PIK3CA-Mutant Non-Small Cell Lung Cancer Refractory to Two Lines of Chemoimmunotherapy: A Case Report
Takayuki Higashi, Tomoyuki Araya, Toshiyuki Kita, Ryo Hara, Hazuki Takato

TL;DR
A case report shows that PIK3CA-mutant non-small cell lung cancer may not respond well to standard chemoimmunotherapy treatments.
Contribution
This case highlights the poor response of isolated PIK3CA-mutant NSCLC to chemoimmunotherapy and suggests a need for PI3K-targeted therapies.
Findings
The patient with PIK3CA E545K mutation had rapid disease progression despite two lines of chemoimmunotherapy.
PIK3CA-mutant NSCLC may be refractory to conventional treatments including CTLA-4 inhibitors.
The case underscores the need for developing PI3K-targeted therapies for better outcomes.
Abstract
PIK3CA mutations play a critical role in tumorigenesis by driving constitutive activation of the phosphoinositide 3-kinase (PI3K) signaling pathway. These mutations have been identified in a small subset of non-small cell lung cancer (NSCLC), but their clinical significance and response to chemoimmunotherapy remain unclear. A 44-year-old man with a 24-pack-year smoking history presented with hoarseness and exertional dyspnea. Imaging demonstrated an irregular left upper-lobe pulmonary nodule consistent with the primary lesion, along with metastatic involvement of the left frontal lobe, cervical-mediastinal lymph nodes, right kidney, and lumbar vertebrae. Endobronchial ultrasound-guided transbronchial needle aspiration of the station 4R lymph node confirmed adenosquamous carcinoma. Molecular analysis revealed a PIK3CA E545K mutation without coexisting oncogenic driver alterations. The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
