Anomalous vertebral artery course causing radiculopathy: A case report and review of relevant literature
H. Jabri, K.T. Chen, S. Sharma, Y. Liu, J.L. Kim

TL;DR
A rare case of cervical radiculopathy caused by an unusual vertebral artery is reported, highlighting the need for careful pre-surgery planning to avoid complications.
Contribution
This case report adds to the limited literature on managing cervical radiculopathy caused by vertebral artery anomalies.
Findings
An ectatic vertebral artery at C4/5 was identified as the cause of cervical radiculopathy in a 73-year-old patient.
Minimally invasive surgery with advanced imaging techniques successfully improved symptoms and confirmed decompression.
Preoperative identification of vertebral artery anomalies is crucial to prevent surgical complications.
Abstract
Cervical radiculopathy typically results from degenerative disc disease, but rarely, an ectatic vertebral artery can cause it. This case report and literature review examine a unique instance of cervical radiculopathy due to an anomalous vertebral artery. Vertebral artery loop formation (VALF) is uncommon but can significantly impact surgical outcomes and poses a risk during cervical spine surgeries if unidentified preoperatively. To highlight the rare occurrence of cervical radiculopathy caused by an ectatic vertebral artery and discuss its surgical management. A 73-year-old female with left shoulder pain and C5 nerve root palsy underwent radiological evaluation, revealing an ectatic vertebral artery at C4/5. Treatment involved posterior tubular minimally invasive laminoforaminotomy with microvascular decompression, using intraoperative ultrasound and indocyanine green (ICG)…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
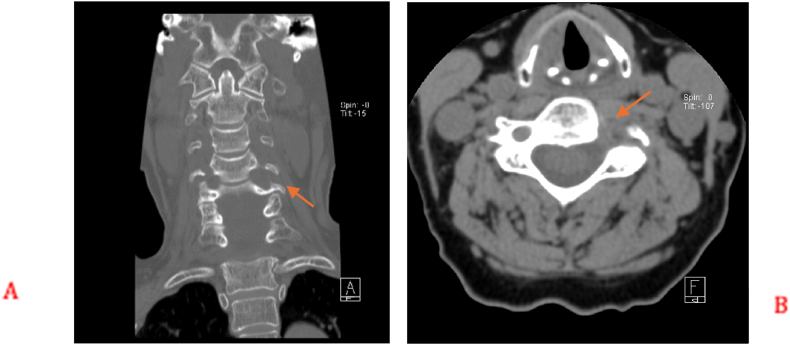 Figure 1
Figure 1 Figure 2
Figure 2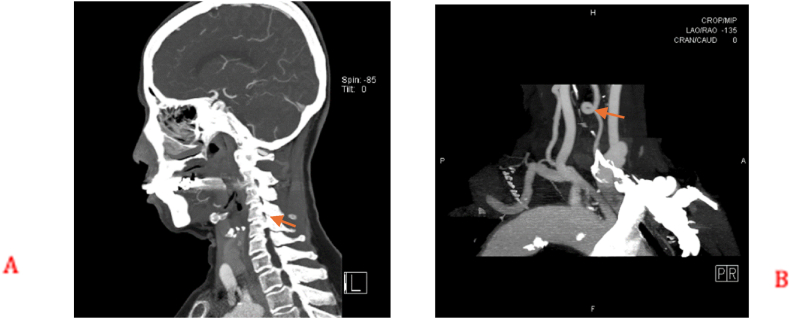 Figure 3
Figure 3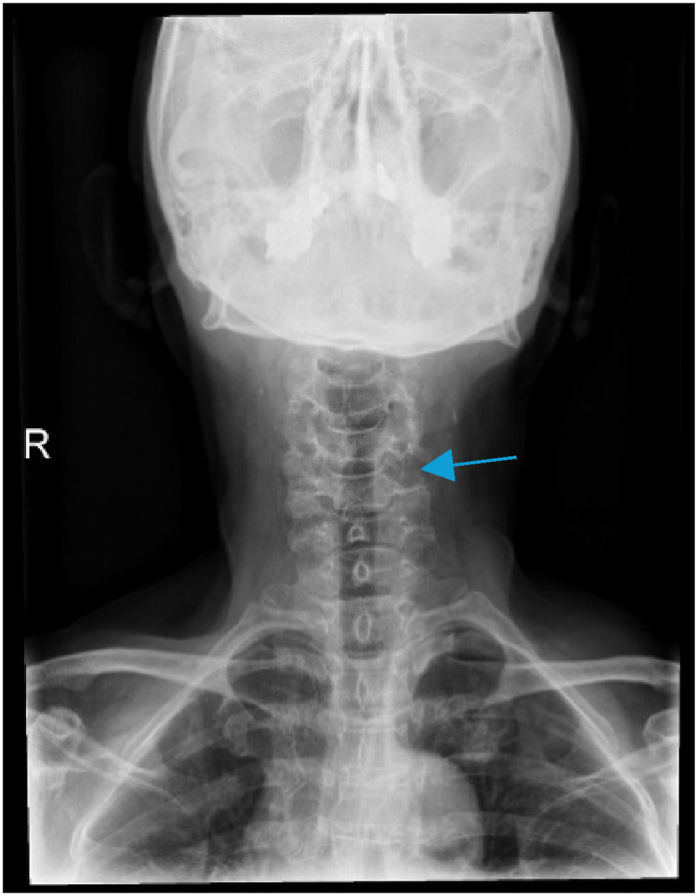 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSpinal Fractures and Fixation Techniques · Intracranial Aneurysms: Treatment and Complications · Cervical and Thoracic Myelopathy
Introduction
1
The origin of anomalous variation in the vertebral artery (VA) remains unknown but congenital abnormality, or as postulated degenerative theory, might be associated, but its incidence is low. The prevalence of vertebral artery loop formation (VALF) in a cadaveric study of 222 cervical spines was 2.7 % (Curylo et al., 2003). However, in a series of cervicobrachial pain without disc pathology, 13 out of 173 patients had VALF, suggesting that the incidence is around 7.51 % (Paksoy et al., 2003). Vertebral artery course remains one of the rare causes of cervical radiculopathy. Overlooking this anomaly might lead to injury to the vertebral artery during surgery for cervical radiculopathy.
