Isolated right ventricular löffler endocarditis secondary to allergic bronchopulmonary aspergillosis
Rikako Horie, Yasuhisa Nakao, Kenta Horie, Osamu Yamaguchi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
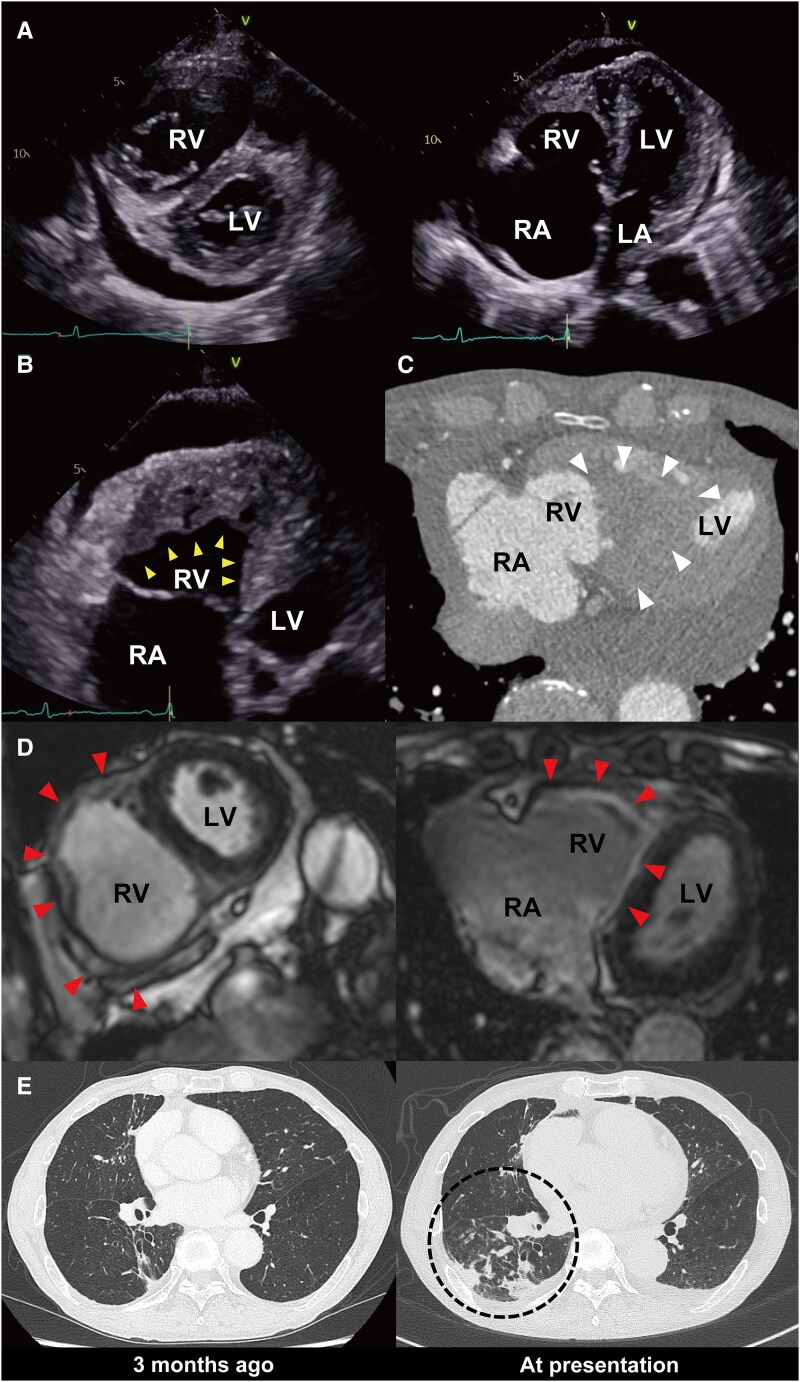 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Infective Endocarditis Diagnosis and Management · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
A 74-year-old man with a history of chronic productive cough presented with rapidly progressive bilateral leg oedema over one month. Transthoracic echocardiography showed preserved left ventricular systolic function, enlargement of the right atrium and ventricle (Panel A), reduced right ventricular wall motion, and an isoechoic mass at the right ventricular apex (yellow arrowheads in Panel B). Cardiac computed tomography confirmed an apical thrombus (white arrowheads in Panel C), and cardiac magnetic resonance imaging demonstrated delayed enhancement of the right ventricular free wall, predominantly in the endocardial to mid-myocardial layers (red arrowheads in Panel D). Laboratory tests revealed persistent eosinophilia (1000–1500/μL) over the previous five years, and bone marrow examination excluded idiopathic hypereosinophilic syndrome. Chest computed tomography showed a progressive right lower-lobe infiltrate (Panel E, black circle), and bronchoscopy revealed a mucus plug. Aspergillus-specific IgG and IgE antibodies were positive, establishing allergic bronchopulmonary aspergillosis (ABPA) as the underlying cause of secondary eosinophilia. Anticoagulation and corticosteroid therapy led to marked thrombus reduction, normalization of eosinophil counts, and resolution of respiratory and heart failure symptoms.
This case highlights that ABPA-related eosinophilia can cause Löffler endocarditis confined to the right ventricle. In contrast to idiopathic hypereosinophilic syndrome—typically associated with aggressive inflammation, biventricular myocardial damage, and extensive intracardiac thrombi—secondary eosinophilia may progress more slowly and be diagnosed while still limited to the right ventricle.^1–3^ Clinicians should maintain a high index of suspicion for intracardiac thrombus in patients with ABPA, as early identification and appropriate therapy may prevent life-threatening cardiac complications.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ommen SR, Seward JB, Tajik AJ. Clinical and echocardiographic features of hypereosinophilic syndromes. Am J Cardiol 2000;86:110–113.10867107 10.1016/s 0002-9149(00)00841-9 · doi ↗ · pubmed ↗
- 2Rhyou HI, Lee SE, Kim MY, Park CS, Jo EJ, Choi GS, et al Idiopathic hypereosinophilia: a multicenter retrospective study. J Asthma Allergy 2022;15:1763–1771.36531904 10.2147/JAA.S 388341 PMC 9749411 · doi ↗ · pubmed ↗
- 3Agarwal R, Khan A, Aggarwal AN, Varma N, Garg M, Saikia B, et al Clinical relevance of peripheral blood eosinophil count in allergic bronchopulmonary aspergillosis. J Infect Public Health 2011;4:235–243.22118718 10.1016/j.jiph.2011.08.006 · doi ↗ · pubmed ↗