Comparative efficacy and safety of mesalazine-based regimens with traditional Chinese medicines in mild-to-moderate ulcerative colitis
Bin Huang, Honglin An, Liming Chen, Huimin Lin, Huaping Wu, Ruofei Li, Yaping Su, Jiumao Lin, Dan Shi

TL;DR
Combining mesalazine with certain traditional Chinese medicines improves ulcerative colitis symptoms and gut health without increasing side effects.
Contribution
A network meta-analysis comparing eight TCM formulations combined with mesalazine for ulcerative colitis, identifying optimal combinations for specific outcomes.
Findings
CurQD and Kangfuxin showed the highest probabilities of improving symptoms in ulcerative colitis.
Glycyrrhizae decoction and Baitouweng decoction provided the greatest reduction in Mayo scores.
Scutellaria granules most effectively reduced inflammatory cytokines like IL-6 and TNF-α.
Abstract
Traditional Chinese medicine (TCM) formulations are increasingly used in combination with mesalazine to treat mild-to-moderate active ulcerative colitis (UC). However, direct comparisons between various TCM regimens are limited. We performed a frequentist network meta-analysis of 34 randomized controlled trials (n = 2,854) comparing oral mesalazine (1.0–4.0 g/day) alone versus mesalazine plus one of eight TCM formulations: Kangfuxin solution, Shaoyao decoction, Glycyrrhizae decoction, Scutellaria decoction (Huangqin granules), Baitouweng decoction (Pulsatilla; retention enema), Shenling Baizhu Powder, CurQD formula, or Fufangkushen capsules. Outcomes included clinical efficacy, adverse events, Mayo score, serum interleukin-6 (IL-6) and tumor necrosis factor-α (TNF-α), and intestinal Bifidobacteria, Lactobacilli, and Escherichia coli. Risk ratios (RRs) were calculated for dichotomous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
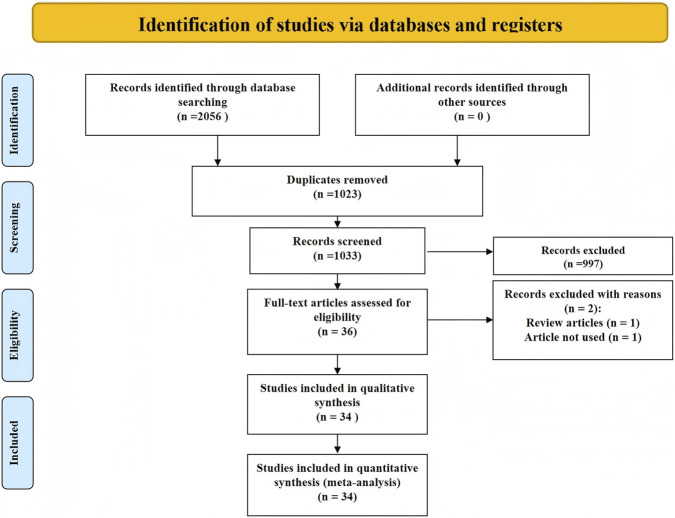 FIGURE 1
FIGURE 1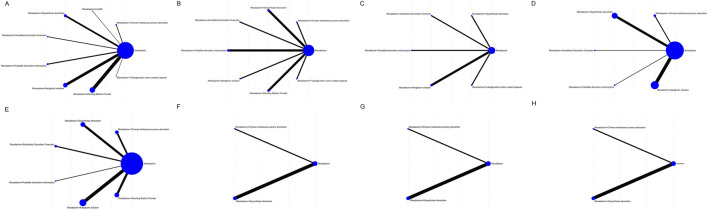 FIGURE 2
FIGURE 2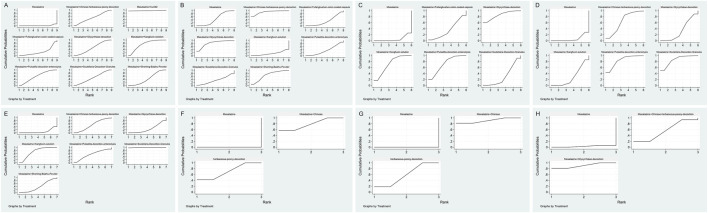 FIGURE 3
FIGURE 3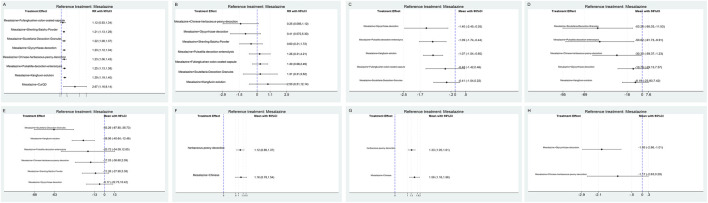 FIGURE 4
FIGURE 4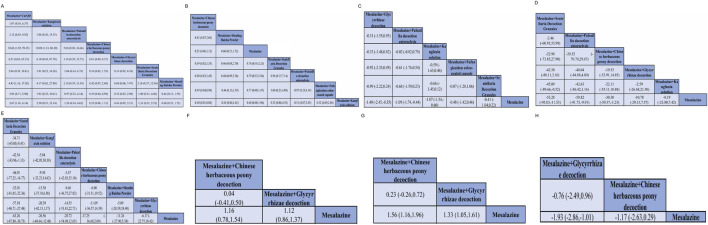 FIGURE 5
FIGURE 5| No. | Author (year) | Study design, region | Sample of study | Age | Sex (M/F) | Interventions | Severity of ulcerative colitis | Duration (Weeks) | Outcomes | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Control group | Experimental group | Control group | Experimental group | Control group | Experimental group | |||||||
| 1 | Chen Jianlin (2018) | RCTs, China | 72 | 37.9 ± 8.66 | 38.5 ± 8.78 | 21/15 | 20/16 | Mesalazine enteric-coated tablets, 0.5 g per dose, three times daily, orally | On the basis of oral mesalazine enteric-coated tablet treatment, shaoyao decoction retention enema was additionally administered | In the treatment group, there were 16 cases of mild, 18 moderate, and 2 severe ulcerative colitis. In the control group, there were 18 mild, 17 moderate, and 1 severe case | 3 weeks | Overall clinical efficacy, serum inflammatory factor levels, intestinal microbiota levels |
| 2 | Liu Yanhong (2019) | RCTs, China | 81 | 39.46 ± 6.38 | 40.15 ± 5.27 | 23/17 | 24/17 | Mesalazine enteric-coated tablets (NMPA H19980148), oral administration: 0.5 g (2 tablets) per dose, 3 times daily | Mesalazine enteric-coated tablets combined with modified shaoyao decoction retention enema therapy | The disease duration in the control group was 2–4 years (3.17 ± 1.02), and in the treatment group was 2–5 years (3.46 ± 1.33) | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 3 | Kong Haiying (2025) | RCTs, China | 100 | 45.79 ± 14.16 | 46.12 ± 13.43 | 26/24 | 31/19 | Treated with oral mesalazine enteric-coated tablets (0.25 g; heilongjiang tianhong pharmaceutical co., ltd.; national drug approval no. H20103359), one tablet three times daily for 12 weeks | Treated with shaoyao decoction combined with mesalazine | Patients had active mild to moderate UC | 12 weeks | Serum inflammatory factor levels, adverse events |
| 4 | Shomron Ben-Horin (2024) | RCTs, Israel | 41 | 25 (23–30) | 35 (23–48) | 5/8 | 15/13 | Received identical-looking mesalazine capsules daily for 8 weeks | Received CurQD: 3 capsules of 500 mg herbal extract and 3 capsules of 500 mg curcumin daily (total 3 g/day) for 8 weeks | Patients had active mild to moderate UC: SCCAI>5, Mayo>2, inflammation>15 cm from rectum | 8 weeks | Overall clinical efficacy |
| 5 | Zheng Lianlian (2015) | RCTs, China | 86 | 42.3 ± 5.2 | 41.7 ± 4.9 | 23/20 | 25/18 | Mesalazine enteric-coated tablets were given | Mesalazine enteric-coated tablets combined with licorice xiexin decoction were given | Diagnosed per the 2007 national IBD consensus with endoscopic and pathological confirmation; condition is mild to moderate | 6 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 6 | Shen Lingna (2021) | RCTs, China | 60 | 47.00 ± 10.28 | 47.67 ± 10.83 | 15/15 | 16/14 | Oral mesalazine enteric-coated tablets, 4 times/day, 4 tablets per dose (1 g total) | Same mesalazine regimen plus glycyrrhizae decoction (twice daily) | In the traditional Chinese medicine group: 13 cases were mild, 17 were moderate; In the control group: 14 cases were mild, 16 were moderate | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels, intestinal microbiota levels, mayo score |
| 7 | Hu Lu (2025) | RCTs, China | 50 | 42.33 ± 3.68 | 42.36 ± 3.64 | 11/14 | 13/12 | Treated with mesalazine (national drug approval no. H19980148, 0.25 g × 24 tablets), 4 tablets per dose, 3 times per day | Mesalazine enteric-coated tablets combined with licorice xiexin decoction were given | Patients had active mild to moderate UC | NR. | Overall clinical efficacy, serum inflammatory factor levels |
| 8 | Li Yan (2024) | RCTs, China | 70 | 45.01 ± 1.61 | 44.50 ± 1.15 | 20/15 | 18/17 | Received oral mesalazine enteric-coated tablets (0.25 g, 1.0 g per dose, 3 times/day; H20103359, tianhong pharma) | Mesalazine enteric-coated tablets combined with licorice xiexin decoction were given | Disease severity in the control group: 19 mild cases, 16 moderate; in the experimental group: 21 mild, 14 moderate | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels, intestinal microbiota levels, adverse events |