Conventionally, the vertebral artery is divided into four segments (Abd el-et al., 1995). The artery courses dorsally in the first segment after originating from the subclavian artery until it enters the foramen of C6. Within the transverse foramina of C6 to C2 lies the second segment. The distal extracranial segment that is short and tortuous is the third portion which passes through the transverse foramen (TF) of the atlas and then curves backward and medially behind the lateral mass of the atlas, where it then makes a sharp turn to pierce the dura mater, thereby entering the cranium through the foramen magnum. The fourth segment is completely intracranial and ends when the vertebral arteries join at the lower pontine border to form the basilar artery (Caplan et al., 1988; Lang and Kessler, 1991). We shall also discuss our experience and present relevant literature review on the topic.
Case report
2
A 73-year-old female presented initially with left shoulder pain and brachaligia for which she received conservative treatment measures in another institute for 4 months. Upon arrival to our care, her pain was increasing, associated with left C5 nerve root partial palsy; her deltoid power was 3/5, her visual analog scale (VAS) score was 5 for neck pain and 6 for shoulder pain, while her neck disability index (NDI) was 35.56. Radiologic examination using cervical spine X-ray, computed tomography (CT) scan, magnetic resonance imaging (MRI) and magnetic resonance angiography (MRA), showed enlargement of the left C4/5 intervertebral foramen (Fig. 1). In addition, MRI, MRA, and CT angiogram showed a prominent ectatic vertebral artery in the left C4/5 intervertebral foramen (Fig. 2, Fig. 3), causing compression of the left C5 nerve root, where no associated herniated disc was visible. The radiologic findings were explained to the patient, and a decision was taken to perform surgical microvascular decompression of the nerve root by posterior tubular minimally invasive laminoforaminotomy approach, and interposing Teflon pledget between the artery and nerve. Intraoperative ultrasound and indocyanine green (ICG) were used to confirm the location of the vertebral artery and the patency of the vertebral artery in order to avoid unintentional kinking of the artery at the end of the procedure. The patient had an uneventful postoperative course, and her one-month follow-up showed improved deltoid power to 4/5 with VAS score of 1 for the neck pain and 2 for shoulder pain, while her NDI was 15.56. Postoperative X-ray (Fig. 4) and CT scan showed adequate bony decompression. Finally, MRI further confirmed the complete liberation of the nerve from the offending vessel (Fig. 5).Fig. 1(A) CT spine coronal view showing enlargement of the left C4-5 foramen. (B) Axial CT scan through C4-5 Foramen.Fig. 1. Fig. 2(A) MRI spine sagittal T2 did not reveal overt disc degeneration. (B) MRI spine axial T2 showing abnormal ectatic artery in the left C4-5 foramen.Fig. 2. Fig. 3(A) CT angiogram showing the abnormal vertebral artery in the foramen. (B) Tortuosity of the left vertebral artery.Fig. 3. Fig. 4Postoperative X-ray showing the foraminotomy window.Fig. 4. Fig. 5Postoperative MRI sagittal and axial cut showing adequate decompression of the nerve.Fig. 5
Discussion
3
