Prehospital emergency response and management of pregnancy-associated haemorrhage in KwaZulu-Natal Province, South Africa: A Retrospective Cross-Sectional Study
S Govender, OP Khaliq, T Abel, J Moodley

TL;DR
This study examines delays and management gaps in emergency care for pregnancy-related bleeding in South Africa, highlighting the need for better training and resources to reduce maternal deaths.
Contribution
The study provides new insights into EMS response times and clinical practices for postpartum haemorrhage in a South African setting.
Findings
Over half of PAH cases had ambulance response times exceeding 60 minutes.
Only 42.6% of PPH patients had consistent vital signs monitoring during transport.
44.3% of PPH cases received no intravenous fluids despite signs of shock.
Abstract
Pregnancy-associated haemorrhage (PAH) is a leading contributor to maternal mortality in KwaZulu-Natal (KZN) and the fourth most common cause in South Africa. Delays in treating PAH increase maternal mortality; prompt prehospital response is therefore critical to improve outcomes. The aim of this study was to analyse response times and clinical management of PAH by public sector Emergency Care Providers in KZN, looking specifically at postpartum haemorrhage (PPH). A retrospective cross-sectional study was conducted in two phases. Phase 1 involved analysis of emergency call centre records (n = 4779) assessing response time patterns. Phase 2 analysed randomly selected PPH cases (n = 61) to assess clinical management practices. Descriptive statistics summarised demographics, response patterns, and clinical practice, Pearson correlation examined the relationships between time variables,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
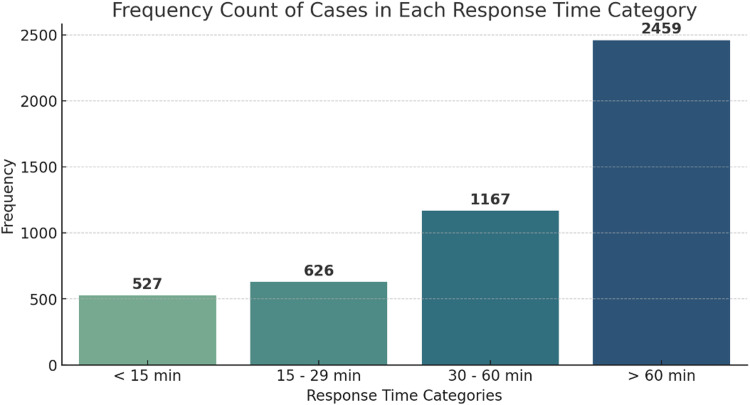 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal and fetal healthcare · Pregnancy-related medical research · Cardiac Arrest and Resuscitation
African relevance
- •Pregnancy-associated haemorrhage, particularly postpartum haemorrhage, remains a leading direct cause of maternal mortality in sub-Saharan Africa where access to emergency care is limited due to lack of transport, poor infrastructure and rurality.
- •There is limited research regarding EMS response and clinical management of obstetric emergencies in an African setting despite a lack of transport being a key contributor to maternal mortality.
- •Findings of the current study highlight gaps in response times and the immediate clinical management that can be mitigated through training, policies and strategic allocation of resources (ambulances).
- •Lessons learnt from this study can also inform efforts to improve maternal outcomes in other resource-limited African EMS systems.
Introduction
Maternal mortality remains a global burden, with approximately 800 deaths per day, most occurring in low- or middle-income countries (LMIC) [1]. While Obstetric Haemorrhage (OH) is the leading direct cause of maternal death globally [1], it is also a significant challenge in South Africa (SA) with the KwaZulu-Natal (KZN) province being the most affected [2]. One of the factors contributing to maternal deaths is delay in women receiving appropriate care which Thaddeus and Maine [3] stated, occurred in 3 phases: (i) delay in the decision to seek care; (ii) delay in reaching a healthcare facility; and (iii) delay in getting adequate care at the healthcare facility [4].
Delays in reaching facilities are often due to pregnant women walking long distances from rural homesteads and limited transport options [5], with similar findings reported in Ghana [6] and Mozambique [7]. In SA, the National Committee on Confidential Enquiries into Maternal Deaths (NCCEMD) [2] documented delays across all three phases, highlighting lack of emergency transport (phase 2) as a key avoidable factor. These delays are compounded by poor rural road networks [8] and inequalities in health infrastructure and public services in SA [9].