| 9 | Feng Yongbo (2023) | RCTs, China | 82 | 39.36 ± 6.25 | 40.11 ± 6.20 | 25/16 | 23/18 | Received mesalazine enteric-coated tablets (0.25 g/tablet, 1 g per dose, before meals, 3×/day; H19980148, sunflower pharma) | Mesalazine enteric-coated tablets combined with licorice xiexin decoction were given | Disease duration in the control group ranged from 0.5 to 12 years, with a mean of 5.89 ± 2.11 years; in the experimental group, duration ranged from 1 to 11 years, with a mean of 6.02 ± 1.98 years | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels, intestinal microbiota levels |
| 10 | Ding Hairong (2018) | RCTs, China | 126 | 42.4 ± 8.7 | 43.5 ± 9.6 | 32/31 | 35/28 | Mesalazine granules (Les laboratoires ethypharm, France; batch no. 160117), 1 g per dose, three times daily | Received mesalazine combined with huangqin decoction granules | In the treatment group: 18 mild cases, 35 moderate, 10 severe; In the control group: 21 mild cases, 34 moderate, 8 severe | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels, mayo score |
| 11 | Wang Haiyang (2024) | RCTs, China | 95 | 49.52 ± 7.13 | 50.36 ± 7.82 | 27/20 | 29/19 | Received probiotics plus mesalazine: Bifidobacterium tablets (1.5 g, 3×/day) and mesalazine (1.0 g, 4×/day) for 1 month | Received the same treatment plus huangqin decoction enema | In the control group, there were 26 mild cases and 21 moderate cases of inflammation; in the study group, there were 25 mild cases and 23 moderate cases | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels, adverse events |
| 12 | Chen Qilong (2019) | RCTs, China | 110 | 20∼60 | 20∼60 | 30/25 | 28/27 | Received oral mesalazine alone (500 mg per dose, three times per day) | Treated with oral mesalazine (500 mg per dose, three times per day) combined with retention enema administration of baitouweng decoction | Patients had active mild to moderate UC | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 13 | Xu Jiaping (2019) | RCTs, China | 124 | 56.1 ± 7.5 | 56.3 ± 6.8 | 30/32 | 31/31 | Received oral mesalazine (produced by harbin zhenikang pharmaceutical co., ltd., brand name: Huidi) | Treated with mesalazine combined with baitouweng decoction administered via enema | In the control group, there were 38 mild cases and 24 moderate cases; in the experimental group, there were 40 mild cases and 22 moderate cases | 4 weeks | Overall clinical efficacy, adverse events, mayo score |
| 14 | Yang Jingnan (2015) | RCTs, China | 46 | 44.26 ± 12.79 | 45.83 ± 14.13 | 11/12 | 12/11 | Mesalazine (500 mg per dose, three times daily) was produced by sunflower pharmaceutical group jiamusi luling co., ltd | Treated with mesalazine combined with baitouweng decoction administered via enema | Patients had active mild to moderate UC | 4 weeks | Overall clinical efficacy |
| 15 | Chen Min (2022) | RCTs, China | 80 | 40.33 ± 2.64 | 39.97 ± 2.47 | 22/18 | 23/17 | Received oral mesalazine (1 g, three times daily; sunflower pharma, H19980148) | Received mesalazine and kangfuxin solution (50 mL; good doctor panxi, Z51021834) | The disease duration was 3 months–6 years (2.65 ± 0.63 years) in the control group and 2 months to 5 years (2.59 ± 0.61 years) in the observation group | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 16 | Zhu Qiang (2022) | RCTs, China | 46 | 45.61 ± 3.61 | 46.02 ± 3.65 | 13/10 | 12/11 | Received 1 g mesalazine enteric-coated tablets (0.25 g/tablet, 3 times daily) | Received mesalazine and enema treatment with kangfuxin solution (10 mL/bottle) | The disease duration ranged from 1 to 10 years, averaging 5.96 ± 1.05 years in the control group and 6.02 ± 1.08 years in the experimental group | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels, mayo score |
| 17 | Chen Hui (2022) | RCTs, China | 60 | 35.78 ± 3.14 | 36.74 ± 3.16 | 17/13 | 14/16 | Received oral mesalazine enteric-coated tablets (0.25 g/tablet, 1 g per dose, three times daily) | Received mesalazine treatment plus enema with kangfuxin solution (20 mL/bottle) | The disease duration was 1–4 years (2.76 ± 0.11 years) in the control group and 2–5 years (2.79 ± 0.12 years) in the experimental group | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 18 | Liu Lina (2022) | RCTs, China | 86 | 47.27 ± 4.27 | 48.24 ± 4.84 | 23/20 | 21/22 | Received oral mesalazine (2 g per dose, twice daily) for 2 months | Received mesalazine treatment plus retention enema with kangfuxin solution | Patients had active mild to moderate UC | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 19 | Xu Ruosi (2022) | RCTs, China | 50 | 42.03 ± 5.18 | 41.53 ± 4.68 | 17/8 | 16/9 | Received mesalazine sustained-release granules (1.0 g per dose, taken with water every 6 h) | Received the same treatment plus mesalazine suppositories and kangfuxin solution retention enema | Observation group: 5 severe, 13 moderate, 7 mild cases; in the control group: 5 severe, 12 moderate, 8 mild cases | 4 weeks | Overall clinical efficacy, mayo score, serum inflammatory factor levels |
| 20 | Liu Lu (2024) | RCTs, China | 80 | 51.23 ± 11.78 | 51.31 ± 12.05 | 20/20 | 21/19 | Received oral mesalazine enteric-coated tablets (1 g per dose, three times daily) for 4 weeks | Received mesalazine treatment plus kangfuxin solution retention enema | Disease duration in the observation group ranged from 7 months to 7 years, with a mean of 3.68 ± 2.77 years; in the control group, it ranged from 6 months to 8 years, with a mean of 3.89 ± 2.98 years | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels, adverse events |
| 21 | Wang Xudong (2025) | RCTs, China | 80 | 45.21 ± 11.69 | 45.60 ± 11.87 | 22/18 | 23/17 | Treated with oral mesalazine enteric-coated tablets (1 g per dose, three times daily) for 4 weeks | Received mesalazine treatment plus retention enema with kangfuxin solution (30 mL kangfuxin +100 mL saline) | Patients had active mild to moderate UC | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels, adverse events |
| 22 | Liu Yang (2022) | RCTs, China | 50 | 40.24 ± 3.26 | 40.30 ± 3.22 | 13/12 | 12/13 | Received oral mesalazine (1.0 g per dose, three times daily) | Received mesalazine treatment plus kangfuxin solution enema | The disease duration was 2 months–5 years (2.63 ± 0.47 years) in the control group and 4 months to 6 years (2.60 ± 0.43 years) in the observation group | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 23 | Meng Qinglei (2025) | RCTs, China | 78 | 38.97 ± 5.40 | 38.67 ± 5.52 | 22/17 | 21/18 | Received oral mesalazine enteric-coated tablets (0.25 g/tablet, 1.0 g per dose, four times daily) for 4 weeks | Received mesalazine treatment plus kangfuxin solution enema (50 mL) | The disease duration was 3 months to 3 years (1.68 ± 0.52 years) in the observation group and 5 months to 3 years (1.64 ± 0.55 years) in the control group | 4 weeks | Overall clinical efficacy, serum inflammatory factor levels, adverse events |
