A single report tells the story: Ventricular fibrillation caused by vasospastic angina recorded from an implantable loop recorder
Daiki Nakajima, Hitoshi Mori, Kazuhisa Matsumoto, Yoshifumi Ikeda, Ritsushi Kato

TL;DR
A patient's unexplained fainting was traced to heart rhythm issues caused by vasospastic angina using an implantable loop recorder.
Contribution
This is the first documented case where ventricular fibrillation due to vasospastic angina was diagnosed using a single implantable loop recorder electrogram.
Findings
Ventricular fibrillation was detected via ILR following ST-T elevation and a premature ventricular contraction.
Vasospastic angina was confirmed as the cause of unexplained syncope in an 80-year-old male.
Implantable loop recorders proved effective in diagnosing arrhythmias and their underlying causes.
Abstract
Implantable loop recorders (ILRs) are essential for diagnosing unexplained syncope, particularly when cardiogenic causes are suspected. An 80-year-old male experienced unexplained syncope following chest tightness, with no obstructive coronary findings. A comprehensive cardiac evaluation failed to identify the underlying cause, however Holter electrocardiography showed non-sustained ventricular tachycardia, suggesting cardiogenic syncope. Therefore, we proceeded with ILR implantation. Ten days post-discharge, ILR monitoring detected ventricular fibrillation (VF) preceded by ST-T elevation and triggered by a premature ventricular contraction, confirming vasospastic angina (VSA) as the cause. This is the first documented case where VF due to VSA was diagnosed via a single ILR electrogram. ILRs thus play a crucial role in managing syncope. Implantable loop recorder (ILR) is useful not…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
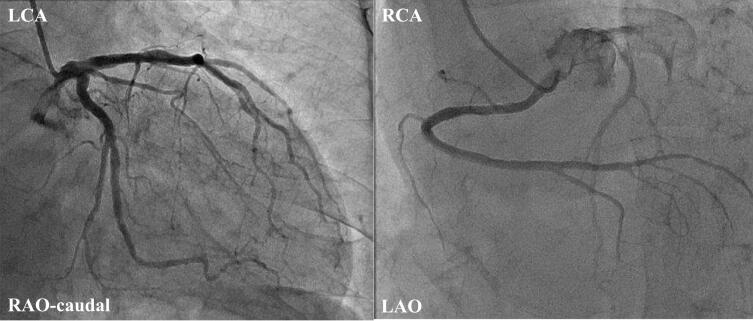 Figure 1
Figure 1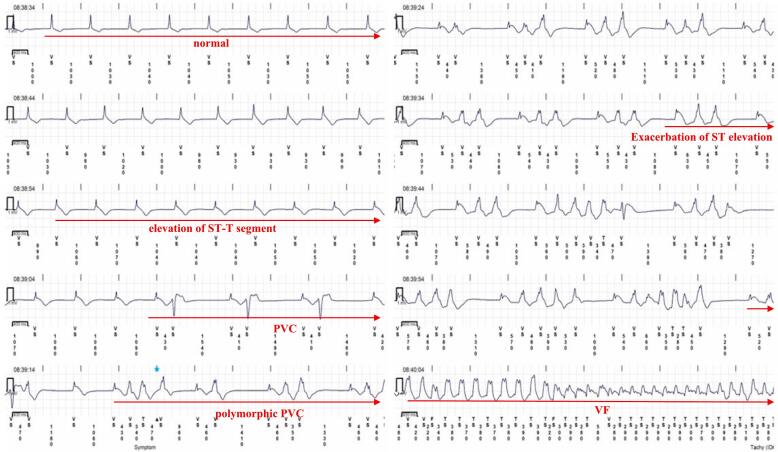 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · Cardiac Imaging and Diagnostics · Cardiac Arrhythmias and Treatments
Introduction
Implantable loop recorders (ILRs) have been widely used to evaluate the cause of unexplained syncope by continuously recording the heartbeat. Clinical guidelines recommend the use of ILRs as a Class I indication for cases of unexplained syncope suspected to be cardiogenic syncope [1]. By recording the electrocardiogram at the time of the syncope, ILRs enable the analysis of arrhythmias that occur during the event, making it useful for a diagnosis. Several reports have noted the utility of ILRs for diagnosing syncope, and a few reports have revealed the utility of ILRs for ventricular arrhythmias [2,3]. Nakai et al. reported a case of syncope caused by vasospastic angina (VSA), in which an ILR was useful for the diagnosis [4]. In that report, atrioventricular block following ST-T elevation was detected by the ILR, contributing to the diagnosis. However, to our knowledge, there have been no reports about ventricular fibrillation (VF) following ST-T elevation caused by VSA that was diagnosed by a single ILR electrogram.
