Successful Percutaneous Retrieval of Embolized Left Atrial Appendage Occlusion Device From Left Ventricle
Nihar Jena, Boney Lapsiwala, Gayatri Bondi, Quang Dat Ha, Yash Verma, Prabhat Singh, Hari Naga Garapati, Sreekant Avula, Rameez Sayyed, Kirit Patel

TL;DR
This paper describes a successful minimally invasive retrieval of a heart device that moved to the wrong place, avoiding the need for surgery.
Contribution
The paper presents a novel percutaneous retrieval method for embolized LAAO devices using a triple-loop snare.
Findings
An 80-year-old patient's embolized LAAO device was successfully retrieved percutaneously.
A combined transseptal and transarterial approach was used for the retrieval.
Percutaneous retrieval is a viable alternative to surgical intervention for this complication.
Abstract
The left atrial appendage occlusion (LAAO) device is a noninferior alternative to anticoagulation therapy in patients with atrial fibrillation. Device embolization is a rare but possible complication, often requiring surgical intervention specifically for left ventricular retrieval. An 80-year-old woman underwent LAAO device placement according to standard protocol, but the device embolized within a few hours. The embolized LAAO device was successfully retrieved percutaneously with a triple-loop snare using a combined transseptal and transarterial approach. The percutaneous approach highlighted in the case offers a unique, minimally invasive method for retrieving the embolized LAAO device, thereby avoiding the need for open heart surgery. LAAO device embolization is a rare potential complication that requires monitoring after the procedure. Percutaneous retrieval using a triple-loop…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
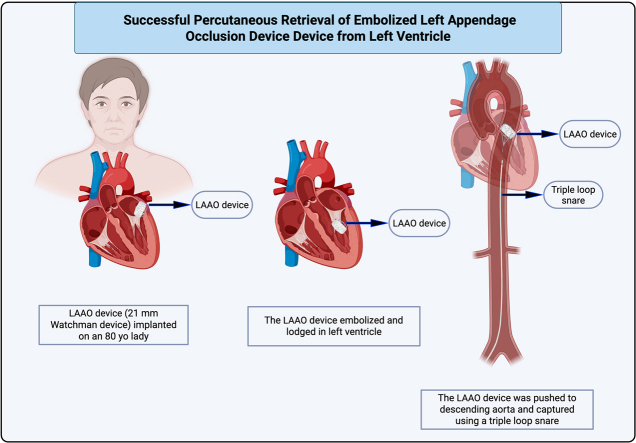 Figure 1
Figure 1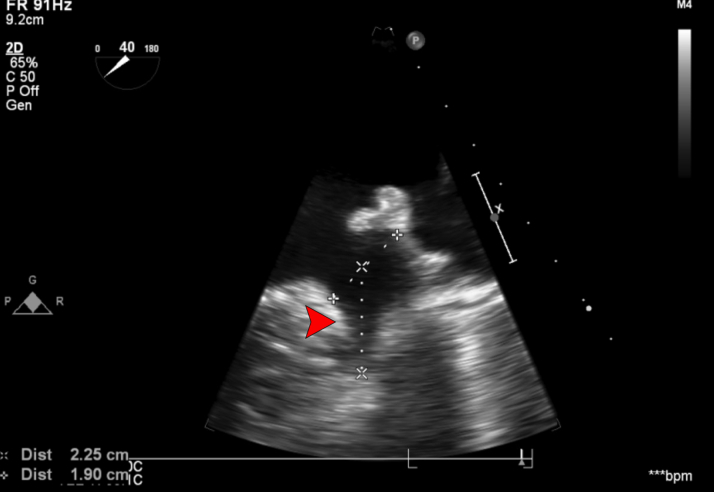 Figure 2
Figure 2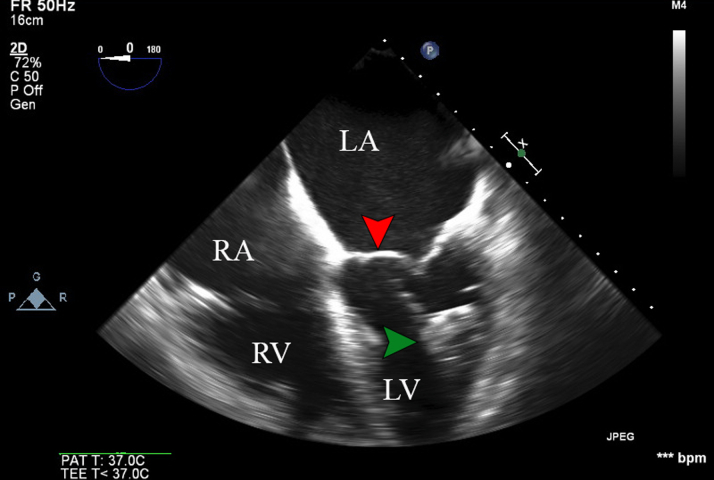 Figure 3
Figure 3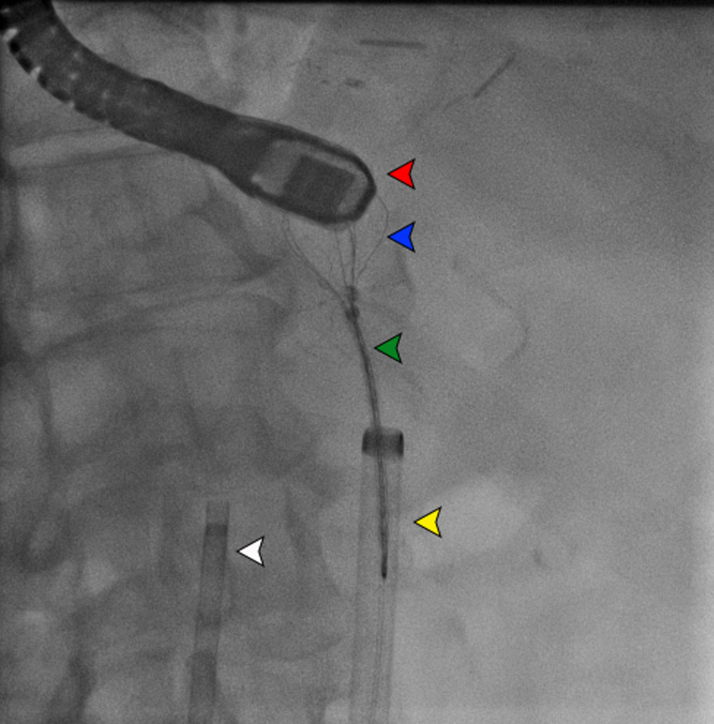 Figure 4
Figure 4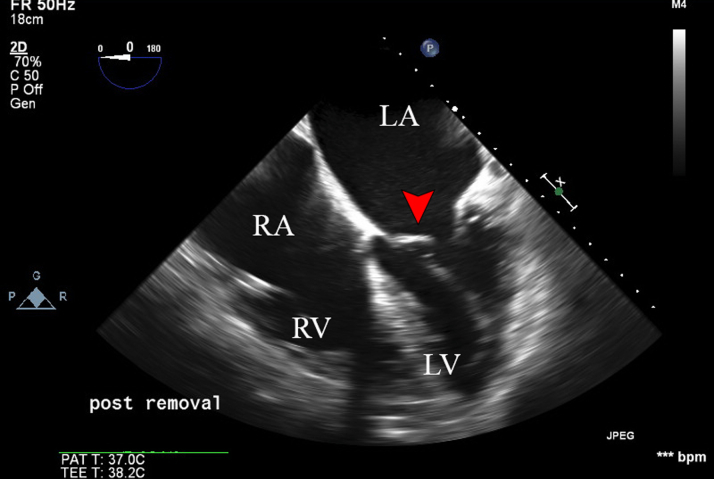 Figure 5
Figure 5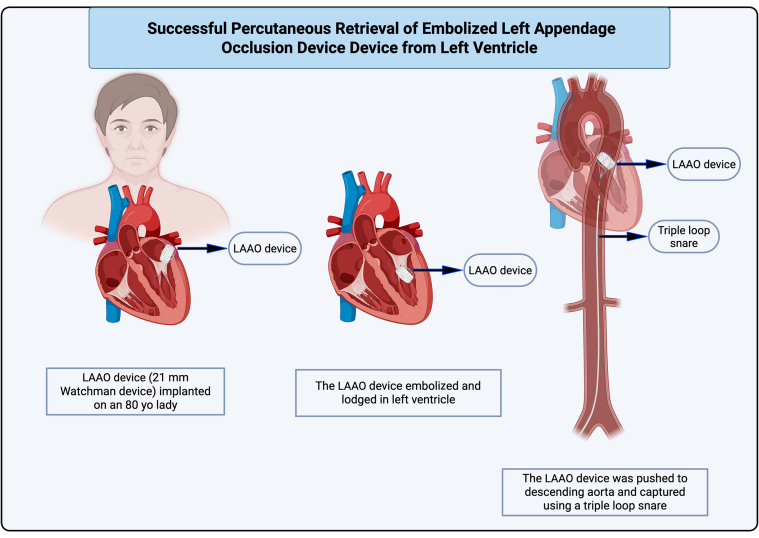 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAtrial Fibrillation Management and Outcomes · Cardiac pacing and defibrillation studies · Cardiac Arrhythmias and Treatments
History of Presentation
An 80-year-old woman was found to have frequent premature ventricular contractions on postoperative monitoring after uncomplicated 21-mm transseptal Watchman device (Boston Scientific) placement which met the PASS (position, anchoring, sizing, and sealing) criteria.1Take-Home Messages
- •High clinical suspicion and echocardiography should be used as a diagnostic modality for embolized LAAO devices.