| 24 | Yang Ying (2018) | RCTs, China | 86 | 37. 85 ± 7. 06 | 38. 25 ± 7. 36 | 25/18 | 26/17 | Received oral mesalazine (0.25 g/tablet, 1 g per dose, four times daily) | Received mesalazine treatment plus oral shenling baizhu powder (6 g per dose, three times daily) | The observation group had a disease duration of 3 months–5 years (mean 8.26 ± 1.25 months); the control group, 4 months to 6 years (mean 8.64 ± 1.74 months) | 12 weeks | Overall clinical efficacy, serum inflammatory factor levels, adverse events |
| 25 | Dong Zenghui (2018) | RCTs, China | 86 | 46.5 ± 1.5 | 45.5 ± 2.5 | 20/23 | 21/22 | Received mesalazine alone (1 g, four times daily) for 12 weeks | Received shenling baizhu powder (6 g, three times daily) plus mesalazine (1 g, three times daily) for 12 weeks with dietary restrictions | Treatment group: disease duration 2–6 weeks, mean 3.5 ± 0.5 weeks; Control group: 1–7 weeks, mean 3.5 ± 0.5 weeks | 12 weeks | Overall clinical efficacy, adverse events |
| 26 | Li Limei (2021) | RCTs, China | 90 | 46.50 ± 7.87 | 47.33 ± 8.52 | 25/20 | 26/19 | Received mesalazine (0.25 g/tablet, dongsheng pharmaceutical co., ltd., approval no. H20020211) at 0.5 g per dose, three times daily | Received mesalazine treatment plus shenling baizhu powder | Observation group: disease duration 8 months to 20 years (mean 9.04 ± 3.24 years); Control group: 6 months to 20 years (mean 8.81 ± 2.15 years) | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 27 | Li Kui (2015) | RCTs, China | 73 | 39.5 ± 8.2 | 40.8 ± 7.6 | 23/14 | 21/15 | Received oral mesalazine (1.0 g per dose, four times daily; provided by sunflower pharmaceutical group jiamusi luling pharmaceutical co., ltd., approval no. H19980148) | Received mesalazine treatment plus oral shenling baizhu powder (6.0 g per dose, three times daily; provided by Beijing Tongrentang pharmaceutical co., ltd., approval no. Z11020947) | The observation group had a disease duration of 4 months–9 years (mean 9.1 ± 2.7 months); the control group, 5 months to 9 years (mean 9.6 ± 3.1 months) | 8 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 28 | Wei Guoli (2013) | RCTs, China | 46 | 18∼58 | 18∼60 | 13/10 | 16/7 | Received oral mesalazine, 1.0 g per dose, four times daily | Received the same treatment plus shenling baizhu powder (composed of ginseng, atractylodes, yam, coix seed, etc.), 6.0 g per dose, three times daily | Patients had active mild to moderate UC | 12 weeks | Overall clinical efficacy, serum inflammatory factor levels |
| 29 | Chen Hong (2014) | RCTs, China | 80 | 39.2 ± 7.6 | 41.7 ± 8.1 | 25/15 | 26/14 | Received oral mesalazine enteric-coated tablets (shire, Germany; reg. No. H20030501), 1,000 mg, three times daily | Received mesalazine treatment plus retention enema with shenling baizhu powder (Z51020828, chengdu jiuzhitang jinding pharmaceutical co., ltd.) | The treatment group had a disease duration of 8 months–20 years (mean 8.9 ± 2.4 years); the control group, 10 months to 21 years (mean 9.0 ± 2.6 years) | 4 weeks | Overall clinical efficacy |
| 30 | He Kuisheng (2014) | RCTs, China | 48 | 37.76 ± 7.12 | 39.36 ± 6.23 | 15/9 | 16/8 | Mesalazine (0.25 g/tablet, 1 g per dose, four times daily; sunflower pharmaceutical group jiamusi luling pharmaceutical co., ltd., approval no. H19980148) | Mesalazine and shenling baizhu powder (6 g per dose, three times daily; chongqing greenforest pharmaceutical co., ltd., approval no. Z20053891) | Patients had active mild to moderate UC | 13 weeks | Overall clinical efficacy |
| 31 | Chen Guozhen (2013) | RCTs, China | 96 | 41.7 ± 8.1 | 38.2 ± 7.6 | 24/24 | 24/24 | Treated with mesalazine (Les laboratoires servier, France; H19980149, 10 sachets/box), 1 g per dose, four times daily | Received combined treatment with shenling baizhu powder (3 g/sachet; shaanxi panlong pharmaceutical group co., ltd., Z22021157) and mesalazine | The treatment group had a disease duration of 10 months–18 years (mean 10.2 ± 2.4 years); the control group, 1–20 years (mean 11.0 ± 2.6 years) | 8 weeks | Overall clinical efficacy |
| 32 | Huang Xiangchun (2016) | RCTs, China | 100 | 42.5 ± 8.5 | 41.5 ± 8.4 | 33/17 | 35/15 | Treated with mesalazine (1.0 g per dose, four times daily, orally) for 12 weeks, using mesalazine from heilongjiang tianhong pharmaceutical co., ltd. (approval no. H20103359) | Received the same mesalazine treatment plus shenling baizhu powder | Patients had active mild to moderate UC | 12 weeks | Overall clinical efficacy |
| 33 | Zhang Aiqing (2019) | RCTs, China | 82 | 39.1 ± 6.4 | 38.9 ± 6.2 | 26/16 | 18/22 | Treated with mesalazine enteric-coated tablets (0.5 g per dose, three times daily, taken 30 min after meals; jiamusi luling pharmaceutical co., H19980148) | Received combined treatment with shenling baizhu powder and mesalazine, using the same dosage and administration | The observation group had a disease duration of 1–8 years (mean 4.6 ± 2.5 years); the control group, 1–7 years (mean 4.4 ± 2.3 years) | NR. | Overall clinical efficacy |
| 34 | Yang Gong (2012) | RCTs, China | 314 | 44.51 ± 12.02 | 43.63 ± 12.01 | 42/38 | 123/111 | Received mesalazine enteric-coated tablets (4 tablets, 4 times/day) + FCC placebo (4 capsules, 3 times/day) | Received fufangkushen colon-coated capsules (4 capsules, 3 times/day) + mesalazine placebo (4 tablets, 4 times/day) | Disease duration: FCC group: 2.99 ± 3.56 years; HD group: 2.39 ± 3.89 years; baseline mayo score: FCC group: 7.86 ± 1.59; HD group: 7.95 ± 1.29 | 8 weeks | Overall clinical efficacy, adverse events, mayo score |
| TCM formulation | Key bioactive constituents | Proposed mechanisms of action |
|---|---|---|
| CurQD | Curcumin, quercetin, resveratrol | NF-κB inhibition, anti-inflammatory, antioxidant, immunomodulation |
| Kangfuxin solution | Polypeptides, nucleotides, glycopeptides | Mucosal repair, epithelial proliferation, angiogenesis, intestinal barrier support |
| Shaoyao decoction | Paeoniflorin, glycyrrhizin | Anti-inflammatory, immune modulation, gut microbiota regulation |
| Glycyrrhizae decoction | Glycyrrhizin, berberine, flavonoids | Anti-inflammatory, gut microbiota modulation, mucosal protection |
