Recurrent Embolic Strokes in Mechanical Aortic Valve: Diagnostic and Management Challenges
Pernille G. Eriksen, Dorte Damgaard, Mariann Tang, Jonas A. Povlsen, Jesper Møller, Bjarne L. Nørgaard, Ivy S. Modrau

TL;DR
A patient with a mechanical aortic valve had repeated strokes with no clear cause, leading to a rare diagnosis of valve thrombosis and successful treatment.
Contribution
Highlights the diagnostic challenges and management of rare mechanical valve thrombosis causing recurrent strokes.
Findings
Recurrent strokes occurred despite inconclusive tests and subtherapeutic anticoagulation.
Fluoroscopy and CT revealed leaflet opening restriction, leading to surgical confirmation of valve thrombosis.
Valve replacement and left atrial appendage occlusion resulted in no further events at 8-month follow-up.
Abstract
Recurrent embolic strokes without an identifiable source in patients with mechanical heart valves pose a significant diagnostic challenge. A 59-year-old woman with a mechanical aortic valve experienced recurrent embolic strokes, the first nearly 7 years after implantation during subtherapeutic anticoagulation. Repeated neurologic and cardiac imaging, thrombophilia screening, and prolonged rhythm monitoring failed to identify a definitive embolic source. Fluoroscopy and computed tomography showed discrete leaflet opening restriction. Multifocal infarctions raised clinical suspicion for mechanical valve thrombosis, prompting surgical exploration that confirmed diagnosis. The valve was replaced with a bioprosthesis, and left atrial appendage occlusion was performed. The patient remained event-free at 8-month follow-up. Mechanical valve thrombosis is rare and often undetectable. This case…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
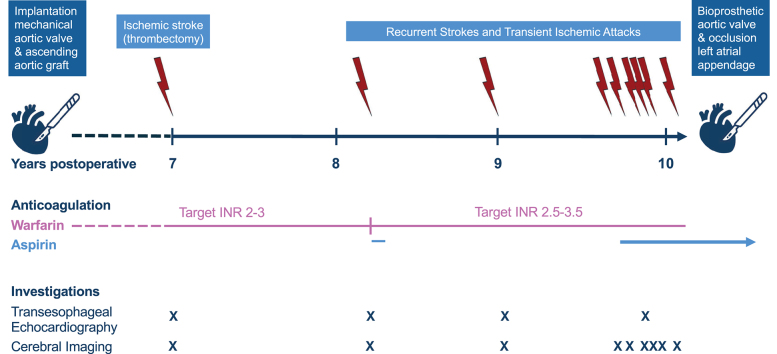 Figure 1
Figure 1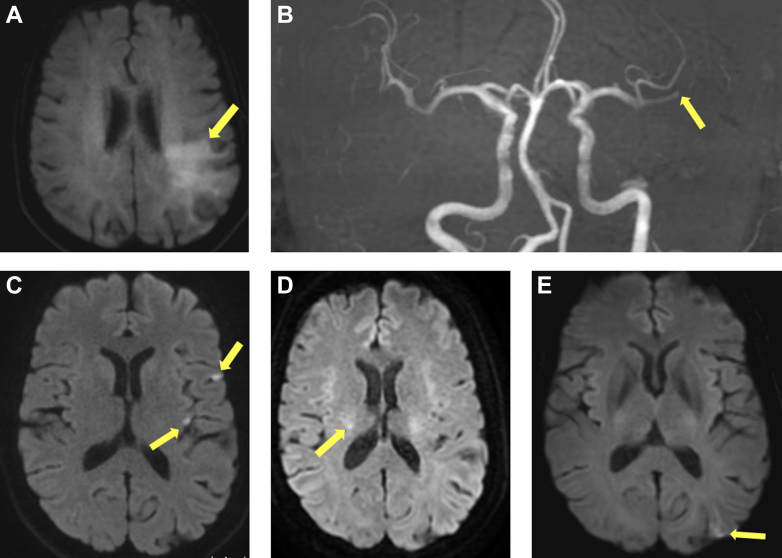 Figure 2
Figure 2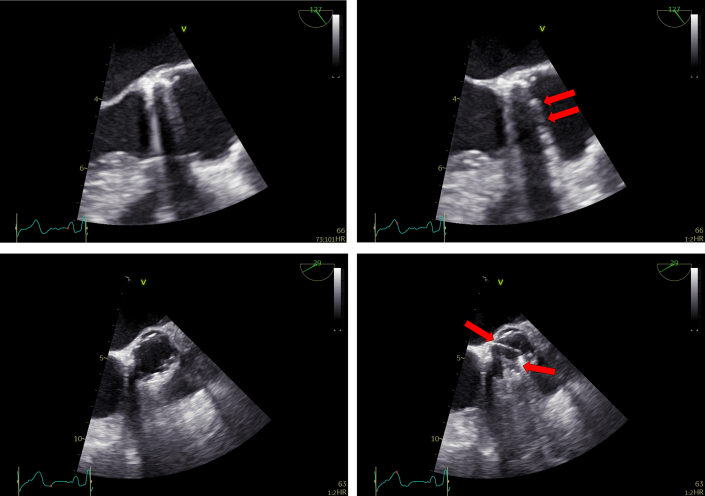 Figure 3
Figure 3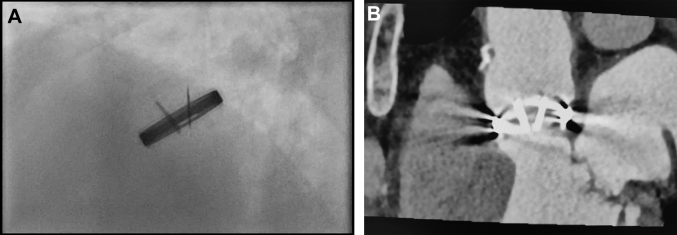 Figure 4
Figure 4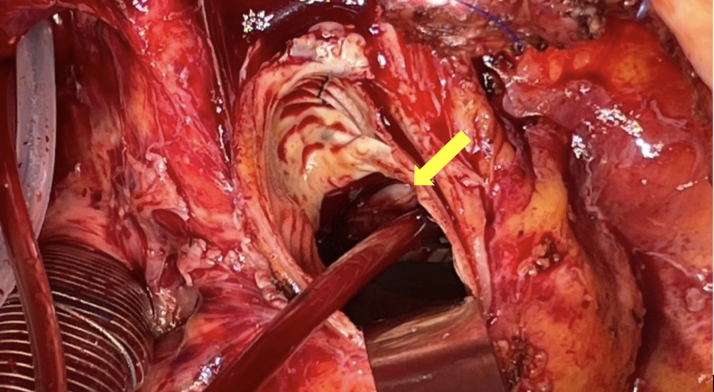 Figure 5