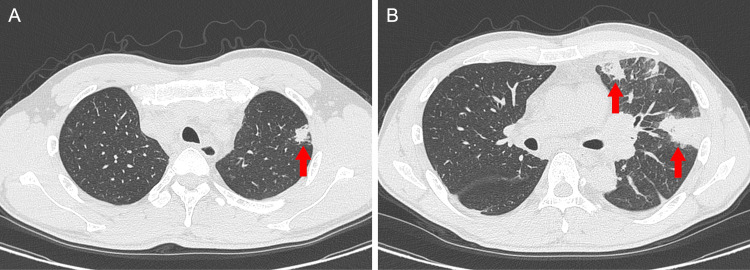 Figure 1
Figure 1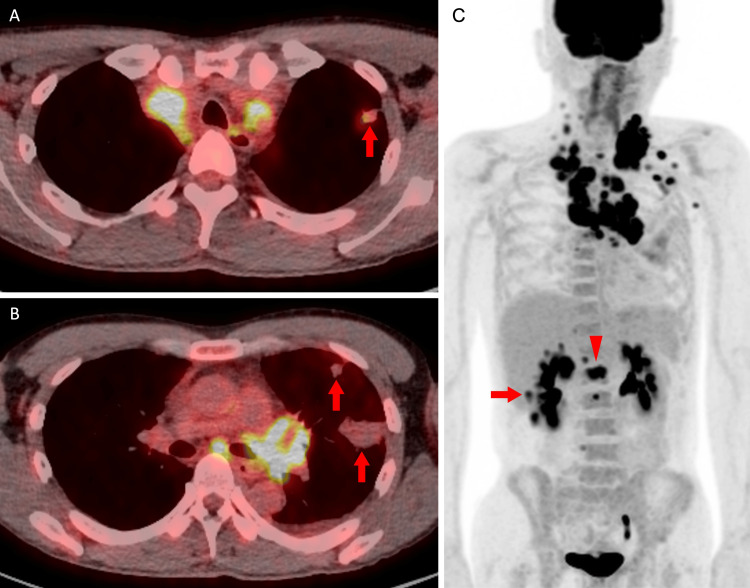 Figure 2
Figure 2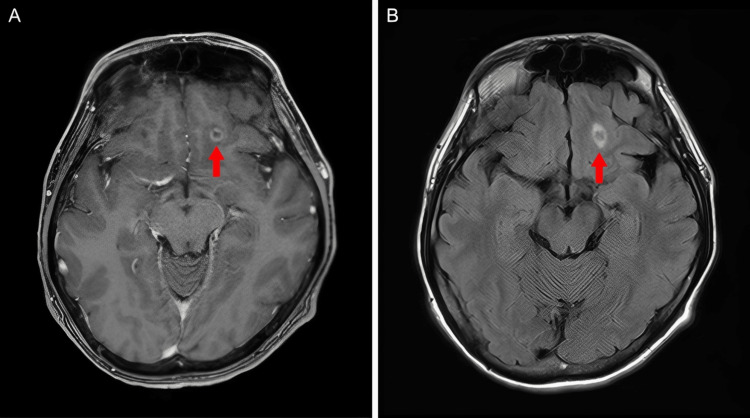 Figure 3
Figure 3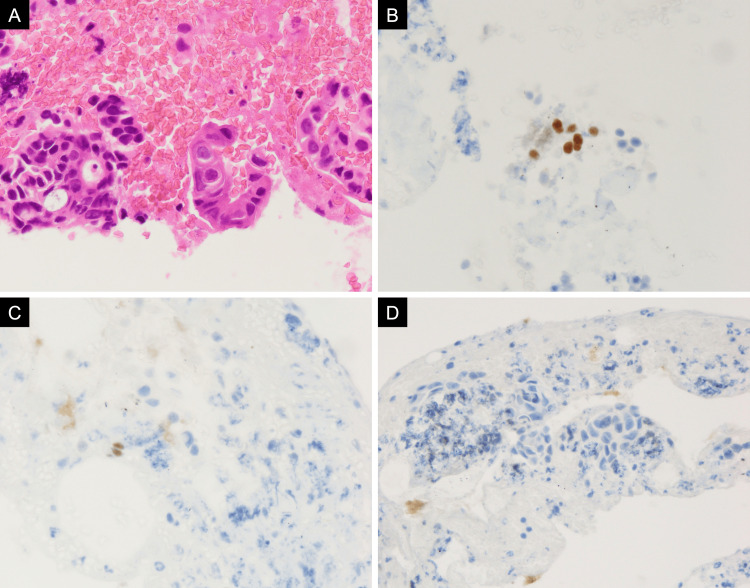 Figure 4
Figure 4| Parameter (unit) | Value | Reference range |
| WBC (/μL) | 12,000 | 4,500-9,000 |
| Neu (%) | 76.4 | 38-74 |
| Lym (%) | 13.1 | 16.5-49.5 |
| Mon (%) | 9.6 | 5-10 |
| Eos (%) | 0.7 | 0-10 |
| Bas (%) | 0.2 | 0-2 |
| RBC (×10⁴/μL) | 476 | 382-500 |
| Hb (g/dL) | 14.7 | 11.7-14.6 |
| Ht (%) | 43.9 | 34.3-44.2 |
| Plt (×10⁴/μL) | 12.1 | 15.8-34.8 |
| CRP (mg/dL) | 11.81 | 0-0.4 |
| T-Bil (mg/dL) | 0.8 | 0.3-1.2 |
| TP (g/dL) | 7.3 | 6.7-8.3 |
| ALP (U/L) | 332 | 38-113 |
| AST (U/L) | 15 | 13-33 |
| ALT (U/L) | 12 | 6-27 |
| LDH (U/L) | 238 | 119-229 |
| Alb (g/dL) | 3.4 | 4.0-5.0 |
| Na (mEq/L) | 137 | 135-149 |
| K (mEq/L) | 4.3 | 3.5-4.9 |
| Cl (mEq/L) | 98 | 96-108 |
| BUN (mg/dL) | 7.6 | 8-22 |
| Cr (mg/dL) | 0.61 | 0.5-0.8 |
| eGFR (mL/min/L) | 112.5 | 60-100 |
| UA (mg/dL) | 4.3 | 2.3-7.0 |
| D-dimer (μg/mL) | 1.9 | 0-1 |
| CEA (ng/mL) | 54.2 | 0-5 |
| CYFRA (ng/mL) | 7 | 0-3.5 |
| ProGRP (pg/mL) | 36.2 | 0-81 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPI3K/AKT/mTOR signaling in cancer · Lung Cancer Treatments and Mutations · Chronic Lymphocytic Leukemia Research
Introduction
Lung cancer remains one of the most frequently diagnosed malignancies worldwide [1]. Although targeted therapies and immunotherapy have dramatically improved survival, certain subsets of patients still experience poor outcomes due to a lack of established standard treatments [2].