Emergency Medical Services (EMS) are integral in responding to, treating and transporting pregnant women with haemorrhage in pregnancy to appropriate healthcare facilities. This role is aligned to the World Health Organization’s (WHO) drive to improve access to “the most disadvantaged, marginalised and hard-to-reach populations, to ensure that no one is left behind” [10]. However, Govender et al. [11] reported a constrained EMS system in SA, with suboptimal components delaying access to care, consistent with other KZN studies linking ambulance shortages to poor response times [12,13].
In response, the SA Department of Health introduced strategies such as the Campaign on Accelerated Reduction of Maternal (and Child) Mortality in Africa (CARMMA), advocating dedicated obstetric ambulances. However, implementation in KZN has been inconsistent due to staffing and vehicle shortages [11].
Given these challenges and limited research specific to this field, this study was designed to focus on OH, a late pregnancy complication. Preliminary data, however, revealed high numbers of early pregnancy complications prompting a broader investigation into pregnancy-associated haemorrhage (PAH), which encompasses haemorrhage in all the trimesters of pregnancy and the postpartum period. Accordingly, the aim of this research was to analyse prehospital response times and clinical management of PAH, by EC providers in KZN Province of SA. While the research broadly considered PAH, the assessment of clinical management focused on postpartum haemorrhage (PPH) as a clinically significant and commonly encountered subset of PAH for detailed analysis.
Methodology
Study design and setting
This was a cross-sectional study using records review to analyse cases of PAH managed by public sector EC providers in KZN between January 2019 to June 2021. The study period spans pre-, intra- and post-COVID-19 phases. PAH was recognised as bleeding in all three trimesters of pregnancy [2].
KZN, one of the provinces in SA, spans 94,361 km² and has the second-largest population (12 312 712) [14]. The province comprises 11 districts, each containing a mix of rural and urban populations [15]. While all districts include both settlement types, 9 are predominantly rural, whereas eThekwini and uMgungundlovu are predominantly urban [15]. Rural areas are defined as low-density municipalities with limited infrastructure and agricultural economies, while urban areas have higher density, developed infrastructure, and diverse economies. This rural–urban mix is relevant for interpreting EMS response patterns and transport times [15].
Each district has both field EMS stations and an Emergency Call Centre (ECC), all staffed by EC providers working 12-hour shifts (07:00–19:00 and 19:00–07:00) [16]. Each telephone call is time-stamped on a vehicle-control form (VCF) that tracks the patients’ transit to hospital. Completed VCFs are entered into one of three electronic database subsets: (i) general cases, (ii) principally inter-facility transfers, and (iii) obstetric cases attended to by dedicated “obstetric ambulances.”
Study population
The study population comprised all PAH cases attended by public-sector EMS in KZN during the study period. Prehospital care was delivered by EC providers registered with the Health Professions Council of South Africa (HPCSA) at one of three levels: Basic Life Support (BLS), Intermediate Life Support (ILS), or Advanced Life Support (ALS), as detailed in online supplementary material A. These levels correspond to distinct capabilities relevant to PAH management; for example, BLS providers are not authorised to administer intravenous fluids or medications, ILS and ALS providers may initiate fluid resuscitation, and only ALS providers are permitted to administer uterotonics such as oxytocin.
Sampling strategy
A multiphase (two-phase) sampling strategy was employed in this study.
Phase 1**:** During the study period, 10017 PAH-related ECC records were identified. Inclusion criteria were interfacility-transfer (IFT) cases with complete sequential timestamps (call received and dispatch) and patient details. Exclusion criteria were records that did not meet these requirements. Using purposive sampling, 4779 IFT cases were selected, as these were clinician-reported rather than call-centre diagnosed, providing greater diagnostic reliability. This subset was considered most appropriate for analysing response times and diagnostic patterns.
Phase 2**:** These 4779 cases were stratified into eight haemorrhage categories. Using purposive sampling, the PPH stratum (210 cases) was selected, given its status as the leading cause of PAH-related maternal death in KZN. Focusing on PPH allowed for an in-depth assessment of clinical management, as analysing all eight PAH categories would have increased complexity and reduced feasibility due to differing clinical protocols. From this stratum, a proportionate, computer-generated simple random sample of 61 records was drawn across six participating districts, ensuring clinical relevance, geographic representation, and a manageable workload for manual data retrieval and review.
Data collection
Data were obtained from 6 of the 11 districts in KZN (uThukela, uMzinyathi, King Cetshwayo, uMgungundlovu, Ugu, and iLembe). The remaining 5 districts were excluded due to the absence of electronic case records.
