Complex Hypertrophic Scar and Ventral Hernia Formation Following Laparoscopic Cholecystectomy: A Case Report
Shashawna S Drum Christie, Trevor Williams, Sabitra Niroula, Bom K Bong, Akwasi Berko, Ka Wai Wu, Frederick Tiesenga

TL;DR
A man developed a severe scar and hernia after a routine surgery, showing how wound healing can go wrong and the challenges in treating it.
Contribution
This case highlights the complex relationship between wound healing, mechanical stress, and scar formation after laparoscopic surgery.
Findings
The patient developed a symptomatic hypertrophic scar and incisional hernia after laparoscopic cholecystectomy.
Surgical excision and corticosteroid injection provided only partial relief, with recurrence of scarring.
Histopathology confirmed dense collagen deposition, consistent with hypertrophic scar formation.
Abstract
Hypertrophic scars are fibroproliferative lesions that form at the site of a wound due to excessive collagen deposition during the healing process. These scars remain confined to the original wound boundaries and may improve over time. Their formation is a complex process influenced by multiple factors, including wound depth and location, tension on the healing skin, genetic predisposition, and the inflammatory response. Abnormal regulation of fibroblasts and prolonged inflammation lead to excessive deposition of type III collagen (the final tensile collagen), resulting in a thickened, raised scar. Mechanical stress at the wound site, such as in areas of frequent movement (e.g., the abdomen), may also contribute to the development of exaggerated scarring. Additionally, delayed wound healing or infection, as seen in some postoperative cases, increases the risk of hypertrophic scar…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1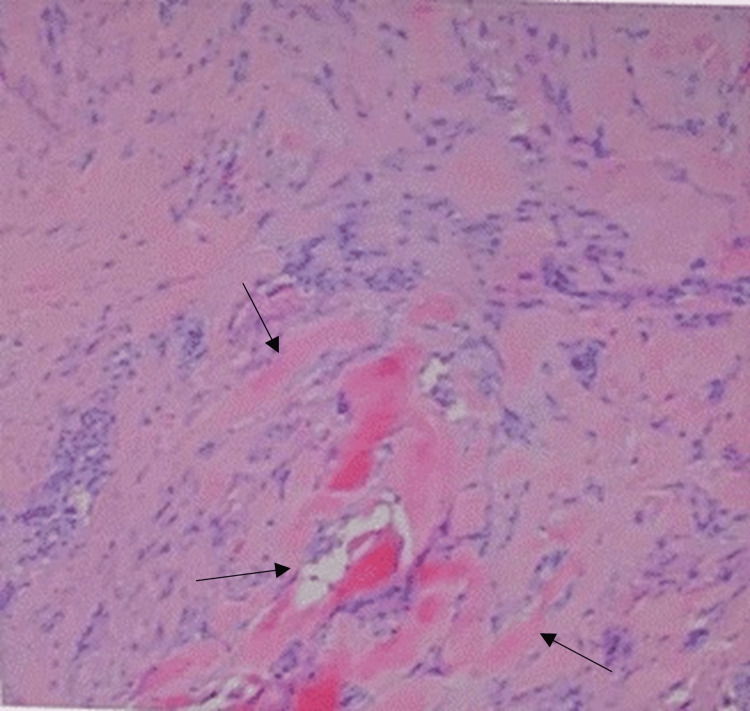 Figure 2
Figure 2 Figure 3
Figure 3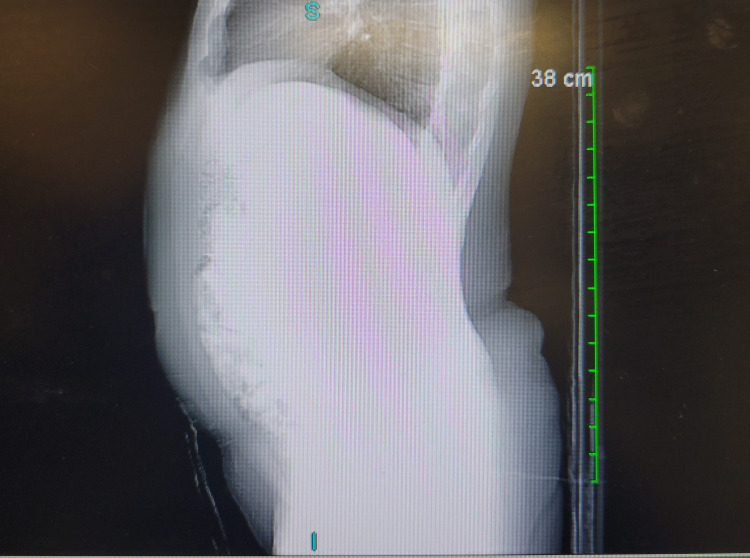 Figure 4
Figure 4| Test | Patient’s value | Reference range |
| Glucose (mg/dL) | 106 | 70-99 |
| Blood urea nitrogen (mg/dL) | 16 | 7-25 |
| Creatinine (mg/dL) | 0.72 | 0.6-1.30 |
| Sodium (mmol/L) | 138 | 133-144 |
| Potassium (mmol/L) | 4.2 | 3.5-5.1 |
| Chloride (mmol/L) | 103 | 98-109 |
| Carbon dioxide (mmol/L) | 30 | 21-31 |
| Anion gap (mmol/L) | 5 | 3.6-11.0 |
| Blood urea nitrogen/creatinine ratio | 22 | 6.0-20.0 |