- •The surgical approach should be the first-line management plan for hemodynamically compromised patients with device embolization.
- •Selective low-risk patients can undergo a percutaneous approach to remove the embolized device.
Past Medical History
The patient had chronic and persistent nonvalvular atrial fibrillation, a CHA_2_DS_2_-VASc score of 6 and a HAS-BLED score of 4, and was intolerant to oral anticoagulants owing to severe lower gastrointestinal bleeding. She had a prior multivessel percutaneous coronary intervention with preserved left ventricular (LV) function, diastolic heart failure (NYHA functional class III), moderate mitral regurgitation, and hypertension. Multidetector computed tomography angiogram and transesophageal echocardiography (TEE) had been performed to determine the size of the left atrial appendage occlusion (LAAO) device before the procedure. The appendage morphology was of the windsock type, with a single lobe having a maximum ostial diameter of 1.9 cm and a depth of 2.25 cm (Figure 1). The device was placed successfully, and a tug test was performed at the end.Figure 1TEE Midesophageal Short-Axis View at 40° Showing the Ostial Diameter of 1.90 cm (+) and Depth of 2.25 cm (×)The red arrowhead indicates the left atrial appendage. TEE = transesophageal echocardiography.
Investigations
The patient was monitored in the cardiac critical care unit, and she experienced frequent premature ventricular contractions. Transthoracic echocardiography revealed that the device had been embolized into the LV and wedged in the mitral subvalvular apparatus (Figure 2).Figure 2TEE Midesophageal 4-Chamber View Showing an Embolized Watchman Device (Green Arrowhead) Lodged in the Left VentricleThe red arrowhead indicates the mitral valve. LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle; TEE = transesophageal echocardiography.
Management
The patient was immediately taken to the cardiac catheterization laboratory in stable condition for attempted retrieval of the Watchman device using both anterograde and retrograde approaches. TEE confirmed that the LAAO device had migrated distally toward the papillary muscle and was wedged between the lateral wall and the papillary muscle (Figure 2).
Under ultrasound guidance, 8-F short sheaths were introduced into the right femoral artery and vein. The 8-F sheath in the right femoral vein was upgraded to a 55-cm Baylis sheath (Baylis Medical) to access the left atrium (LA) via transseptal puncture. A wire was advanced into the LA under TEE guidance. The LA opening pressure was recorded, with a mean pressure of approximately 10 to 15 mm Hg. Intravenous heparin was administered to maintain an activated clotting time of over 300 to 350 seconds. Simultaneously, a 16-F sheath was placed in the right femoral artery, with preclosure performed using Perclose sutures (Abbott Laboratories).
The Baylis sheath was then upgraded to a medium-curve DiRex sheath (Boston Scientific), which allowed for improved manipulation and access to the LV. A ThermoCool SmartTouch ablation catheter (Biosense Webster) was advanced through the DiRex sheath into the LV and was used to manipulate the device. The device was successfully freed from the lateral wall under fluoroscopic and TEE guidance and was allowed to migrate through the aortic valve into the descending aorta.