Phase 1: Each district ECC used a standardized electronic database to record cases. Data that required analysis included the pre-response time (PRT): calculated from time the call was received to the dispatch of the ambulance and response time (RT): calculated from the time the call was received to the arrival of the ambulance on-scene [17]. Data were verified before being transferred to SPSS v29 for analysis. Additionally, cases were grouped into <20 weeks (early pregnancy haemorrhage) and >20 weeks (late pregnancy haemorrhage).
Phase 2: District staff scanned and submitted 61 randomly selected PPH patient report forms to the research team. Forms were reviewed for key indicators: maternal history, blood loss estimation, initial and continuous vital signs, fluid resuscitation relative to shock status, provider level, and documentation. The review focused on EMS care from loading at the referring facility to handover at the receiving hospital.
Data and statistical analysis
Data were analysed in Microsoft Excel and SPSS v29. Descriptive statistics (means, medians, frequencies) summarised demographics, response intervals, and clinical management. Pearson’s correlation tested the relationship between pre-response and total response times, and Chi-square tests examined associations between provider qualification and compliance (p < 0.05).
Shock Index (SI) was classified as <0.6 (no shock), 0.6–0.9 (compensated), 1.0–1.4 (mild), 1.5–1.9 (moderate), and ≥2.0 (severe) to grade PPH severity and assess adequacy of prehospital care. Interventions including vital sign monitoring, IV access, fluids, medication, and documentation were benchmarked against national maternity guidelines, HPCSA EMS protocols, and WHO standards to evaluate alignment with patient condition and EC provider level of care.
Ethical and health regulatory approvals
Ethics approval for the study was obtained from the University of KwaZulu-Natal Biomedical Research Ethics Committee (BREC) (ref.no. BREC/00,003,780/2022) and the KwaZulu-Natal Provincial Department of Health (ref.no. KZ_202,205_008).
Results
Between January 2019 and June 2021, there were 10 017 cases of PAH recorded in the study districts. These formed the basis for the analysis. From this dataset, 4 779 interfacility transfer (IFT) cases were identified for detailed review. Phase 1 analysed response trends and causes of PAH while Phase 2 analysed clinical management specific to PPH. Broader three-year data (January 2019–December 2021) is provided in the online supplementary B to offer contextual background without interrupting the flow of the main results.
Phase 1 – Response trends and PAH causes
Some 4779 cases of PAH were transported to healthcare facilities, during the study period. Among these patients, 54 % (n = 2577) had a gestation of <20 weeks, 17 % (n = 822) >20 weeks, and 29 % (n = 1380) indeterminate. The mean age of patients across all cases was 27 years (range: 13 – 48). Miscarriage accounted for 53% (n = 2535) of the cases and was the leading cause of PAH, followed by APH with 10.3% (n = 492), PPH with 4.4% (n = 210) and indeterminate group with 28.9% (n = 1380) (Table 1).Table 1. Causes of pregnancy-associated haemorrhage attended by Emergency Care providers from January 2019 to June 2021 (n = 4779).Table 1Cause and gestation201920202021(until June)Total< 20 weeksRuptured ectopic pregnancy17 (0.4)18 (0.4)7 (0.1)42 (0.9)Miscarriage1002 (21)1050 (22)483 (10)2535 (53)> 20 weeksAntepartum haemorrhage180 (3.8)219 (4.6)93 (1.9)492 (10.3)Ruptured uterus2 (0.04)4 (0.08)2 (0.04)8 (0.2)Vaginal birth trauma (3rd/4th degree tear)16 (0.3)11 (0.2)8 (0.2)35 (0.7)Postpartum haemorrhage82 (1.7)86 (1.8)42 (0.9)210 (4.4)Retained placenta25 (0.5)38 (0.8)14 (0.3)77 (1.6)UnknownIndeterminate bleeding502 (10.5)622 (13)256 (5.4)1380 (28.9)Total1826 (38.2)2048 (42.9)905 (18.9)4779 (100)
Of the cases, 18.4 % (n = 880) were interhospital transfers, while 81.6 % (n = 3899) were from primary health facilities (clinics or community health centres) to hospitals. Most patients (75.7 %, n = 3618) were managed by ILS providers, with 20.7 % (n = 990) by BLS and 3.6 % (n = 173) by ALS.