Cervical radiculopathy is commonly caused by degenerative/discogenic herniated disc. However, other rare causes like ectatic vertebral artery course, congenital lesions, arteriovenous malformation, and tumors should be ruled out, especially when no disc herniation is identified on imaging (Anderson et al., 2014; Kim et al., 2010; Doweidar et al., 2014; Fink et al., 2010). Most surgeons should continue to locate the vertebral artery and its course during the preoperative evaluation for anterior or posterior cervical spine surgery, as this is a crucial step to avoid iatrogenic injury to these vessels (Oga et al., 1996; Peng et al., 2009). As previously mentioned, the prevalence of vertebral artery loop formation (VALF) in a cadaveric study of 222 cervical spines was 2.7 % (Curylo et al., 2003). In another series of cervicobrachial pain without disc pathology, 13 out of 173 patients had VALF, suggesting that the incidence is around 7.51 % (Paksoy et al., 2003). The etiology of this loop formation remains unknown but congenital abnormality, or as postulated degenerative theory, might be implicated. Oga et al., concluded after reviewing 22 cases that the extent of tortuosity is correlated with the severity of cervical spondylosis (Oga et al., 1996). This degenerative theory was also backed by Sakiadia et al., who postulated that the initial step in a process which is flowed by pulsatile pressure leads to migration and erosion of the adjacent structures (Fink et al., 2010). This theory might be supported by the higher occurrence of this pathology in older population.
The delayed symptomatic presentation of this presumably congenital vascular anomaly can be attributed to age-related degenerative changes. We hypothesize that although the arterial tortuosity was present from birth, the cumulative effects of aging - including intervertebral disc height reduction, osteophyte formation, and altered arterial wall compliance - progressively compromised the dimensions of the neural foramen. These physiological changes, absent in earlier decades of life, gradually exacerbated the mechanical impact of the pulsatile tortuous artery until reaching a critical threshold where neurological symptoms became apparent. This temporal relationship between congenital vascular anomalies and delayed symptom onset represents an important consideration in the diagnostic evaluation of patients presenting with similar neurological manifestations later in life (Oga et al., 1996; Sakaida et al., 2009).
Clinical presentation of cases with VALF varies based on pain, radiculopathy, myelopathy or a combination of symptoms; in some instances, vertebrobasilar insufficiency was also reported (Oga et al., 1996). Most patients may be asymptomatic and only diagnosed incidentally during imaging for trauma or other purposes. In a study of 239 symptomatic cervical trauma patients, 6 % of the patients had VALF (Toktaş et al., 2016).
The most common location of VALF in reported cases is C4-5, followed by C3-4, C5-6, and C6-7 and finally C1-2; its usually unilateral with reported cases of bilaterality, mainly in older population typically in the fifth and sixth decades of life (Toktaş et al., 2016). There is a higher prevalence among females rather than males.