| Scutellaria decoction | Baicalin, baicalein, scutellarin | NF-κB inhibition, anti-inflammatory, cytokine regulation (TNF-α, IL-6) |
| Baitouweng decoction | Berberine, paeoniflorin, flavonoids | Anti-inflammatory, antimicrobial ( |
| Shenling baizhu powder | Polysaccharides, saponins | Gut barrier repair, immune modulation, anti-inflammatory |
| Fufangkushen capsules | Alkaloids, flavonoids | Anti-inflammatory, immunomodulation, antioxidant properties |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInflammatory Bowel Disease · Pharmacological Effects of Natural Compounds · Flavonoids in Medical Research
Introduction
Ulcerative colitis (UC) is a chronic, relapsing inflammatory bowel disease characterized by diffuse mucosal inflammation confined to the colon and rectum (Pang, 2023; Yang et al., 2023). Its incidence and prevalence have steadily increased worldwide over the past 2 decades, including in traditionally low-incidence regions such as East Asia (Levine et al., 2020). The disease imposes a substantial burden on patients, with symptoms such as persistent diarrhea, abdominal pain, rectal bleeding, and fatigue contributing to impaired quality of life, reduced work productivity, and psychological distress (Wakai et al., 2020). UC is associated with long-term risks including colorectal dysplasia and cancer, particularly in patients with prolonged disease duration and extensive colonic involvement (Wan et al., 2021; Yue et al., 2025). Mesalazine (5-aminosalicylic acid) remains the cornerstone of pharmacologic therapy for mild-to-moderate UC, particularly in inducing and maintaining remission (Lima et al., 2022). However, despite its widespread use and established anti-inflammatory effects, the therapeutic response to mesalazine varies considerably among patients. Issues such as incomplete symptom resolution, frequent relapse, suboptimal adherence due to dosing frequency or gastrointestinal side effects, and concerns over nephrotoxicity in long-term use highlight the limitations of monotherapy (Martí-Aguado et al., 2021; Lu et al., 2024). These shortcomings necessitate adjunctive strategies to enhance treatment outcomes and reduce drug burden.
Traditional Chinese medicine (TCM) has been increasingly integrated into UC management, particularly in East Asia, owing to its multi-targeted effects on immune modulation, inflammation control, and mucosal repair. Several TCM formulations have demonstrated promising effects in alleviating UC symptoms, lowering systemic and local cytokine levels, and promoting intestinal microbiota balance in both clinical and preclinical studies. Given these potential benefits, there is growing interest in combining TCM with mesalazine to enhance therapeutic efficacy and safety in UC patients (Kou et al., 2020; Shen et al., 2021). Over the past decade, an increasing number of randomized controlled trials (RCTs) have investigated the efficacy of various TCM formulations combined with mesalazine in the treatment of UC. Combinations such as Kangfuxin solution, Shaoyao Decoction, Glycyrrhizae decoction, and Baitouweng Decoction with mesalazine have shown favorable outcomes in improving clinical remission rates, reducing inflammatory cytokines (e.g., IL-6, TNF-α), and modulating gut microbiota (Chen, 2018; Kong et al., 2025). These findings suggest that TCM may provide an effective adjunct to standard mesalazine therapy (Yang et al., 2023; Zhang et al., 2022).
However, most of the existing evidence comes from small-scale two-arm RCTs with varied diagnostic criteria, outcome measures, and sample sizes. Head-to-head comparisons of different TCM–mesalazine combinations are scarce, and long-term outcomes or adverse event profiles are often underreported. Such methodological inconsistencies limit the generalizability and interpretability of these findings, hindering the evidence-based integration of TCM into standardized UC management. To date, no comprehensive network meta-analysis has systematically compared the efficacy and safety of various TCM formulations in combination with mesalazine, leaving a critical gap in the selection of optimal treatment strategies for integrative care.
Despite the potential benefits of TCM in the treatment of UC, there is a lack of systematic comparative studies to determine which TCM formulations work best in combination with mesalazine. Therefore, this study aims to perform a network meta-analysis to compare the efficacy and safety of different TCM–mesalazine combinations. In response to this gap, we conducted a frequentist network meta-analysis that included 34 RCTs evaluating eight TCM–mesalazine combinations for active mild-to-moderate UC. This analysis allowed both direct and indirect comparisons, enabling us to rank the interventions based on their efficacy and safety using surface under the cumulative ranking curve (SUCRA) probabilities. We specifically selected TCM formulations that (i) had randomized trials directly comparing “TCM + mesalazine” versus “mesalazine alone,” ensuring a connected network for quantitative synthesis; (ii) represent complementary pharmacological actions relevant to UC, such as NF-κB–mediated cytokine suppression (e.g., Scutellaria granules, CurQD), mucosal healing (e.g., Kangfuxin), microbiota and barrier modulation (e.g., Shaoyao and Glycyrrhizae decoctions), topical therapy for distal disease (Baitouweng retention enema), and broad immune support (Shenling Baizhu Powder); (iii) are available as fixed-composition, clinically used preparations (decoctions/granules/capsules/liquids) to ensure reproducibility; and (iv) can be co-administered with mesalazine in routine care. The final set of TCM formulations included Kangfuxin solution, Shaoyao decoction, Glycyrrhizae (Gancao Xiexin) decoction, Scutellaria (Huangqin) granules/decoction, Baitouweng decoction (retention enema), Shenling Baizhu Powder, CurQD, and Fufangkushen capsules. Although CurQD and Fufangkushen were each represented by a single RCT, they were retained due to their clinical relevance, and sensitivity analyses were conducted to assess the robustness of the rankings excluding single-trial interventions. This study provides a comprehensive, quantitative synthesis of the efficacy and safety of TCM–mesalazine combinations, offering valuable insights for individualized UC treatment strategies.