Phosphoinositide 3-kinases (PI3Ks) are a family of lipid kinases that phosphorylate intracellular phosphoinositides, thereby regulating key cellular processes such as proliferation, survival, and metabolism [3,4]. PI3Ks are classified into three major classes, such as class I, class II, and class III, based on their structural and functional characteristics [3,4]. Class I PI3Ks are obligate heterodimers and are subdivided into two subclasses, class IA and class IB [3,4]. Class IA PI3Ks consist of one of the catalytic subunits, p110α, p110β, or p110δ, in complex with a p85-type regulatory subunit and are activated primarily by receptor tyrosine kinases [3,4]. By contrast, class IB PI3Ks consist of the p110γ catalytic subunit in complex with either the p101 or p84/p87 regulatory subunit and are activated by G-protein-coupled receptors [3,4].
Among the catalytic isoforms, p110α, encoded by PIK3CA, is the most frequently mutated and plays a critical role in tumorigenesis [4]. *PIK3CA *mutations occur predominantly at E542K and E545K in exon 9 and at H1047R in exon 20, resulting in constitutive activation of the PI3K signaling pathway [4,5]. These mutations are detected in approximately 2-5% of non-small cell lung cancers (NSCLCs) and have been associated with poor prognosis [6-9].
PI3K-targeted therapies, such as alpelisib, have demonstrated clinical benefit in PIK3CA-mutant breast cancer and have been approved by the US Food and Drug Administration [10]. However, their efficacy in NSCLC has not been established. Furthermore, the therapeutic outcomes of conventional chemotherapy and chemoimmunotherapy in PIK3CA-mutant NSCLC remain poorly understood. We report a case of PIK3CA-mutant NSCLC that was refractory to two different regimens of chemoimmunotherapy, ultimately resulting in rapid disease progression and death within four months of diagnosis.
This article was previously presented as a meeting abstract at the 2025 Annual Meeting of the Japan Lung Cancer Society on November 6, 2025.
Case presentation
A 44-year-old man presented with a one-month history of hoarseness and exertional dyspnea. He had no significant past medical history. His family history was notable for breast cancer in his sister and malignant lymphoma in his grandmother. He had a 24-pack-year smoking history and worked as a plasterer. Physical examination revealed multiple firm, immobile lymph nodes in the left cervical region, and his vital signs were stable.
Laboratory findings showed a white blood cell count of 12,000/μL, a C-reactive protein level of 11.81 mg/dL, and elevated serum tumor markers, including carcinoembryonic antigen at 54.2 ng/mL and cytokeratin 19 fragment at 7.0 ng/mL (Table 1).
Cervical and chest CT demonstrated an irregular nodule in the left upper lobe and multiple enlarged lymph nodes extending from the cervical to the mediastinal regions. Additionally, multiple wedge-shaped opacities were observed in the left lung parenchyma (Figure 1). 18F-fluorodeoxyglucose (FDG) PET/CT revealed intense FDG uptake in the enlarged lymph nodes and moderate uptake in the pulmonary nodule, right kidney, and lumbar vertebrae. In contrast, the wedge-shaped opacities in the left lung showed no abnormal FDG accumulation (Figure 2). Contrast-enhanced brain magnetic resonance imaging demonstrated a ring-enhancing lesion in the left frontal lobe (Figure 3).
CT findingsChest CT shows an irregularly shaped nodule in the left upper lobe (A, arrow), accompanied by multiple wedge-shaped opacities in the left lung parenchyma (B, arrows).