| Calcium (mg/dL) | 9.9 | 8.6-10.3 |
| Total protein (g/dL) | 7.3 | 6.4-8.9 |
| Albumin (g/dL) | 4.8 | 3.5-5.7 |
| Aspartate aminotransferase (U/L) | 11 | 13-39 |
| Alanine aminotransferase (U/L) | 21 | 7-52 |
| Alkaline phosphatase (U/L) | 64 | 40-129 |
| Total bilirubin (mg/dL) | 0.5 | 0.0-1.0 |
| Glomerular filtration rate (Modification of Diet in Renal Disease, non-African American) (mL/min/1.73 m²) | >60 | >60 |
| Glomerular filtration rate (Modification of Diet in Renal Disease, African American) (mL/min/1.73 m²) | >60 | >60 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatologic Treatments and Research · Surgical Sutures and Adhesives · Intestinal and Peritoneal Adhesions
Introduction
Hypertrophic scars represent abnormal wound-healing responses characterized by excessive collagen deposition, leading to raised, firm, and often symptomatic scars [1]. These lesions may develop after surgical trauma, postoperative infection, prolonged inflammation, or delayed wound healing and are often associated with pain, pruritus, and cosmetic concerns for patients. Hypertrophic scars occur in 39-68% of surgical wounds involving high-tension areas, with the abdomen representing a moderate-risk location due to frequent movement, increased dermal tension, and susceptibility to postoperative complications [1]. Postoperative complications, such as surgical site infection (SSI), have been shown to significantly increase the risk of abnormal scarring by disrupting normal granulation, impairing collagen organization, and prolonging inflammatory signaling [2]. Risk factors for poor wound healing include diabetes, obesity, stress, tobacco use, and malnutrition [2].
In addition to abnormal scar formation, impaired wound healing is a major risk factor for the development of incisional hernias, which occur in approximately 10-20% of abdominal surgeries, with even higher rates when infection is present. Mechanical tension, fascial dehiscence, and early collagen disarray weaken the integrity of the abdominal wall, thereby predisposing patients to herniation. Trocar-site hernias, although less common than midline incisional hernias, may occur at any laparoscopic port site, particularly those larger than 10 mm or those associated with postoperative infection or prolonged healing delay [3].
