | 0.00 | 0.99 (0.98-0.99) | 0.00 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Cardiac Arrest and Resuscitation · Appendicitis Diagnosis and Management
Introduction and background
Point-of-care ultrasound (POCUS) has emerged as an important bedside diagnostic tool in emergency and critical care medicine, allowing clinicians to rapidly obtain focused imaging information to guide immediate management decisions [1,2]. POCUS examinations are performed and interpreted directly by the treating clinician, enabling real-time clinical integration and repeat assessment where necessary [2].
Pneumothorax is a potentially life-threatening condition, particularly in trauma and critically ill patients [3]. Thoracic ultrasound has become an integral component of modern emergency assessment protocols [4,5]. POCUS offers a rapid and readily available method to evaluate for traumatic and non-traumatic pneumothorax at the bedside, particularly when clinical examination findings are subtle or confounded by concurrent injuries or mechanical ventilation [6,7]. Computed tomography (CT) remains the reference standard for diagnosing pneumothorax and can detect small or occult pneumothoraces not visible on chest radiography; however, CT is time-consuming, costly, and not always immediately available in unstable patients [7,8].
Systematic reviews and meta-analyses have demonstrated that thoracic ultrasound is more sensitive than supine chest radiography for detecting traumatic pneumothorax, while maintaining high specificity [8-10]. However, reported sensitivity varies depending on the clinical population, reference standard, and inclusion of CT-only (occult) pneumothoraces [3,9,11]. This diagnostic test accuracy systematic review is reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses for Diagnostic Test Accuracy (PRISMA-DTA) guidance [12]. Diagnostic accuracy is further influenced by operator training, experience, and scanning protocol [13,14].
The role of POCUS has expanded beyond the emergency department into prehospital, aeromedical, and retrieval settings, where conventional imaging is limited and rapid decision-making is essential [15-22]. Given the increasing use of thoracic POCUS across diverse acute care environments, this systematic review and meta-analysis aims to evaluate its diagnostic accuracy for pneumothorax, summarising pooled sensitivity and specificity and exploring sources of heterogeneity. Recent emergency department evaluations and aeromedical feasibility studies further support the broad applicability of thoracic POCUS across acute care environments [23,24].
Review
Methods
Study Design
This systematic review and meta-analysis were conducted in accordance with PRISMA-DTA reporting principles for diagnostic test accuracy studies [12]. A review protocol was developed prior to study initiation.
Search Strategy
A comprehensive literature search was performed in PubMed, Scopus, Web of Science, and Google Scholar from database inception to December 31, 2025. Search terms included “point-of-care ultrasound,” “POCUS,” “thoracic ultrasound,” “pneumothorax,” “sensitivity,” and “specificity,” using Boolean operators and Medical Subject Headings (MeSH) where appropriate. Reference lists of relevant articles and systematic reviews were manually screened.
Eligibility Criteria
Inclusion criteria were patients of any age with suspected pneumothorax; thoracic POCUS as the index test; CT, chest radiography, or intraoperative findings as the reference standard; observational diagnostic accuracy studies; and sufficient data to derive true-positive, false-positive, true-negative, and false-negative results.
Exclusion criteria included case reports, editorials, narrative reviews, animal studies, studies with fewer than 10 participants, and studies conducted outside emergency or acute care settings.
Study Selection and Data Extraction
Two reviewers independently screened titles, abstracts, and full-text articles. Extracted data included study design, setting, sample size, patient population, pneumothorax prevalence, ultrasound protocol, operator type and training, reference standard, and diagnostic accuracy outcomes. Disagreements were resolved by consensus with a third reviewer.
Quality Assessment
Risk of bias was assessed using the Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool, evaluating patient selection, index test conduct, reference standard, and flow and timing.
Statistical Analysis
Meta-analysis was performed using R (version 4.3.1; R Foundation for Statistical Computing, Vienna, Austria) with diagnostic accuracy modelling packages. Pooled sensitivity, specificity, likelihood ratios, and diagnostic odds ratios (ORs) were estimated using a bivariate random-effects model. Summary estimates were presented with 95% confidence intervals (CIs). Subgroup analyses explored the effects of clinical setting, ultrasound protocol, operator type, and study quality. Leave-one-out sensitivity analyses were conducted to assess the influence of individual studies.
Results
Study Selection
The literature search identified 277 records, of which 186 duplicates were removed. Ninety-one titles and abstracts were screened, and 48 full-text articles were assessed for eligibility. Fifteen studies met the inclusion criteria and were included in the final meta-analysis (Figure 1) [9,11,13-22,25].
PRISMA flow chart illustrating the study selection process for this systematic review and meta-analysis.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Characteristics of Included Studies
Included studies were conducted across the United States, Europe, Asia, and the Middle East. Study designs included prospective and retrospective cohort studies as well as cross-sectional analyses. Sample sizes ranged from 12 to 846 participants. Ultrasound examinations were performed by physicians, residents, nurses, paramedics, and retrieval practitioners. Study quality varied across QUADAS-2 domains (Table 1).