18F-FDG PET/CT findings18F-FDG PET/CT shows intense FDG uptake in the enlarged lymph nodes (A-C) and moderate uptake in the pulmonary nodule (A, arrow), right kidney (C, arrow), and lumbar vertebrae (C, arrowhead), while no abnormal FDG accumulation is observed in the wedge-shaped opacities in the left lung (B, arrows).FDG: fluorodeoxyglucose
MRI findingsContrast-enhanced T1-weighted imaging demonstrated a ring-enhancing lesion in the left frontal lobe (A, arrow). FLAIR imaging showed perilesional edema associated with the lesion (B, arrow).FLAIR: fluid-attenuated inversion recovery
Endobronchial ultrasound-guided transbronchial needle aspiration of the station 4R lymph node confirmed adenosquamous carcinoma. Immunohistochemical staining showed focal positivity for thyroid transcription factor-1, p40, and cytokeratin 5/6, and negativity for Napsin A, consistent with adenosquamous differentiation (Figure 4). The Oncomine Dx Target Test identified a *PIK3CA *E545K mutation, whereas no alterations were detected in EGFR, BRAF, HER2 (ERBB2), ALK, ROS1, MET, or RET. The cobas^®^ EGFR Mutation Test v2 was also negative. The programmed cell death ligand 1 tumor proportion score indicated low expression (1-9%). Tumor mutational burden and microsatellite instability were not assessed.
Pathological findings of the station 4R lymph nodeHematoxylin and eosin staining revealed both glandular formation and keratinization (A, ×600). Immunohistochemistry showed focal positivity for p40 (B, ×600) and thyroid transcription factor-1 (C, ×600) and negativity for Napsin A (D, ×400).
The left lung nodule was considered the primary lesion, whereas the lesions in the brain, lymph nodes, bones, and kidney were consistent with metastatic disease. The clinical stage was cT2N3M1c, corresponding to stage IVB. Tracheal stenosis and bilateral recurrent laryngeal nerve palsy, attributed to tumor invasion and compression, were noted. Additionally, the wedge-shaped opacities in the left lung were interpreted as pulmonary infarction. The patient’s Eastern Cooperative Oncology Group performance status (ECOG PS) was 1.
Because no approved PI3K-targeted therapy for NSCLC was available and no applicable clinical trial could be identified, PI3K inhibitors were not administered. First-line treatment with carboplatin, nab-paclitaxel, and pembrolizumab was initiated. However, disease progression occurred after two cycles, with the emergence of a new right adrenal metastasis and enlargement of preexisting lymph node lesions. Given the patient’s young age, stable ECOG PS of 1, and limited exposure to first-line therapy, a multidisciplinary team conference recommended an immune checkpoint inhibitor (ICI)-containing second-line regimen. Accordingly, treatment with carboplatin, pemetrexed, nivolumab, and ipilimumab, a cytotoxic T-lymphocyte-associated antigen 4 (CTLA-4) inhibitor, was initiated. However, airway obstruction continued to worsen, and the patient’s ECOG PS declined to 3 after the first cycle. Therefore, the best supportive care was selected, and palliative radiotherapy (30 Gy in 10 fractions) to the neck and mediastinum was administered, leading to transient symptomatic improvement. Nevertheless, the patient died two months later, approximately four months after the initial diagnosis.
Discussion
This case highlights that PIK3CA-mutant NSCLC can be refractory to both ICIs and cytotoxic chemotherapy. Notably, our patient was a young male smoker with adenosquamous carcinoma who exhibited rapid progression of lymph node disease.
The disease progressed rapidly despite two platinum-based chemoimmunotherapy regimens, including one incorporating a CTLA-4 inhibitor. Previous studies have suggested that *PIK3CA *mutations promote immune evasion by remodeling the tumor microenvironment into an immunosuppressive state through activation of the PI3K signaling pathway, which recruits myeloid-derived suppressor cells and suppresses cytotoxic CD8+ T-cell activity. This mechanism attenuates antitumor immunity and renders tumors refractory to ICIs [11]. In addition, PIK3CA-mutant cancers, such as breast and colorectal cancers, have been shown to be refractory to cytotoxic chemotherapy [12,13]. A similar tendency may be observed in PIK3CA-mutant NSCLC, although clinical evidence remains limited.
Previous studies have indicated that PIK3CA-mutant NSCLC is more likely to present with lymph node involvement, suggesting that activation of the PI3K signaling pathway may promote lymphatic invasion and metastatic potential of tumor cells [9,14].