In neurologically symptomatic cases, X-ray demonstrates an enlargement of the foramen transversarium with an erosion of the adjacent bone and sclerotic margins related to pulsatile arterial pressure (Sildiroglu et al., 2005). These bony details are better appreciated in axial and reconstructed CT images. Contrasted CT and MRI show signal void in the foramen with nerve compression. Other radiologic examinations such as CT, MRI, and MRA might also be equally informative in demonstrating the course and exact location of tortuosity. Furthermore, Doppler ultrasonography can help intraoperatively in confirming the location of artery (Bruneau et al., 2005). Intraoperative indocyanine green video angiography could be utilized; however, interpretation of the signal intensity should be carefully monitored, which varies with bolus timing, artery distance from the periosteal sheath, and presence of robustious venous plexus (Bruneau, 2010).
These patients' management should start with a trial of conservative management, where some reports confirmed symptom resolution with NSAIDs, blood pressure control, and physiotherapy. Surgery is considered in refractory cases with clear vascular compression or neurological deficit. Surgical decompression can be employed anteriorly, posteriorly, or with combined approaches, as seen in different reports in the literature.
The ultimate surgical goal is freeing the compressed neural structure, whether nerve root or spinal cord, or both. Although, the anterior approach that exposes and frees the vertebral artery carries the risk of recurrent laryngeal nerve and carotid artery injuries. Exposure carried out using laterally passed longus colli to expose the transverse process might damage the sympathetic nerves and may lead to Horner's syndrome. The vessel loop can also be relocated, but the anterior approach is not possible above C3 level.
In the posterior approach, foraminotomy can be performed using minimal invasive surgery tubular dilator or microscopic technique, which indirectly decompresses the nerve, freeing adhesions, with the feasibility of using telfa patch interposed between the nerve and offending vessel loop, hence reducing the likelihood of nerve recompression. Separation of the vessel loop using sling technique(Korinth and Mull, 2007; Tandon et al., 2013) or bypass and reconstruction have been reported in the literature (Sakaida et al., 2009). A technique using a cellular human dermis sling that is wrapped around the VA and sewn to the adjacent paraspinous muscles was reported by Tandon et al. (2013) Blood flow adequacy of the VA should be monitored and evaluated intraoperatively to avoid immediate kinking. One advantage of the sling method is the higher likelihood of separation maintenance. Padding may reduce the pulsatile compression of the offending vessel loop, similar to the surgeries commonly performed in microvascular decompression surgery in cranial pain syndromes.
While bony decompression is the foremost important step in these patients, it might not be adequate to alleviate the patient's symptoms. If either the anterior or posterior approach is adopted, there is a risk of instability, depending mainly on the amount of bone removed to achieve adequate decompression, which could be higher in the posterior approach. Instability in these types of surgery has not been reported in the literature and fusion was not required.
A surgical approach is usually dictated by the extent of every individual patient's pathology, the extent of decompression needed, as well as the surgeon's preference and comfort (Table 1).Table 1. Summary of literature search.Table 1. ReferenceSymptomCervical LevelApproachOutcomeCommentAnderson et al. 1970 (Anderson et al., 2014)Neck painC3-4Posterolateral foraminotomyResolved painZimmerman et al. 1970 (Zimmerman and Farrell, 1970)Occipitocervical neuralgiaC4-5Posterolateral laminectomyResolved painSharma et al., 1993 (Read More)Occipital neuralgiaC2-3Posterolateral laminectomy,VDResolved painKlippel Feil syndrome, cellulose for VDSatoh et al. 1993 (Sharma et al., 1993)Neck, shoulder, arm