Diagnostic Accuracy
Pooled diagnostic accuracy estimates for thoracic POCUS were as follows: sensitivity: 0.9741 (95% CI 0.9125-0.9927), specificity: 0.9356 (95% CI 0.8347-0.9767), positive likelihood ratio: 15.12, and negative likelihood ratio: 0.028. These findings indicate high overall diagnostic performance for bedside detection of pneumothorax using POCUS.
Detailed pooled estimates and hierarchical summary receiver operating characteristic (HSROC) parameters are presented in Table 2, and forest plots for sensitivity and specificity are shown in Figures 2-3, in accordance with PRISMA-DTA reporting standards.
Forest plot of pooled sensitivity.TP: true positive; FP: false positive; FN: false negative; TN: true negative; CI: confidence intervalReferences [23,3,21,22,24,19,20,16,17,9,14,18,25,15,13]
Forest plot of pooled specificity.TP: true positive; FP: false positive; FN: false negative; TN: true negative; CI: confidence intervalReferences [23,3,21,22,24,19,20,16,17,9,14,18,25,15,13]
Subgroup Analysis
Higher sensitivity was observed in non-trauma populations, in studies employing focused two-point lung ultrasound protocols, and among examinations performed by physicians or residents with formal ultrasound training [13,14,22]. Specificity remained consistently high across subgroups (Table 3).
Sensitivity Analysis
Leave-one-out analyses demonstrated that no single study disproportionately influenced pooled estimates, supporting the robustness of the findings (Table 4).
Discussions and clinical implications
This systematic review and meta-analysis demonstrate that thoracic POCUS has high pooled sensitivity and specificity for the detection of pneumothorax in acute care settings. These findings are consistent with previous systematic reviews showing superior sensitivity of ultrasound compared with supine chest radiography, while maintaining high specificity [8-10].
Diagnostic performance varied depending on clinical context and reference standard. Sensitivity may be lower in cohorts that include CT-detected occult pneumothoraces or patients with small pneumothoraces, whereas performance is higher for clinically significant cases [3,9,11]. Operator experience and structured training play a key role in diagnostic accuracy, particularly in recognising dynamic sonographic signs such as lung sliding and the lung point [13,14].
Thoracic POCUS is especially valuable in prehospital, aeromedical, and retrieval environments, where rapid decision-making is required, and access to radiography is limited [15-22,26]. Multiple studies demonstrate that diagnostic lung ultrasound can be feasibly performed during transport and may influence early management decisions.
Recent emergency department-based studies and aeromedical evaluations further support the feasibility and diagnostic utility of thoracic POCUS across diverse acute care environments, reinforcing its applicability beyond controlled trauma settings [23,24].
Limitations
This review is limited by heterogeneity in study design, patient populations, ultrasound protocols, and reference standards. Some included studies had small sample sizes or limited pneumothorax events, reducing statistical precision. Differences in equipment and operator training may also affect diagnostic performance.
Conclusions
Thoracic POCUS demonstrates high sensitivity and specificity for the detection of pneumothorax in emergency and acute care settings. It enables rapid bedside assessment, supports early clinical decision-making, and may reduce reliance on delayed imaging modalities. Standardised scanning protocols and structured training are essential to optimise diagnostic performance, particularly in prehospital and retrieval environments.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Point-of-care ultrasonography N Engl J Med Díaz-Gómez JL Mayo PH Koenig SJ 1593160238520213467004510.1056/NEJ Mra 1916062 · doi ↗ · pubmed ↗
- 2Role of point-of-care ultrasound in critical care and emergency medicine: update and future perspective Clin Exp Emerg Med Choi W Cho YS Ha YR 3633811020233822577810.15441/ceem.23.101PMC 10790072 · doi ↗ · pubmed ↗
- 3Emergency department accuracy of point-of-care ultrasound in identifying clinically significant pneumothorax in high-severity trauma patients J Emerg Med Singer DD Scott H Khan A 1401517720254091387510.1016/j.jemermed.2025.07.009 · doi ↗ · pubmed ↗
- 4Point-of-care ultrasound-history, current and evolving clinical concepts in emergency medicine Medicina (Kaunas) Osterwalder J Polyzogopoulou E Hoffmann B 21795920233813828210.3390/medicina 59122179 PMC 10744481 · doi ↗ · pubmed ↗
- 5Advanced trauma life support (ATLS®): the ninth edition J Trauma Acute Care Surg ATLS Subcommittee; American College of Surgeons’ Committee on Trauma; International ATLS Working Group 13631366742013 https://doi.org/10.1097/TA.0b 013e 31828 b 82f 52360929110.1097/TA.0b 013e 31828 b 82f 5 · doi ↗ · pubmed ↗
- 6Point of care ultrasound: lung and diaphragm Best Pract Res Clin Anaesthesiol Yeşil BB Hogg RMG 296308392025
- 7Computed tomography in secondary spontaneous pneumothorax: reading the fine print Lung India Singh S Bhalla AS Naranje P Mohan A 319324392022 https://doi.org/10.4103/lungindia.lungindia_282_213584866210.4103/lungindia.lungindia_282_21PMC 9390294 · doi ↗ · pubmed ↗
- 8Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department Cochrane Database Syst Rev Chan KK Joo DA Mc Rae AD Takwoingi Y Premji ZA Lang E Wakai A 07202010.1002/14651858.CD 013031.pub 2PMC 739033032702777 · doi ↗ · pubmed ↗