PIK3CA mutations frequently coexist with other canonical oncogenic driver alterations, such as EGFR or *KRAS *[8,15]. In contrast, our patient harbored an isolated activating *PIK3CA *E545K mutation without concurrent oncogenic driver alterations. In a retrospective cohort of PIK3CA-mutant advanced NSCLC, isolated *PIK3CA *mutations were reported to occur more frequently in older patients with squamous histology, and the median overall survival was 12 months [16]. By comparison, our patient was relatively young, had adenosquamous carcinoma, and died approximately four months after diagnosis. This atypical case expands the clinical spectrum of isolated PIK3CA-mutant NSCLC. Several studies have reported that isolated PIK3CA-mutant NSCLC exhibits a poorer prognosis than cases with co-occurring oncogenic driver alterations [14,15]. This unfavorable outcome may be explained by the lack of effective standard treatment options for NSCLC harboring isolated PIK3CA mutations, whereas NSCLC with other oncogenic driver alterations may benefit from targeted therapy [15].
Although no standard targeted therapy has been established for isolated PIK3CA-mutant NSCLC, emerging evidence suggests that PI3K-targeted therapies may have activity in a specific molecular subset [16]. In other PIK3CA-mutant malignancies, PI3K inhibitors have demonstrated clinical benefit [10], and preclinical studies provide further rationale for a range of PI3K-targeted approaches. For example, bladder cancer models have shown that combined PI3K inhibition and immune checkpoint blockade creates an immunostimulatory tumor microenvironment and produces strong synergistic antitumor effects [17]. Additionally, endometrial and breast cancer models have shown that multi-node inhibition targeting PI3K and downstream signaling components achieves more complete pathway suppression than single-node inhibition [18]. Collectively, these findings suggest that PI3K-targeted therapies warrant further clinical evaluation as potential treatment options for PIK3CA-mutant NSCLC.
Conclusions
This case highlights that isolated PIK3CA-mutant NSCLC may be refractory to conventional chemoimmunotherapy, including regimens incorporating a CTLA-4 inhibitor. Further clinical investigation of PI3K-targeted therapies, ideally in prospective basket or umbrella trials and in larger real-world cohorts, is warranted to establish effective treatment strategies for PIK3CA-mutant NSCLC.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer statistics, 2025 CA Cancer J Clin Siegel RL Kratzer TB Giaquinto AN Sung H Jemal A 10457520253981767910.3322/caac.21871 PMC 11745215 · doi ↗ · pubmed ↗
- 2The effect of advances in lung-cancer treatment on population mortality N Engl J Med Howlader N Forjaz G Mooradian MJ 64064938320203278618910.1056/NEJ Moa 1916623 PMC 8577315 · doi ↗ · pubmed ↗
- 3Phosphatidylinositol 3-kinase, growth disorders, and cancer N Engl J Med Goncalves MD Hopkins BD Cantley LC 2052206237920183046294310.1056/NEJ Mra 1704560 · doi ↗ · pubmed ↗
- 4PI 3K isoforms in cell signalling and vesicle trafficking Nat Rev Mol Cell Biol Bilanges B Posor Y Vanhaesebroeck B 5155342020193111030210.1038/s 41580-019-0129-z · doi ↗ · pubmed ↗
- 5The structure of a human p 110α/p 85α complex elucidates the effects of oncogenic PI 3Kα mutations Science Huang CH Mandelker D Schmidt-Kittler O 1744174831820071807939410.1126/science.1150799 · doi ↗ · pubmed ↗
- 6Coexistence of EGFR with KRAS, or BRAF, or PIK 3CA somatic mutations in lung cancer: a comprehensive mutation profiling from 5125 Chinese cohorts Br J Cancer Li S Li L Zhu Y 2812282011020142474370410.1038/bjc.2014.210PMC 4037826 · doi ↗ · pubmed ↗
- 7Landscape of phosphatidylinositol-3-kinase pathway alterations across 19 784 diverse solid tumors JAMA Oncol Millis SZ Ikeda S Reddy S Gatalica Z Kurzrock R 15651573220162738858510.1001/jamaoncol.2016.0891 · doi ↗ · pubmed ↗
- 8Coexistence of PIK 3CA and other oncogene mutations in lung adenocarcinoma-rationale for comprehensive mutation profiling Mol Cancer Ther Chaft JE Arcila ME Paik PK 4854911120122213523110.1158/1535-7163.MCT-11-0692 PMC 3593239 · doi ↗ · pubmed ↗