The device was subsequently captured using the EN Snare (triple-loop snare, Merit Medical) and was safely explanted through the 16-F long sheath (Figure 3). TEE showed no pericardial effusion and no valvular regurgitation (Figure 4). The patient recovered from anesthesia without neurological deficits. She had an uneventful overnight recovery and was discharged the following day on aspirin 81 mg and apixaban 5 mg twice daily. The timeline of the case is shown in Table 1. The devices used during the procedure are detailed in Table 2.Figure 3. Fluoroscopic Image Showing Aortic Snare Removal of the Embolized Watchman DeviceThe red arrowhead indicates the TEE probe; the blue arrowhead indicates the embolized Watchman device captured by snare; the green arrowhead indicates the triple-loop snare; the yellow arrowhead indicates the 16-F aortic sheath; and the white arrowhead indicates the ThermoCool ablation sheath. TEE = transesophageal echocardiography.Figure 4TEE Midesophageal 4-Chamber View After Removal of the Embolized DeviceThe red arrowhead indicates the mitral valve. Abbreviations as in Figure 2.Table 1. Timeline of the CaseTimeEventsDay of procedure/day 1An 80-year-old woman with atrial fibrillation presented for elective LAAO device placement. The device size was predetermined by TEE and CTA.Day 1Within a few hours, the device embolized to the left ventricle, which was visualized by TTE.ProcedureA transseptal and transarterial approach with a triple-loop snare was used to capture the device from the descending aorta.PostprocedureThe patient was evaluated for 2 days and discharged home.Follow-up, 1 wk, 4 wk, and 6 moShe was maintained on anticoagulation with careful monitoring of her hemoglobin levels.8 moThe patient underwent Amplatzer Amulet device placement with a successful outcome.Follow-up, 1 wk and 45 dClinically well with no complications. TEE revealed a sealed device with no evidence of thrombus.CTA = computed tomography angiogram; LAAO = left atrial appendage occlusion; TEE = transesophageal echocardiography.Table 2. List of Devices Used in the CaseDevice UsedManufacturerRole21-mm Watchman deviceBoston ScientificInitial LAAO implant55-cm Baylis sheathBaylis MedicalTransseptal access to the left atriumMedium-curve DiRex sheathBoston ScientificAccess to the left ventricleThermoCool SmartTouch ablation catheterBiosense Webster (Johnson & Johnson)Manipulated embolized device in the left ventricle16-F long arterial sheathCordisTransarterial access for snare retrievalPerclose suturesAbbottPreclosure of the femoral arterial access siteAmplatzer Amulet deviceAbbott LaboratoriesAbbott LaboratoriesLAAO = left atrial appendage occlusion.
Follow-Up
The patient was evaluated at 1 week, 4 weeks, and 6 months postprocedure, and she was maintained on anticoagulation therapy while being monitored for hemoglobin levels. Later, she underwent a successful Amplatzer Amulet device (Abbott Laboratories) placement without complications. The device was chosen given the appendage's wider ostium and borderline depth. Its lobe and disc design allowed for more stable anchoring compared with the depth-dependent anchoring of the Watchman device.
Discussion
An LAAO device is widely recognized as an effective alternative to oral anticoagulation in atrial fibrillation, particularly in patients with an elevated risk of bleeding. Although rare, inadvertent device embolization is a known, potentially life-threatening complication of the procedure.2 According to the National Cardiovascular Data Registry's LAAO Registry, 30 embolizations (0.07%) were reported between 2016 and 2021. Systematic reviews have shown the incidence of device embolization to range from 0% to 2% of all procedures.3^,^4 One-third of these cases occurred early, during the procedure itself, while the remaining two-thirds occurred postprocedure, during hospitalization.3 Clinical presentations vary widely, from asymptomatic to severe cardiogenic shock. For example, Aminian et al5 described a case presenting 1 month postprocedure with acute pulmonary edema and cardiogenic shock due to embolization of the Amplatzer cardiac plug into the left ventricle. In another case, Bhagat et al6 reported the asymptomatic delayed embolization of a Watchman FLX device, diagnosed via follow-up transthoracic echocardiography 35 days after implantation.
Regular practice of PASS criteria has been shown to reduce embolization events. In the current case, the device was secured properly using PASS criteria, but it embolized within a short period. Several factors may contribute to device migration, including improper sizing, suboptimal placement, and vigorous tug testing.1 The most common embolization sites include the descending aorta (30%), LA (24%), and LV (20%).4 Although prompt device removal is crucial, the embolization site significantly influences the choice of retrieval technique and the associated procedural morbidity. Percutaneous retrieval is the preferred approach for devices embolized to the aorta or LA. However, percutaneous extraction from the LV has traditionally been considered unfeasible given the risk of injury to the surrounding structures, particularly the mitral and aortic valves.7 Consequently, surgical extraction from the LV is often required, although it carries a risk of significant complications.