Methods
Literature search strategy
We performed a comprehensive literature search across five major databases: PubMed, China National Knowledge Infrastructure (CNKI), Wanfang Data, VIP Database, and SinoMed. The search spanned from database inception to July 2025. Both Medical Subject Headings (MeSH) and free-text keywords were used in combination to maximize sensitivity and specificity. English search terms included UC, mesalazine, TCM, Shaoyao decoction, Kangfuxin solution, and randomized controlled trial. Equivalent Chinese terms were applied to Chinese-language databases to capture regionally published trials. Boolean operators (AND, OR) were used to structure the queries. No restrictions were applied to publication language; however, only studies published in English or Chinese were eligible. Reference lists of all included articles and relevant reviews were also manually screened to identify additional studies missed by the electronic search.
Eligibility criteria
Studies were included if they met all of the following criteria:
- Study design: Randomized controlled trials (RCTs), regardless of blinding or allocation concealment status.
- Population: Patients with a confirmed diagnosis of active mild-to-moderate UC, based on established clinical, endoscopic, and/or histopathological criteria.
- Intervention: The experimental group received a single TCM formula—either a classical decoction or Chinese patent medicine—administered orally or via enema, in combination with oral mesalazine. The control group received oral mesalazine monotherapy.
- Outcomes: Studies were required to report at least one of the following outcomes: overall clinical efficacy rate, Mayo score, levels of inflammatory cytokines (IL-6, TNF-α), intestinal microbiota indices (e.g., Bifidobacteria, Lactobacilli, Escherichia coli), or incidence of adverse events.
Studies were excluded if they met any of the following conditions:
- Use of more than one TCM formulation, or concurrent use of non-pharmacologic traditional therapies such as acupuncture or moxibustion in the experimental group.
- Non-randomized trials, quasi-experimental studies, or trials with major methodological flaws.
- Incomplete or irretrievable outcome data, or studies that failed to report extractable quantitative results.
- Duplicate publications or abstracts without corresponding full texts.
Data extraction
Data from eligible studies were independently extracted by two reviewers using a pre-defined standardized data collection form. Extracted information included: first author, year of publication, country or region where the study was conducted, sample size in each group, baseline characteristics of participants (mean age, sex distribution), details of interventions (name and dosage of the TCM formulation, mesalazine regimen, route of administration), treatment duration, and all reported outcome measures. These included both primary outcomes (e.g., clinical efficacy rate, Mayo score) and secondary outcomes (e.g., serum or mucosal levels of IL-6, TNF-α; intestinal microbiota changes; adverse event rates). Any discrepancies between the two reviewers were resolved by discussion, and if consensus could not be reached, a third reviewer was consulted to adjudicate.
Risk of bias assessment
The methodological quality of the included randomized controlled trials was evaluated using the Cochrane Risk of Bias Tool (RoB 2.0). This tool assesses seven domains: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) completeness of outcome data, (6) selective outcome reporting, and (7) other potential sources of bias (Jang et al., 2021). Assessments were visualized using RevMan 5.4.
Statistical analysis
All statistical analyses were performed using Stata (StataCorp, College Station, TX, United States). For dichotomous outcomes, effect sizes were calculated as risk ratio (RR) with 95% confidence intervals (CIs). For continuous outcomes, mean difference (MD) with 95% CIs. We conducted a frequentist random-effects network meta-analysis (NMA) integrating direct and indirect comparisons. Surface under the cumulative ranking curve (SUCRA) values were calculated; higher SUCRA indicates higher probability of being best.
Heterogeneity across studies was assessed using the I ^ 2 ^ statistic. To detect potential publication bias, comparison-adjusted funnel plots were visually inspected, and asymmetry was formally tested using Egger’s regression. Inconsistency between direct and indirect evidence was evaluated using the node-splitting method when closed loops were present in the treatment network. A p-value <0.05 was considered statistically significant for all analyses.
Results
Study selection and characteristics
A total of 2,056 records were identified. After removing 1,023 duplicates, 1,033 titles/abstracts were screened and 36 full texts were assessed. Two full texts were excluded (one review; one not meeting eligibility), leaving 34 RCTs for the network meta-analysis (Chen, 2018; Kong et al., 2025; Liu, 2019; Ben-Horin et al., 2024; Zheng et al., 2015; Shen, 2021; Li et al., 2024; Feng, 2023; Ding et al., 2018; Wang and Zhang, 2024; Chen et al., 2019; Jia-Ping and Chao-Qun, 2019; Yang and Wang, 2015; Chen, 2022; Zhu and Ji, 2022; Shan and Chen, 2022; Liu L., 2022; Xu et al., 2022; Liu Y., 2022; Yang and Yan, 2018; Dong, 2018; Li and Wang, 2021; Li, 2015; Wei, 2013; Chen, 2014; He, 2014; Chen et al., 2013; Huang, 2016; Zhang, 2019; Gong et al., 2012; Hu, 2025; Liu, 2024; Meng, 2025). The literature selection process is illustrated in Figure 1.
PRISMA flow diagram of study selection.
All trials were conducted in China except one multicenter RCT from Israel (CurQD). Sample sizes ranged from 41 to 314; mean ages ranged from approximately 20–56 years. Treatment duration was 3–12 weeks. Controls received oral mesalazine monotherapy (1.0–4.0 g/day). Experimental arms combined mesalazine with one TCM: Shaoyao decoction (n = 3), Glycyrrhizae decoction (n = 5), Scutellaria decoction (n = 2), Baitouweng decoction (n = 4; retention enema), Kangfuxin solution (n = 10), Shenling Baizhu Powder (n = 8), CurQD formula (n = 1), or Fufangkushen capsules (n = 1) (Table 1).
Network geometry, consistency, and bias assessment
Networks for all outcomes (Figures 2A–H) were well connected via mesalazine. Contribution plots indicated that comparisons involving Kangfuxin and Shaoyao contributed the largest information. Comparison-adjusted funnel plots showed no clear small-study effects; formal tests were not significant (all p > 0.05).
Network plots for eight TCM–mesalazine combinations and mesalazine monotherapy across study outcomes. A–H correspond to: (A) clinical efficacy, (B) adverse events, (C) Mayo score, (D) serum IL-6, (E) serum TNF-α, (F) intestinal Bifidobacteria, (G) intestinal Lactobacilli, and (H) intestinal Escherichia coli.
Clinical efficacy
The comparative efficacy rankings are summarized in Figure 3. Most mesalazine–TCM combinations achieved higher clinical efficacy than mesalazine alone (Figures 4A, 5A). CurQD and Kangfuxin ranked highest by SUCRA (96.7% and 72.7%); in the direct CurQD–mesalazine comparison the pooled effect was RR = 2.67 (95% CI 1.16–6.14; RR > 1 favors the combination). Kangfuxin showed consistent benefit across multiple trials (RR = 1.29, 95% CI 1.19–1.40).