This case report describes the unusual presentation of a recurrent hypertrophic scar associated with an incisional hernia following laparoscopic cholecystectomy. Despite surgical revision, the patient continued to experience persistent pain, erythema, and thickening at the incision site, consistent with recurrent hypertrophic scarring. Partial symptomatic relief with topical Contractubex^®^ gel (heparin, allantoin, and onion extract) suggests that the irritation and tenderness were primarily related to ongoing abnormal scar tissue activity [4]. This case aims to highlight the interplay among postoperative infection, mechanical stress, and aberrant wound healing in the development of hypertrophic scars and incisional hernias following laparoscopic abdominal surgery.
Case presentation
A 46-year-old man presented with persistent pain, swelling, and redness localized to a previous laparoscopic cholecystectomy incision site in the epigastric region. The patient underwent laparoscopic cholecystectomy on January 2, 2024, at a tertiary hospital for symptomatic acute calculous cholecystitis. The operation was challenging due to the presence of dense fibrotic tissue resulting from repeated inflammatory episodes. The gallbladder was removed laparoscopically after difficult dissection, during which bile spillage occurred, and the supraumbilical fascial incision required dilation to facilitate specimen extraction.
The immediate postoperative course was complicated by a superficial wound infection at the epigastric trocar site, manifesting as seropurulent drainage and localized tenderness. The infection was treated with oral cephalexin, which was discontinued due to an allergic rash. The wound subsequently healed by secondary intention. Although the infection resolved, the patient developed a progressively thickened, raised, erythematous scar that became tender and pruritic.
Over the following months, the patient noted progressive localized swelling and discomfort beneath the scar, described as a sensation of pressure and bulging (Figure 1). No inflammatory collection or mass was identified.
Clinical photograph of the patient’s postoperative epigastric incision site, demonstrating a linear, healed scar with focal areas of inflammationA central erythematous nodular elevation is visible along the scar line, consistent with localized inflammatory change. A small pustular focus is present just left of midline (blue arrow), representing superficial purulence within the scar tract. Surrounding the scar, there is mild diffuse erythema without induration or fluctuance. No active drainage is observed.
Persistent localized pain prompted further evaluation. Examination revealed a 1 × 1 cm incisional (ventral) hernia beneath a hypertrophic scar at the previous port site. Routine laboratory investigations demonstrated normal renal and hepatic function, normal albumin, and an elevated fasting glucose level consistent with prediabetes, which was managed non-pharmacologically. No recent HbA1c or inflammatory markers (CRP and ESR) were available. Laboratory findings are summarized in Table 1.
On February 13, 2025, the patient underwent open incisional hernia repair with excision of hypertrophic scar tissue and intralesional triamcinolone (Kenalog) injection at an outside hospital. Intraoperatively, a 1 × 1 cm fascial defect was identified beneath an area of dense fibrotic scar. The hernia sac and overlying hypertrophic scar were excised en bloc in an elliptical fashion. The fascial defect was closed with 0 Ethibond sutures, hemostasis was achieved, and the wound was closed in layers. Kenalog was injected into the wound bed to reduce the risk of recurrence. Estimated blood loss was minimal, and no complications occurred. A portion of the excised tissue was submitted for histopathologic evaluation.
The pathology report (GoPath Laboratories; collected: February 13, 2025; reported: February 17, 2025) described a 3.3 × 1.1 × 1.0 cm segment of tan skin with underlying soft tissue and a second smaller lobulated fragment. Microscopic examination revealed dense, haphazardly arranged eosinophilic collagen bundles with fibroblastic proliferation, consistent with a hypertrophic scar. No atypia or malignancy was identified. The final pathology diagnosis was benign hypertrophic scar, without evidence of malignancy (Figure 2).
Histopathologic section of the excised hypertrophic scarBlack arrows indicate dense eosinophilic collagen bundles within the dermis, accompanied by increased fibroblast proliferation (H&E stain, ×10). These findings are characteristic of hypertrophic scar architecture and confirm the absence of malignancy.
At postoperative follow-up, the patient reported partial improvement in pressure and bulging but persistent localized scar pain, irritation, and redness. He denied drainage, fever, or features suggestive of recurrent hernia. The discomfort was described as a burning and pulling sensation, worsened by touch. On examination, the epigastric incision measured approximately 4 cm and appeared raised, firm, and erythematous with localized tenderness (Figure 3). The patient reported partial improvement in irritation and pruritus with the use of Contractubex^®^ gel (heparin, allantoin, and onion extract), applied twice daily.