Fig. 1 shows the distribution of ambulance response times (n = 4779). In 51.5 % (n = 2459) of the PAH cases, ambulances took >60 min (response time) to reach the scene. Only 11 % (n = 527) of the ambulances reached the scene within 15 min.Fig. 1. Response time categories for pregnancy-associated haemorrhage.Fig 1
The pre-response time (PRT) had a median of 30 min (range: 1–609) with a 5 % trimmed mean of 50.9 min, indicating a positively skewed distribution influenced by extreme outliers. The overall response time (RT) showed a similar pattern, with a median of 63.5 min (range: 3–683) and a 5 % trimmed mean of 85.7 min. These wide ranges and skewness likely reflect operational challenges, including ambulance shortages, long interfacility transfer distances, and occasional data logging errors, which inflate the upper extremes. Pearson correlation analysis revealed a strong association between PRT and RT (r = 0.929, p < 0.01).
Across the 6 districts (Table 2), King Cetshwayo recorded the longest median PRT of 39 min (IQR 87) and a median RT of 79 min (IQR 102). In contrast, uThukela had the shortest median pre-response time of 24 min (IQR 58) and a median response time of 53 min (IQR 75) .Table 2. Response trends for cases of pregnancy-associated haemorrhage attended by Emergency Care providers from January 2019 to June 2021 (n = 4779).Table 2DistrictTotal cases (n)TimesMeanMedianPercentile 25Percentile 75****IQRiLembe721Pre-Response time53.4230.009.0078.0069.00Response time72.9552.0024.00102.0078.00King Cetshwayo1561Pre-Response time71.8539.0013.00100.0087.00Response time103.7879.0040.00142.00102.00Ugu715Pre-Response time61.1933.0010.0089.0079.00Response time87.2664.0037.00117.0080.00uMgungundlovu302Pre-Response time68.6030.0010.0092.0082.00Response time98.1967.0030.00136.00106.00uMzinyathi301Pre-Response time49.8126.007.0064.0057.00Response time79.1763.0030.00100.0070.00uThukela1179Pre-Response time49.7824.009.0067.0058.00Response time72.6153.0023.0098.0075.00
Phase 2 – Clinical management of PPH
Some 61 cases of PPH were retrieved for analysis, with mean age 25 years; 73.8 % (n = 45) were transferred by EC providers from primary health care facilities to hospital and 26.2 % (n = 16) were transferred between hospitals.
In Phase 2, each patient report form was manually reviewed to assess prehospital actions: vital signs, IV access, fluid resuscitation, medication administration, and documentation of blood loss against the relevant standards outlined in the National Maternity Guidelines , EC provider Clinical Practice Guidelines and WHO recommendations. Patient assessment was evaluated across four indicators: (i) maternal history, (ii) estimation of blood loss, (iii) initial vital signs, and (iv) continuous vital signs monitoring. Treatment was assessed by fluid administration relative to shock status, determined by the Shock Index.
Among PPH patients, 88.5 % (n = 54) of EC providers were non-compliant in obtaining patient history and 96.7 % (n = 59) in estimating blood loss (Table 3). While 91.8 % (n = 56) assessed initial vital signs, ongoing monitoring in transit was absent in 57.4 % (n = 35). Blood loss was described as bleeding (77 %; n = 47), severe bleeding (11.5 %; n = 7), bleeding with clots (9.8 %; n = 6), and profuse bleeding (1.6 %; n = 1).Table 3. Patient assessment for Post Partum Haemorrhage (n = 61).Table 3Clinical assessment indicatorCompliancen( %)****p-valueMaternal historyCompliant7 (11.5)< 0.001Non-Compliant54 (88.5)Estimated fluid lossCompliant2 (3.3)< 0.001Non-Compliant59 (96.7)Vital signsCompliant56 (91.8)< 0.001Non-Compliant5 (8.2)Continuous vital signs monitoringCompliant26 (42.6)0.249Non-Compliant35 (57.4)
Almost all - 98.4 % (n = 61) of the PPH patients were in shock and treated by BLS providers (19.7 %, n = 12), ILS providers (70.5 %; n = 43) and ALS providers (9.8 %; n = 6) (Table 4). Most of the patients (68 %; n = 42) were in compensated shock with a shock index of 0.6 – 0.9. Fluid administration occurred in 55.7 % of the patients transported to health care facilities leaving 44.3 % that were transported without intravenous fluid.Table 4. Fluid administration based on shock severity for Post Partum Haemorrhage (n = 61).Table 4Shock severityNo ShockCompensated ShockMild ShockModerate ShockSevere ShockTotalFluid admin.Compliant1 (1.6)24 (39.3)8 (13.1)1 (1.6)0 (0)34 (55.7)Non-Compliant0 (0)18 (29.5)6 (9.8)3 (4.9)0 (0)27 (44.3)Total1 (1.6)42 (68.9)14 (24)4 (6.6)0 (0)61 (100)No shock: <0.6; compensated shock: 0.6 to 0.9; mild shock:1.0 to <1.4; moderate shock: 1.5 to 1.9; severe shock: 2.0.