Case report
An 80-year-old male presented to a previous hospital for further evaluation of chest tightness and unexplained syncope. The syncope had recurrently occurred following episodes of chest pain lasting several minutes, raising suspicion of coronary ischemia as the underlying cause. The patient underwent evaluation including transthoracic echocardiography, Holter electrocardiography, and coronary angiography. Transthoracic echocardiography showed a preserved ejection fraction of 65 %, with no wall motion abnormalities or hypertrophy. Holter electrocardiography revealed no ST-segment changes or non-sustained ventricular tachycardia during hospitalization. Coronary angiography was subsequently performed and showed no obstructive lesions (Fig. 1). Furthermore, no ST-segment changes or ventricular arrhythmias were observed throughout the hospital stay. Therefore, cardiogenic syncope due to arrhythmias was suspected, and he was referred to our hospital for further evaluation of the syncope. An ILR was implanted for the evaluation of the unexplained syncope based on the clinical guidelines. Ten days after discharge, VF was reported in the early morning by the alert system of the remote monitoring system. He was urgently hospitalized and the electrocardiogram recorded by the ILR was analyzed, showing that VF was triggered by a premature ventricular contraction, preceded by ST-T elevation (Fig. 2). Given that the event occurred in the early morning, ischemic changes with ST-T elevation were positive, and no significant stenosis was found on coronary angiography, this case was diagnosed as VF caused by variant angina due to VSA. After this diagnosis, calcium channel blockers and isosorbide dinitrate were initiated. Since starting the medical therapy, he has not experienced any syncope or lethal arrhythmia events during the ILR monitoring.Fig. 1. Coronary angiography shows no obstruction of the left coronary artery (left panel) and right coronary artery (right panel).LAO, left anterior oblique; LCA, left coronary artery; RAO, right anterior oblique; RCA, right coronary artery.Fig. 1. Fig. 2Electrogram recorded by implantable loop recorder. After the initially normal ST-T segment exhibited a mild elevation, multiple PVCs appeared, progressing to polymorphic PVCs. This was followed by an exacerbation of the ST elevation, which finally led to VF.PVC, premature ventricular contraction; VF, ventricular fibrillation.Fig. 2
Discussion
With the miniaturization of ILRs, they play an important role in the management of syncope. ILRs can diagnose the cause of syncope more effectively than conventional syncope evaluations, including electrophysiological testing, in cases of unexplained syncope [5]. Previous reports have also noted that ILRs are useful for detecting syncope caused by VSA and for diagnosing atrioventricular block associated with VSA following ST-T elevation [4]. ILRs are valuable not only for identifying arrhythmias as the cause of syncope but also for diagnosing the underlying condition. However, to our knowledge, this is the first report of VF caused by VSA that was diagnosed through a single ILR electrogram. A single recording from an ILR revealed everything.
Conclusion
ILRs are invaluable for diagnosing unexplained syncope, providing unique insights into arrhythmias and underlying conditions, as demonstrated in this first reported case of VF caused by VSA.
Patient consent statement
Patient consent for publication was obtained.
Consent for publication
Patient consent for publication was obtained.
Ethics statement
Not applicable.
Funding information
None.
Authors' contributions
DN and HM drafted the manuscript; KM and YI revised the manuscript; RK supervised the study.
Clinical trial registration
Not applicable.
Declaration of competing interest
HM received lecture fees from Biosense Webster Japan and Boston Scientific Japan. Our department also received grant support from Boston Scientific Japan and Abbott Medical Japan.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Takase B.Ikeda T.Shimizu W.Abe H.Aiba T.Chinushi M.Koba S.Kusano K.Niwano S.Takahashi N.Takatsuki S.Tanno K.Watanabe E.Yoshioka K.Amino M.JCS/JHRS 2022 guideline on diagnosis and risk assessment of arrhythmia J Arrhythm 4020246557523913989010.1002/joa 3.13052 PMC 11317726 · doi ↗ · pubmed ↗
- 2Przyżycka P.Kałowski M.Poddębska I.Kaczmarek K.Ptaszyński P.Wranicz J.K.Cygankiewicz I.Self-terminating ventricular fibrillation recorded by an implantable loop recorder as a cause of syncope - a case report J Electrocardiol 5120186176192999700010.1016/j.jelectrocard.2018.04.006 · doi ↗ · pubmed ↗
- 3Kawazoe H.Ikeda S.Uga S.Kadota H.Yamane K.I.Kotani T.Shimizu H.Izumi N.Ohshima K.Hamada M.A case of idiopathic ventricular fibrillation in which implanted loop recorder was useful in application decision for implantation of implantable cardioverter-defibrillator J Cardiol Cases 62012 e 59e 633053307210.1016/j.jccase.2012.06.003PMC 6269273 · doi ↗ · pubmed ↗
- 4Nakai T.Sonoda K.Watanabe I.Diagnosis of coronary spastic angina by implantable loop recorder Europace 1520136622302433610.1093/europace/eus 318 · doi ↗ · pubmed ↗
- 5Krahn A.D.Klein G.J.Yee R.Skanes A.C.Randomized assessment of syncope trial: conventional diagnostic testing versus a prolonged monitoring strategy Circulation 104200146511143533610.1161/01.cir.104.1.46 · doi ↗ · pubmed ↗