Clinical photograph of the epigastric incision site demonstrating a raised, firm, erythematous scar with localized thickening and irregular surface texture measuring approximately 4 cm at postoperative follow-upThe scar corresponds to the prior laparoscopic port site and remains symptomatic with tenderness and pruritus.
On physical examination, the epigastric incision appeared elevated, firm, erythematous, and mildly tender, without fluctuance, warmth, drainage, or palpable hernia recurrence. The abdomen was soft and non-distended.
A postoperative CT of the abdomen without contrast, performed on June 27, 2025, demonstrated an unremarkable abdomen, with no free air, fluid collection, lymphadenopathy, or bowel obstruction. The liver, spleen, pancreas, adrenals, kidneys, and aorta were unremarkable. No seroma, abscess, or recurrent hernia was identified. These findings confirmed stable postoperative anatomy and an intact fascial repair (Figure 4).
Sagittal CT image of the upper abdomen (non-contrast) obtained on June 27, 2025, demonstrating an intact fascial repair without evidence of recurrent hernia, seroma, abscess, or postoperative fluid collectionPartially visualized bowel loops are not dilated. No acute intra-abdominal pathology is identified.
Given the chronicity of symptoms, postoperative imaging findings, and confirmed histopathology, the patient was diagnosed with recurrent symptomatic hypertrophic scar following open incisional hernia repair. He was advised to continue conservative topical scar therapy, with consideration of serial intralesional corticosteroid injections, silicone sheeting, and dermatologic referral for adjunctive therapies.
Discussion
Hypertrophic scars are characterized by excessive collagen deposition during wound repair and remain confined to the original wound boundaries, distinguishing them from keloid scars, which extend beyond the wound margins. Their pathogenesis involves abnormal, dysregulated fibroblast activity, prolonged inflammation, and excessive production of the extracellular matrix. These processes are often triggered by factors such as wound depth, delayed healing, location, mechanical tension, infection, and genetic predisposition [5,6]. In this patient, abdominal wound tension following laparoscopic cholecystectomy, combined with a documented postoperative superficial infection, created an environment conducive to hypertrophic scar formation and subsequent incisional hernia development.
Incisional hernia is a recognized complication after abdominal surgery due to disruption of the fascia, with risk factors including advanced age, obesity, diabetes, SSI, and trocar size. SSIs significantly increase the risk of hernia development, as confirmed by meta-analyses, because they impair collagen remodeling and increase fascial dehiscence. Although most trocar-related hernias occur at the umbilical port site, this patient’s postoperative infection and delayed healing became the locus of hernia formation, likely due to a combination of tissue tension, repeated inflammation, and scarring [6,7].
Management of hypertrophic scars is multimodal due to their high recurrence rate after treatment. First-line therapies include tension reduction, silicone gel sheeting, and intralesional corticosteroid injections. Triamcinolone acetonide (TAC) demonstrates the highest efficacy among corticosteroids for scar reduction [4,8]. Corticosteroid injections reduce hypertrophic scar formation by downregulating pro-inflammatory cytokines and growth factors, such as TGF-β, which decreases fibroblast activity and extracellular matrix deposition. These injections ultimately reduce scar thickness and volume, as well as pruritus and pain [4,8]. Limiting factors for corticosteroid treatment include variable efficacy, a high recurrence rate, and steroid resistance, often requiring multiple dermatology clinic visits, which can be challenging for patients in resource-limited settings [8]. Pressure therapy and topical agents may provide symptomatic relief, but evidence for their effectiveness is variable.
Surgical revision is reserved for refractory cases and should be combined with adjuvant therapies to minimize recurrence risk. Evidence shows that the lowest recurrence rates are achieved with multimodal therapy combining surgery plus radiation and/or TAC [7]. This approach targets multiple aspects of hypertrophic scar pathophysiology: surgery removes the bulk of the scar, while radiation and TAC suppress fibroblast proliferation and collagen synthesis, preventing abnormal wound healing and reducing recurrence.