Discussion
The study set out to analyse records regarding the response and management of PAH in KZN. Response times data was first analysed (phase 1). The mean patient age was 27 years, outside classical high-risk periods of adolescence and advanced maternal age (≥35 years) [18,19]. Despite this low-risk profile, 54 % presented with early pregnancy bleeding (<20 weeks), associated with complications such as premature birth, APH, and miscarriage [20]. Sayyad et al. [20] found that over 50 % of early pregnancy bleeding cases resulted in pregnancy loss, consistent with our finding that miscarriage accounted for 53 % of cases.
Among PAH >20 weeks, APH (10.3 %; n = 492) and PPH (4.4 %; n = 210) appeared marginal, but many cases were likely included in the “indeterminate” group (28.9 %; n = 1380), recorded only as “per vaginal bleeding.” Proper diagnosis would reclassify and increase the cases into the <20 week or >20 week groups. Diagnostic gaps across districts highlight inadequate ECC history-taking and warrant further investigation.
Most PAH cases (81.6 %, n = 3899) were transferred from clinics and CHCs to hospitals, reflecting adherence to SA’s referral system [21]. Similar patterns were reported in India [22]. Despite SA’s robust referral architecture [23], EMS coverage across sub-Saharan Africa remains limited, with fewer than one-third of countries reporting formal prehospital services [24,25].
District EMS response varied, likely due to ambulance availability, workload, and geography. King Cetshwayo had the longest PRT (39 min) and RT (79 min), with some cases exceeding 120 min, whereas uThukela had the shortest PRT (24 min) and RT (53 min), reflecting more efficient deployment. Ambulance shortages as a key contributor to prolonged PRT are consistent with other KZN studies [[11], [30]], though other contributing factors require further exploration [[12], [26]]. With 51.5 % (n = 2459) of cases exceeding 60 min (provinical norm) [27], EMS response is delayed, supporting NCCEMD reports [2,28]. Similar delays were observed in Gauteng [28], while Sierra Leone reported shorter PRTs (14 min) but similar RTs due to road and distance constraints [29].
Phase 2 findings were interpreted within the EMS phase of care, from patient loading at the referring facility to handover at the receiving facility. The first set of vital signs provided a baseline to evaluate whether interventions, such as fluid administration or ongoing monitoring, were appropriately initiated or continued during transport. Pre-transfer care was not assessed; the focus remained on identifying lapses within EMS responsibility during transfer.
This study focused on interfacility transfers (IFTs), reflecting care in a referral-based context. IFT records were selected for their completeness and confirmed diagnoses, though prior treatment cannot be assumed adequate. Many patients remained in shock during transfer, and essential interventions, such as fluid administration, were often missed, highlighting gaps in prehospital care. The cohort’s mean age was 25 years. Phase 1 described system-level response trends across all PAH types, while Phase 2 purposively focused on PPH, a leading cause of maternal death. This purposive narrowing may introduce sampling bias and limits generalisability but enabled focused clinical analysis. Prehospital care quality was assessed using five indicators benchmarked against national maternity and EMS guidelines: maternal history, blood loss estimation, initial and continuous vital signs, and intravenous fluid administration aligned to shock severity.
Most EC providers recorded an initial set of vital signs, but no further clinical assessments were documented during transport. Providers were largely non-compliant in recording maternal history, estimating blood loss, and monitoring vital signs continuously. Similar gaps were reported in another KZN IFT study, where no action was taken when patients’ conditions changed [30]. Because PPH signs such as blood loss, tachycardia, and hypotension may be masked, continuous in-transit assessment is essential for timely symptomatic treatment [31]. Delayed initiation of guideline-based PPH interventions in the prehospital setting remains a recognised contributor to preventable maternal mortality [32].
Most PPH patients (98.4 %, n = 61) transferred to higher-level facilities were in shock (Table 4), yet referring clinics did not initiate intravenous fluids in 27 (44.3 %) cases. Of these, 15 were managed by ILS and ALS providers who also failed to administer fluids despite it being within their level of care, while the remaining 12 (19.7 %) were transferred by BLS providers, who are not authorised to establish intravenous access under HPCSA regulations. Similarly, Moores [33] reported that EC providers in Timor Leste did not provide intravenous fluids during PPH IFTs. These omissions contravene national prehospital maternity care guidelines and HPCSA clinical standards [21,34].