SUCRA rankings of interventions for each outcome (A–H).
Forest plots of network estimates for each outcome. Data are presented as RRs with 95% CIs for dichotomous outcomes and MDs for continuous outcomes (A–H).
Rankograms for the probability distribution of each intervention’s ranking (A–H).
Safety profile
Adverse-event rates were similar across regimens (Figures 4B, 5B). Safety rankings favored Shaoyao (SUCRA 90.2%) and Glycyrrhizae (82.1%); no combination showed a statistically significant increase in adverse events.
Mayo score reduction
Six interventions reported Mayo score (Figures 4C, 5C). The greatest mean reductions were observed with Glycyrrhizae decoction (MD = −1.40, 95% CI −2.45 to −0.35), Baitouweng decoction via retention enema (MD = −1.09, 95% CI −1.74 to −0.44), and Kangfuxin solution (MD = −1.07, 95% CI −1.54 to −0.60). SUCRA rankings were consistent with these estimates.
Inflammatory cytokines
For IL-6 (Figure 4D), the largest decreases were with Scutellaria decoction (MD = −53.28 pg/mL, 95% CI −95.03 to −11.53) and Baitouweng decoction (MD = −50.82 pg/mL, 95% CI −91.73 to −9.91). For TNF-α (Figure 4E), Scutellaria decoction ranked highest (MD = −53.26 pg/mL, 95% CI −87.80 to −38.73), followed by Kangfuxin solution (MD = −26.56 pg/mL, 95% CI −40.64 to −12.48).
Intestinal microbiota
Microbiota outcomes were reported in fewer trials (Figures 4F–H, 5F–H).
Bifidobacteria increased with Shaoyao (MD = 1.12, 95% CI 0.86–1.37) and Glycyrrhizae (MD = 1.16, 95% CI 0.78–1.54).
Lactobacilli increased with Shaoyao (MD = 1.33, 95% CI 1.05–1.61) and Glycyrrhizae (MD = 1.56, 95% CI 1.16–1.96).
Escherichia coli decreased significantly with Glycyrrhizae (MD = −1.93, 95% CI −2.86 to −1.01); Shaoyao showed a non-significant trend toward reduction (MD = −1.17, 95% CI −2.63 to 0.29).
Overall, combinations most frequently appearing in the top-three rankings were: CurQD and Kangfuxin for clinical efficacy; Shaoyao and Glycyrrhizae for safety; Glycyrrhizae, Baitouweng, and Kangfuxin for Mayo score reduction; Scutellaria for IL-6 and TNF-α; and Shaoyao/Glycyrrhizae for microbiota modulation.
Sensitivity analysis for single-trial interventions
To assess the potential instability of the SUCRA rankings due to single-trial interventions (e.g., CurQD and Fufangkushen capsules), sensitivity analyses were performed by excluding these interventions and recalculating the rankings for the remaining treatments. The exclusion of CurQD and Fufangkushen capsules did not significantly alter the overall treatment rankings, suggesting that the top-ranked interventions (e.g., Kangfuxin, Shaoyao decoction) maintained their relative positions in the network. These results indicate that the overall rankings are robust, although caution is recommended when interpreting the rankings for single-trial interventions.
Adverse events
Adverse events were generally mild and infrequent across all treatment regimens. The most commonly reported adverse events were gastrointestinal discomfort, including symptoms such as bloating, nausea, and diarrhea. These occurred in approximately 10%–15% of patients receiving Kangfuxin solution and Shenling Baizhu Powder. Allergic reactions, such as skin rashes and pruritus, were reported in 2%–3% of patients treated with Fufangkushen capsules. Renal safety was closely monitored, and mild, transient increases in serum creatinine were observed in 1%–2% of patients receiving Kangfuxin solution and Shenling Baizhu Powder. However, these changes were not clinically significant.
The safety profiles of mesalazine–TCM combinations were generally favorable, with most adverse events being mild and self-limiting. Gastrointestinal discomfort was the most common side effect, particularly with Kangfuxin solution and Shenling Baizhu Powder, where 10%–15% of patients reported mild nausea and bloating. Allergic reactions, such as skin rashes and pruritus, were more frequently observed in patients receiving Fufangkushen capsules (2%–3%). Renal function was monitored throughout the study, with mild, transient elevations in serum creatinine noted in 1%–2% of patients treated with Kangfuxin solution and Shenling Baizhu Powder. These changes resolved with dose adjustments. Liver function tests revealed no significant hepatotoxicity, although mild elevations in liver enzymes were observed in some patients receiving Glycyrrhizae decoction.
Overall, the incidence of serious adverse events (SAEs) was low, and mesalazine–TCM combinations were well tolerated. However, individualized monitoring of gastrointestinal, renal, and hepatic function is recommended, particularly for patients with preexisting conditions or those requiring long-term therapy.
Discussion
This network meta-analysis synthesized evidence from 34 RCTs involving eight standardized TCM formulations combined with mesalazine versus mesalazine monotherapy for mild-to-moderate active UC. Most combinations improved clinical efficacy without increasing adverse events. CurQD formula and Kangfuxin solution ranked highest for clinical response, while Shaoyao decoction and Glycyrrhizae decoction ranked highest for safety. Glycyrrhizae decoction, Baitouweng decoction, and Kangfuxin solution were most effective for Mayo score reduction. Scutellaria decoction showed the greatest improvement in both IL-6 and TNF-α, followed by Kangfuxin for TNF-α. Shaoyao decoction and Glycyrrhizae decoction had the most favorable effects on gut microbiota, with Glycyrrhizae decoction uniquely reducing E. coli. These findings suggest that adding selected TCM formulations to mesalazine may provide additive or complementary benefits, and that the optimal choice may depend on the primary clinical goal—symptom remission, inflammation control, or microbiota modulation.
Comparison with previous evidence
Our finding that Kangfuxin solution ranks among the most effective regimens for clinical response aligns with previous conventional meta-analyses, which have shown that Periplaneta americana extract accelerates mucosal healing and improves symptom control in UC (Li et al., 2018; He et al., 2023).
Consistent with earlier safety reviews of these herbal interventions in gastrointestinal disease (Jiabao et al., 2023), none of the TCM–mesalazine combinations increased adverse event rates. Shaoyao decoction and Glycyrrhizae decoction ranked highest for safety, which may reflect their long-standing clinical use and generally mild adverse reaction profile.
Glycyrrhizae decoction and Baitouweng decoction were among the most effective interventions for Mayo score improvement, consistent with their traditional indications for damp-heat syndromes and inflammatory bowel disorders. The observed benefits are plausibly linked to suppression of mucosal inflammation and promotion of epithelial regeneration (Luo et al., 2022).
Scutellaria decoction showed the greatest reductions in IL-6 and TNF-α, supporting pharmacological evidence that Scutellaria baicalensis constituents (e.g., baicalin, baicalein) inhibit NF-κB signaling and downstream proinflammatory cytokine production (Liao et al., 2021).