The patient’s allergic reaction to cephalexin, a commonly prescribed beta-lactam antibiotic for skin and soft-tissue infections, is consistent with known IgE-mediated hypersensitivity and necessitated immediate discontinuation [9]. Symptomatic improvement with topical Contractubex^®^, a formulation containing heparin, allantoin, and onion extract, aligns with experimental evidence showing improved wound architecture and reduced scar thickness in animal models [4].
This case suggests a multifactorial contribution to hypertrophic scar recurrence, including postoperative infection, delayed wound healing, mechanical tension, and prior scar pathology. These factors interact to produce persistent symptoms. Evidence-based management requires early intervention, multimodal therapy, and individualized follow-up to optimize outcomes [4-6,7]. However, interpretation of these findings should consider the report’s limitations, including its single-patient design, which restricts generalizability and precludes causal inference, and the relatively limited duration of postoperative follow-up, which limits assessment of long-term recurrence risk and durability of treatment outcomes.
Conclusions
This case illustrates the potential contributions of postoperative infection, delayed wound healing, and mechanical stress to the development of hypertrophic scarring and subsequent incisional hernia formation. The patient’s clinical course highlights the challenges of managing postoperative hypertrophic scars, particularly when infectious complications exacerbate fibroproliferative responses and compromise fascial integrity. Conservative measures, including topical scar therapy (e.g., Contractubex^®^) and tension reduction, remain foundational components of a multimodal treatment approach. However, adjunctive interventions such as intralesional corticosteroid injections, laser therapy, or combination modalities may be required for sustained symptom control in more severe or recurrent cases. Although limited by the inherent constraints of a single case, this report emphasizes the importance of early recognition of postoperative wound complications and timely implementation of multimodal scar management strategies to mitigate recurrence and potentially reduce postoperative complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Hypertrophic scarring keloids Stat Pearls [Internet] Carswell L Borger J Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/30725743/30725743 · pubmed ↗
- 2Impaired wound healing Stat Pearls [Internet] Wernick B Nahirniak P Stawicki SP Treasure Island (FL)Stat Pearls Publishing 2025 https://pubmed.ncbi.nlm.nih.gov/29489281/29489281 · pubmed ↗
- 3Trocar site post incisional hernia: about 19 cases Pan Afr Med J Nacef K Chaouch MA Chaouch A Khalifa MB Ghannouchi M Boudokhane M 1832920183006196110.11604/pamj.2018.29.183.14467 PMC 6061823 · doi ↗ · pubmed ↗
- 4Pharmacotherapy for keloids and hypertrophic scars Int J Mol Sci Murakami T Shigeki S 46742520243873189310.3390/ijms 25094674 PMC 11083137 · doi ↗ · pubmed ↗
- 5The most current algorithms for the treatment and prevention of hypertrophic scars and keloids: a 2020 update of the algorithms published 10 years ago Plast Reconstr Surg Ogawa R 7994149202210.1097/PRS.0000000000008667 PMC 868761834813576 · doi ↗ · pubmed ↗
- 6An abnormality in glucocorticoid receptor expression differentiates steroid responders from nonresponders in keloid disease Br J Dermatol Rutkowski D Syed F Matthews LC Ray DW Mc Grouther DA Watson RE Bayat A 69070017320152571214310.1111/bjd.13752 PMC 4744777 · doi ↗ · pubmed ↗
- 7Update on hypertrophic scar treatment Clinics (Sao Paulo) Rabello FB Souza CD Farina Júnior JA 5655736920142514111710.6061/clinics/2014(08)11PMC 4129552 · doi ↗ · pubmed ↗
- 8Minimal-invasive technologies for treatment of hts and keloids: corticosteroids Textbook on Scar Management Lee J Kim J Cham Springer 202036351132 · pubmed ↗