Few cases of LAAO device embolization and subsequent retrieval have been reported. Ferraris et al8 described a case involving embolization to the atrial side of the mitral valve, which was successfully retrieved percutaneously using a double-snare technique. In a literature review, Aminian et al9 found that 80% of reported Watchman device embolizations to the LV were managed surgically. Since then, there has been a rise in the number of emergent surgical retrievals. For instance, Birmingham et al7 documented a case of mitral valve embolization that required emergent open heart surgery after multiple failed percutaneous attempts and 2 episodes of pulseless electrical activity. Additionally, Ceresa et al10 recently described a case of intraoperative device embolization to the ventricular side of the anterior mitral leaflet, which required surgical intervention after failed percutaneous snare retrieval.
To date, a few successful percutaneous retrievals of embolized LAAO devices from the LV have been reported. Spilias et al1 described a case in which an LAAO device was retrieved from the LV using a transarterial approach and a single snare after failed attempts via a transseptal route. In our case, the LAAO device was found wedged between the lateral wall and the papillary muscle. Our strategy involved gentle manipulation to free the device from the surrounding structures, effectively converting a complex LV embolization into a simple embolization. The EN Snare system, equipped with a triple-loop snare offering a higher probability of foreign body capture compared with a single-loop design, was positioned in the descending aorta to safely retrieve the device once it moved from the LV into the aorta.
We describe a novel percutaneous approach that successfully avoided major surgery, its associated complications, and prolonged postoperative recovery. The previously published peer-reviewed articles on embolized LAAO devices are summarized in Supplemental Table 1.
Conclusions
Device embolization is a rare but life-threatening complication of LAAO. Although retrieval from the aorta and LA can be percutaneous, a surgical approach is often required for LV device entrapment. This case study demonstrates that a percutaneous snare technique can be a viable and safe approach for retrieving an embolized LAAO device from the LV in centers with limited access to cardiothoracic surgery. Notably, the use of triple-snare loops played a key role in securing and extracting the device effectively, providing enhanced control and stability during retrieval. Although the use of multiple-snare loops appears effective, further research is necessary to fully evaluate the safety, potential complications, and procedural nuances. Continued study will help refine the technique and guide its broader application in future cases.Visual SummaryIllustration of Case PresentationThe images were created using Biorender.com.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spilias N.Kochar A.Patel J.Saliba W.Kapadia S.Percutaneous retrieval of a watchman device from the left ventricle using a transarterial approach JACC Case Rep 1520198768833431695010.1016/j.jaccas.2019.11.029PMC 8288985 · doi ↗ · pubmed ↗
- 2Osmancik P.Tousek P.Herman D.Interventional left atrial appendage closure vs novel anticoagulation agents in patients with atrial fibrillation indicated for long-term anticoagulation (PRAGUE-17 study)Am Heart J 1832017 Jan 1081142797903410.1016/j.ahj.2016.10.003 · doi ↗ · pubmed ↗
- 3Asmarats L.Rodés-Cabau J.Percutaneous left atrial appendage closure: current devices and clinical outcomes Circ Cardiovasc Interv 10112017 e 00535910.1161/CIRCINTERVENTIONS.117.00535929146668 · doi ↗ · pubmed ↗
- 4Lakkireddy D.Left atrial appendage occlusion device embolization (the LAAODE study): understanding the timing and clinical consequences from a worldwide experience J Atr Fibrillation 135202125163495034410.4022/jafib.2516 PMC 8691350 · doi ↗ · pubmed ↗
- 5Aminian A.Chouchane I.Compagnie M.Decubber M.Lalmand J.Delayed and fatal embolization of a left atrial appendage closure device Circ Cardiovasc Interv 7420146286302513908910.1161/CIRCINTERVENTIONS.114.001546 · doi ↗ · pubmed ↗
- 6Bhagat A.A.Gier C.Diggs P.Gursoy E.C.Delayed embolization of watchman FLX closure device in an asymptomatic patient J Am Coll Cardiol 8182023400310.1016/j.hrcr.2023.05.014PMC 1051189337746578 · doi ↗ · pubmed ↗
- 7Birmingham K.P.Moawad N.Garibo R.B.Rose D.Surgical retrieval of a left atrial appendage closure device (Watchman TM) following embolization into the mitral valve Cardiol Plus 442019125127
- 8Ferraris F.Millesimo M.Anselmino M.Successful percutaneous retrieval of an embolized left atrial appendage occluder JACC Case Rep 424202210168910.1016/j.jaccas.2022.101689 PMC 984723836684032 · doi ↗ · pubmed ↗