Potential mechanisms
The differential efficacy observed among the eight TCM formulations likely reflects their distinct pharmacological profiles and mechanisms of action. Kangfuxin solution contains peptides, nucleotides, and other bioactive compounds that promote epithelial proliferation, angiogenesis, and tissue repair, contributing to its strong performance in mucosal healing (Shu, 1999). Shaoyao decoction, rich in paeoniflorin and glycyrrhizin, exerts anti-inflammatory effects by downregulating proinflammatory cytokines such as IL-6 and TNF-α (Zheng, 2013; Zhen et al., 2024). Glycyrrhizae decoction combines the anti-inflammatory, antimicrobial, and mucosal-protective actions of glycyrrhizin, berberine, and flavonoids, which may explain its broad efficacy across clinical, inflammatory, and microbiota-related outcomes (Liang et al., 2015). Scutellaria decoction, with its high content of baicalin and baicalein, potently inhibits inflammatory signaling pathways (Liao et al., 2021). The CurQD formula integrates curcumin’s NF-κB inhibitory effects with other herbal bioactives for potential synergistic anti-inflammatory action. Shenling Baizhu Powder supports gut barrier integrity and modulates intestinal immune responses through its polysaccharide and saponin components (Rao et al., 2022; Zhang et al., 2024). These mechanistic distinctions highlight the value of tailoring TCM selection to individual patient priorities—whether focused on symptom relief, inflammation control, or microbiota modulation.
As summarized in Table 2, each of the eight TCM formulations evaluated in this study contains key bioactive constituents that contribute to their therapeutic effects in ulcerative colitis (UC). These compounds are associated with various mechanisms of action, such as NF-κB inhibition, mucosal repair, anti-inflammatory effects, and gut microbiota modulation, all of which may explain the observed clinical benefits when combined with mesalazine. The multi-targeted mechanisms of these formulations address both systemic inflammation and intestinal barrier integrity, offering a comprehensive approach to managing UC. The diverse pharmacological profiles of these TCM formulations emphasize the potential of integrative therapies for UC, where the combination of TCM and mesalazine could result in enhanced therapeutic outcomes through synergistic mechanisms.
Long-term management of UC and safety considerations
While this study primarily focuses on short-term outcomes, long-term management of UC remains a significant concern. The potential for sustained mucosal healing and relapse prevention with mesalazine–TCM combinations warrants further investigation. While short-term studies suggest efficacy in symptom control and cytokine modulation, longer follow-up is necessary to assess whether these effects translate into durable remission and a reduction in relapse rates. Some formulations, such as Kangfuxin, may promote intestinal epithelial regeneration, which could support mucosal healing over the long term; however, this remains unverified in extended trials.
Additionally, the long-term safety of mesalazine–TCM combinations requires further exploration. Although no significant renal, hepatic, or gastrointestinal toxicities were observed in the short-term studies reviewed, prolonged use may reveal emerging adverse effects. Future studies should include renal function monitoring (e.g., serum creatinine levels), as well as liver and gastrointestinal health assessments, to ensure the safety of long-term combination therapy. Moreover, prospective studies with longer follow-up periods (12–24 months) are necessary to assess relapse rates, sustained remission, and the long-term efficacy of mesalazine–TCM combinations. Given the chronic nature of UC, optimizing long-term disease control while minimizing treatment-associated risks is essential to improving patient outcomes.
Further exploration of scutellaria Decoction’s anti-inflammatory effects
Scutellaria decoction has demonstrated significant anti-inflammatory effects in the treatment of UC, primarily through the inhibition of NF-κB, a key regulator of inflammation. While our study provides clinical evidence for its efficacy, the precise molecular mechanisms responsible for these effects require further exploration. To validate the hypothesis that Scutellaria decoction exerts its anti-inflammatory effects through NF-κB inhibition, biopsy studies in UC patients could allow for direct molecular analysis of NF-κB activity in colonic tissue. Cytokine profiling, both in serum and local mucosal samples, would help correlate NF-κB inhibition with reductions in proinflammatory cytokines such as TNF-α, IL-6, and IL-1β. These analyses would strengthen the evidence for Scutellaria decoction as a key modulator of inflammation in UC.
Furthermore, molecular pathway analyses, including RNA sequencing and protein expression analysis, could provide deeper insights into additional signaling pathways involved, such as MAPK and JAK-STAT, alongside NF-κB. Identifying the specific pathways modulated by Scutellaria decoction could uncover new therapeutic targets and help explain the variability in patient responses. Personalized treatment strategies, guided by biomarkers of response, could be developed to optimize treatment outcomes. Investigating resistance mechanisms could also shed light on why some patients show suboptimal responses, leading to better patient stratification and more effective therapies. Thus, while this study provides a solid foundation for the clinical efficacy of Scutellaria decoction, future research incorporating biopsy analysis, cytokine profiling, and molecular pathway studies is essential to further validate its mechanisms of action and optimize treatment for UC patients.
Personalized approach to Mesalazine-TCM combinations based on patient characteristics
Our findings can be translated into a pragmatic, hypothesis-generating framework that matches mesalazine–TCM combinations to patient phenotypes and therapeutic targets. For patients with a high symptomatic burden during active disease, combinations prioritizing rapid clinical response—CurQD and Kangfuxin—ranked most favorably for overall efficacy and are biologically plausible choices given their anti-inflammatory and mucosal-repair profiles. When endoscopic improvement is the principal goal, greater Mayo score reductions with Glycyrrhizae decoction, Baitouweng decoction (notably as a retention enema), and Kangfuxin suggest preferential use in patients with proctitis or left-sided disease, where a topical route may increase local exposure. In a systemic inflammatory phenotype (elevated IL-6/TNF-α at baseline), Scutellaria granules consistently ranked highest for cytokine reduction, with Kangfuxin as a reasonable alternative. For patients with microbiota dysbiosis or frequent relapse, Shaoyao decoction and Glycyrrhizae decoction—which were associated with increases in Bifidobacteria/Lactobacilli and reduced Escherichia coli—may be attractive for remission consolidation or maintenance alongside standard mesalazine dosing. Safety signals were broadly comparable to mesalazine alone; nevertheless, clinicians should continue routine renal monitoring for long-term mesalazine, and consider individual intolerance or allergy histories when selecting specific formulas. These subgroup inferences are constrained by study-level (aggregate) data, short treatment windows (3–12 weeks), and incomplete reporting of disease extent and biomarkers across trials; as such, they should be interpreted as exploratory rather than prescriptive. Prospective, biomarker-stratified and route-of-administration–aware RCTs—ideally with individual participant data—are needed to confirm effect modification by disease severity, extent, cytokine profiles, and baseline microbiota, and to determine whether these tailored pairings improve durable remission and relapse prevention.
Strengths and limitations
This study has several notable strengths. It is the first to apply a frequentist network meta-analysis to directly and indirectly compare eight standardized TCM–mesalazine combinations, incorporating a broad spectrum of outcomes, including clinical efficacy, safety, symptom scores, inflammatory biomarkers, and gut microbiota indices. The use of SUCRA rankings offers a transparent and systematic framework to guide clinicians in selecting adjunctive therapies aligned with specific treatment goals.
However, several limitations should be acknowledged. Most of the included RCTs were single-center studies conducted in China, which may limit the external generalizability of the results. The methodological quality varied across studies, with frequent omissions in reporting critical aspects such as allocation concealment, blinding, and intention-to-treat analyses. Additionally, the follow-up durations were generally short (≤12 weeks), which restricted our ability to evaluate long-term remission, relapse prevention, and sustained mucosal healing. For certain interventions, such as CurQD and Fufangkushen capsules, the evidence stemmed from a single trial, introducing considerable uncertainty into their SUCRA rankings. Moreover, microbiota-related outcomes were assessed in relatively few studies, limiting the robustness of the conclusions in this domain. Addressing these gaps through well-designed, multicenter RCTs with longer follow-up and comprehensive outcome reporting is essential to strengthen the evidence base.