In summary, this study found that prehospital PAH care was marked by delayed response times, with many cases exceeding recommended targets, and significant gaps in patient assessment, monitoring, and treatment. Inadequate ECC history-taking contributed to the “indeterminate” group, reflecting non-compliance or limited clinical knowledge, while documentation gaps and inconsistent adherence to EMS responsibilities highlighted systemic and clinical weaknesses.
Addressing these deficiencies requires both operational and clinical reforms. Expanding ambulance availability can reduce prolonged PRTs, and strengthening provider capacity through obstetric-focused training, guideline reinforcement, and scenario-based refreshers will improve assessment and interventions. Routine audits and supervision are also recommended to ensure consistent documentation and adherence to standards.
Strengths and limitations
This study used the largest known EMS dataset on PAH, spanning rural and urban districts, with standardised VCFs providing detailed, time-stamped operational data rarely available in obstetric EMS research. However, findings are limited to the public-sector EMS in KZN, with five districts excluded due to poor-quality records and reliance on retrospective documentation. The Phase 2 PPH sample was small and not representative of other haemorrhage types, and analyses were restricted to interfacility transfers. The absence of pre-transfer timelines and treatment histories prevented determination of the exact stage of care, so results reflect only care documented during the EMS phase.
Conclusion
This study highlights system-level inefficiencies and clinical shortcomings limiting EMS response to PAH in KZN. By targeting ambulance availability, provider skills, monitoring, and intervention practices, policymakers and EMS managers can strengthen prehospital care and align with national health guidelines. Such reforms are urgently needed to improve timeliness and quality of obstetric emergency care and reduce maternal morbidity and mortality in the province.
Author contributions: CReDiT statement
S Govender: Conceptualization, Methodology, Investigation, Resources, Writing – original draft. OP Khaliq: Project administration, Visualization, Writing - review & editing. T Abel: Data curation, Validation, Writing- review & editing. J Moodley: Supervision, Validation, Writing- review & editing.
Dissemination of results
The result of this study will be presented to the National School of Government online research presentations, KZN Provincial Emergency Medical Service Committee and the KZN College of Emergency Medical Care.
Declaration of competing interest
There is no conflict of interest to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization WHO recommendations on the assessment of postpartum blood loss and use of a treatment bundle for postpartum haemorrhage 2023 World Health Organization Genevahttps://www.who.int/publications/i/item/9789240085398[accessed 14 February 2025]38170808 · pubmed ↗
- 2National Committee for Confidential Enquiry into Maternal Deaths Saving mothers 2023: annual report of the national committee for confidential enquiry into maternal deaths in south africa for 20232024 Pretoria: Department of Health
- 3Thaddeus S.Maine D.Too far to walk: maternal mortality in context Soc Sci Med 388199410.1016/0277-9536(94)90226-71091-108042057 · doi ↗ · pubmed ↗
- 4Alam N.Chowdhury M.E.Kouanda S.The role of transportation to access maternal care services for women in rural Bangladesh and Burkina Faso: a mixed methods study Int J Gynaecol Obstet 13532016 S 45S 5010.1016/j.ijgo.2016.09.00327836084 · doi ↗ · pubmed ↗
- 5Makacha L.Mlambo R.Chikoko L.Martinez-Alvarez M.Makanga P.T.Concerning mobilising transport for accessing maternal health care and how impactful strategies are in low-resourced settings: a scoping review The Dyke 1612022142159 https://hdl.handle.net/10520/ejc-dyke_v 16_n 1_a 12
- 6Atuoye K.N.Dixon J.Rishworth A.Can she make it? Transportation barriers to accessing maternal and child health care services in rural Ghana BMC Health Serv Res 15201533310.1186/s 12913-015-1005-y 26290436 PMC 4545969 · doi ↗ · pubmed ↗
- 7Munguambe K.Boene H.Vidler M.Barriers and facilitators to health care seeking behaviours in pregnancy in rural communities of southern Mozambique Reprod Health 13Suppl 120163110.1186/s 12978-016-0141-027356968 PMC 4943506 · doi ↗ · pubmed ↗
- 8Snyman L.Coetzee S.Measuring geographic accessibility in data poor rural areas by augmenting the road network with a triangular irregular network – A case study in the O.R. Tambo District Municipality of the Eastern Cape, South Africa J Transp Geogr 103202410380810.1016/j.jtrangeo.2024.103808 · doi ↗