painC1-2Suboccipital and C1 decompressionResolved painSuture to anchorvertebral arteries to duraDuthel et al., 1994 (Umemori et al., 2009)Cervicobrachial neuralgia, second and third digit paresthesiaC5-C6Anterolateral, VDResolved symptomsTeflon for VDDetwiler et al.1998(Detwiler et al., 2009)Cervical and scapular painC3-C4Posterolateral laminectomyand facetectomy, VDResolved painSakaida et al. 2001 (Sakaida et al., 2009)C5 radiculopathyC4-C5Anterolateral, vascular reconstructionResolved painEnd-to-end anastomosisKorinth et al. 2007 (Korinth and Mull, 2007)Neck, shoulder painC4-C5Anterolateral, VDResolved painTeflon for VDDahdaleh et al., 2010 (Dahdaleh et al., 2010)PresyncopeC2-3, C3-4Posterior cervical fusionResolved symptomsHage et al. 2012 (H et al., 2012)Neck pain, C7 radiculopathyC6-C7Anterolateral, VDResolved painChibbaro et al., 2012 (Chibbaro et al., 2012)C6 radiculopathyC5-C6Anterolateral, VDResolved painTandon et al., 2013 (Tandon et al., 2013)Neck, shoulder painC4-C5Anterolateral, VDResolved painAllograft slingEksi et al. 2016 (Toktaş et al., 2016)Neck pain, weaknessC5-C6Posterolateral laminectomy and foraminotomyResolved painWang et al. 2017 (Duthel et al., 1994)C6 weakness, paresthesia, radiculopathyC5-C6Anterolateral, VDResolved symptomsTeflon for VDWang et al. 2017 (Duthel et al., 1994)Head, neck painC3-C4Anterolateral, VDImproved symptomsVenteicher et al., 2018 (Venteicher et al., 2018)C5 weakness, radiculopathyC4-C5Anterolateral, VDResolved symptomsTeflon for VDYamada et al., 2018 (Yamada et al., 2018)occcpitalgia, sensory abnormalitiesC1-2Suboccipital craniotomy and C1 laminectomyResolved painPTEF for VDPresent studyNeck, shoulder pain, C5 weakness, radiculopathyC4-C5Posterolateral tubular foraminotomyImproved symptomsTeflon for VD
Conclusion
4
Anomalous origin of the VA may not be the sole reason behind a disease process. However, it may undoubtedly lead to a misdiagnosis during cervical radiculopathy diagnosis. Therefore, detailed information is crucial before any surgery or endovascular intervention in the neck region. Conservative treatment remains the mainstay of management of these anomalies. In refractory cases, surgery is indicated whether approached anteriorly, posteriorly or combined approaches.
The ultimate surgical goal is decompression of the nerve root to alleviate radiculopathy and allow weakness to improve (ICG); by halting the pulsatile compression of the artery on the nerve. Furthermore, the possibility of iatrogenic instability resulting from decompression surgery can be prevented by adding fusion surgery, if needed.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Abd el-Bary T.H.Dujovny M.Ausman J.I.Microsurgical anatomy of the atlantal part of the vertebral artery Surg. Neurol.444199539240010.1016/0090-3019(95)00033-xdiscussion 400, indexed in Pubmed: 85532618553261 · doi ↗ · pubmed ↗
- 2Anderson R.E.Norman Shealy C.Cervical pedicle erosion and rootlet compression caused by a tortuous vertebral artery Radiology 963201453753810.1148/96.3.5375456309 · doi ↗ · pubmed ↗
- 3Bruneau M.Video 662201030531110.1227/01.NEU.0000363596.52283.6520087130 · doi ↗ · pubmed ↗
- 4Bruneau M.Cornelius J.F.George B.OF the V ERTEBRAL a RTERY to the 57200526226710.1227/01.NEU.0000176414.58086.2B 16234673 · doi ↗ · pubmed ↗
- 5Caplan L.R.Ertebrobasilar system syndromes Vinken P.J.Bruyn G.W.Klawans Handbook of Clinical Neurology. Vascular Disease. Part 11988 Elsevier Science Publisher B.V.Amsterdam 371409
- 6Chibbaro S.Mirone G.Yasuda M.Marsella M.Di Emidio P.George B.Vertebral artery loop - a cause of cervical radiculopathy World Neurosurg.783–42012375.e 11375.e 1310.1016/j.wneu.2011.12.00222381311 · doi ↗ · pubmed ↗
- 7Curylo L.J.Mason H.C.Bohlman H.H.Yoo J.U.Tortuous course of the vertebral artery and anterior cervical decompression Spine 252220032860286410.1097/00007632-200011150-00004(Phila Pa 1976)11074670 · doi ↗ · pubmed ↗
- 8Dahdaleh N.S.Albert G.W.Hasan D.M.Multiple symptomatic vertebral artery loops treated with posterior cervical fusion J. Clin. Neurosci.176201078879010.1016/j.jocn.2009.10.00420356748 · doi ↗ · pubmed ↗