Clinical implications and future research
The findings suggest that CurQD formula or Kangfuxin solution may be prioritized when the primary objective is short-term clinical remission, as these combinations showed the highest efficacy in rapid symptom relief. In contrast, Glycyrrhizae decoction and Baitouweng decoction may be more appropriate for reducing Mayo scores and promoting mucosal healing. Scutellaria decoction appears particularly effective in lowering systemic inflammatory cytokines, making it a valuable choice for patients with elevated IL-6 or TNF-α levels. Shaoyao decoction and Glycyrrhizae decoction, which help restore gut microbiota balance, may be beneficial in cases of concomitant dysbiosis, contributing to remission consolidation or maintenance when used alongside standard mesalazine dosing.
Future research should include large-scale, multicenter RCTs with rigorous blinding, standardized diagnostic and outcome criteria to allow valid cross-study comparisons. Extended follow-up periods are needed to evaluate the durability of treatment effects, relapse rates, and sustained endoscopic healing. In parallel, mechanistic investigations focusing on immune modulation, epithelial barrier restoration, and microbiota–host interactions will be critical to elucidate the underlying therapeutic pathways and refine patient selection for specific regimens.
Potential long-term benefits of combining TCM with mesalazine
While this network meta-analysis primarily focuses on short-term clinical outcomes (3–12 weeks), the chronic and relapsing nature of UC warrants consideration of long-term management strategies, particularly regarding relapse prevention and sustained remission. Combining mesalazine with TCM may offer several advantages in long-term UC care:
TCM formulations such as Kangfuxin and Glycyrrhizae decoction have demonstrated potential to reduce inflammation and promote mucosal healing, which may help prevent UC relapses. TCM formulations like Shaoyao decoction could also regulate the gut microbiota and improve intestinal permeability, supporting sustained remission and reducing flare-up frequency. Future studies with longer follow-up are needed to determine if these benefits translate into reduced relapse rates over time.
Given the crucial role of mucosal healing in UC management, TCM formulations that support intestinal epithelial repair (e.g., Kangfuxin) could be beneficial in maintaining mucosal integrity and preventing the progression of UC, including complications like colorectal cancer in patients with longstanding disease. While short-term evidence is promising, long-term studies are essential to confirm the durability of mucosal healing and the potential role of TCM in preventing disease progression.
The potential for nephrotoxicity and gastrointestinal issues with mesalazine highlights the need to ensure the safety of combination therapies. Some TCM formulations, such as Shaoyao decoction, have shown protective effects against gastrointestinal discomfort and liver abnormalities, which may help mitigate the side effects associated with prolonged mesalazine use. However, more studies are needed to assess the safety and tolerability of long-term TCM–mesalazine combinations.
Given the importance of long-term management in UC, further studies with extended follow-up periods (6–12 months or longer) are required to assess the full potential of TCM–mesalazine combinations. These studies should evaluate outcomes such as sustained remission, relapse rates, long-term mucosal healing, and the safety of chronic combination therapy. Future trials should also focus on monitoring renal and hepatic function to ensure the long-term safety of these combination treatments.
Future insights from advanced microbiota analysis
While microbiota outcomes in this study were based on broad profiling methods with limited taxonomic resolution, the use of 16S rRNA sequencing or metagenomic sequencing would provide more detailed and functional insights into microbial shifts in response to mesalazine–TCM combinations. These advanced techniques would allow for a more comprehensive analysis of microbial species abundance and diversity, as well as the functional capacity of the microbiota, including microbial metabolism and immune modulation.
Higher-resolution analysis through 16S rRNA sequencing could identify specific microbial species—such as Bifidobacteria, Lactobacilli, and Escherichia coli—that are directly associated with the pathogenesis of UC and could be modulated by TCM formulations. This approach could help clarify which species are beneficial or harmful in the context of UC and how TCM may alter these populations in ways that support disease remission.
Metagenomic sequencing would provide functional insights into how changes in the microbiota contribute to UC treatment. Specifically, it would allow for the identification of microbial genes and metabolic pathways, such as short-chain fatty acid production and immune modulation, that are crucial for maintaining gut health and reducing inflammation in UC. This approach could uncover microbial mechanisms that directly link to clinical outcomes, such as mucosal healing and symptom relief.
By linking microbial data with clinical outcomes, future studies could identify microbial biomarkers that predict treatment efficacy and resistance to mesalazine–TCM combinations. Understanding these correlations could lead to more targeted and personalized approaches in UC management, ultimately improving treatment outcomes.
Conclusion
This network meta-analysis of 34 randomized controlled trials provides evidence that combining selected TCM formulations with mesalazine enhances short-term clinical outcomes in mild-to-moderate UC without increasing adverse events. Specifically, the CurQD formula and Kangfuxin solution ranked highest for clinical remission, while Glycyrrhizae decoction and Baitouweng decoction showed the greatest effectiveness for Mayo score reduction. Scutellaria decoction was most effective in suppressing inflammatory cytokines, and both Shaoyao decoction and Glycyrrhizae decoction were particularly beneficial for modulating gut microbiota. The choice of adjunctive regimens should be based on the primary therapeutic goal. However, further high-quality, multicenter randomized controlled trials with extended follow-up are necessary to confirm these findings and provide robust, evidence-based recommendations for clinical guidelines.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ben-Horin S. Salomon N. Karampekos G. Viazis N. Lahat A. Ungar B. (2024). Curcumin-Qing Dai combination for patients with active ulcerative colitis: a randomized, double-blinded, placebo-controlled trial. Clin. Gastroenterology Hepatology 22 (2), 347–356.e 6. 10.1016/j.cgh.2023.05.023 37302449 · doi ↗ · pubmed ↗
- 2Chen H. (2014). Clinical observation of shenling baizhu san retention enema combined with oral mesalazine in the treatment of chronic nonspecific ulcerative colitis. Hebei J. Traditional Chin. Med. (11), 1643–1644.
- 3Chen J. (2018). Effects of shaoyao decoction retention enema on inflammatory factors in patients with damp-heat type ulcerative colitis. Chin. J. Integr. Med. Dig.
- 4Chen M. (2022). Effects of kangfuxin liquid combined with mesalazine on inflammatory and oxidative stress markers in ulcerative colitis patients. Mod. Med. Health Res. Electron. Version.
- 5Chen G. Huang H. Liu R. (2013). Analysis of shenling baizhu san combined with mesalazine in the treatment of spleen and stomach qi deficiency type ulcerative colitis. Chin. Med. Sci. 3 (17), 2.
- 6Chen Q. Fei S. Zhang Y. (2019). Effects and mechanisms of Bai tou weng decoction enema combined with oral mesalazine in the treatment of ulcerative colitis. Chin. Sch. Med. J. 33 (12), 4.
- 7Ding H. Deng Y. Y. Yang R. Q. Wang Q. S. Jiang W. Q. Han Y. L. (2018). Efficacy of huangqin decoction granules combined with mesalazine in the treatment of ulcerative colitis and its effect on inflammatory factors. Med. Test Clin. Res. 15 (6), 4. 10.1186/s 12974-017-1051-y 29304864 PMC 5755461 · doi ↗ · pubmed ↗
- 8Dong Z. (2018). Clinical effects of shenling baizhu san assisted Western medicine in the treatment of ulcerative colitis. Clin. Med. Res. Pract. 3 (5), 2.