Figure 5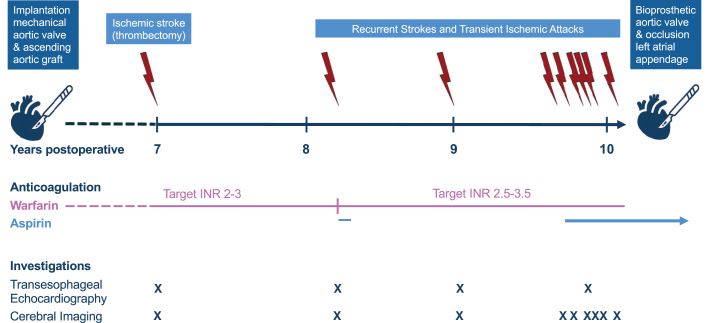 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Infective Endocarditis Diagnosis and Management · Aortic Disease and Treatment Approaches
History of Presentation
A 59-year-old woman with a mechanical aortic valve presented with a series of recurrent cerebral thromboembolic events beginning nearly 7 years after valve implantation. The initial stroke occurred in the setting of subtherapeutic anticoagulation (international normalized ratio [INR]: 1.4) and resolved completely after successful recanalization with thrombectomy. Over the next 3 years, the patient experienced further 8 cerebral thromboembolic events despite sustained—and later intensified—anticoagulation treatment. Vital signs, including blood pressure, remained stable throughout. After a cluster of recurrent events, redo valve replacement was pursued based on clinical suspicion of mechanical valve thrombosis, despite a lack of definitive imaging evidence.Take-Home Messages
- •Current noninvasive cardiac imaging often fails to detect small, nonobstructive thrombi on mechanical aortic valves.
- •Recurrent embolic events despite negative imaging warrant individualized evaluation by a multidisciplinary team and consideration of surgical intervention.
Past Medical History
Ten years before presentation, the patient underwent implantation of a 22-mm bileaflet mechanical aortic valve (ATS Open Pivot AP, advancing the standard; ATS Medical Inc) and a 26-mm ascending aortic tube graft for stenotic bicuspid valve with ascending aortic dilation. Cardiovascular risk factors included medically treated hypertension and hypercholesterolemia. She developed intermittent left bundle branch block, which later became persistent. Cardiac computed tomography excluded coronary artery disease; left ventricular ejection fraction remained preserved. Other comorbidities included nonpharmacologically managed intermittent depression, psoriatic arthritis treated with methotrexate, chronic back pain, and prior lumbar discectomy.Figure 4. Thrombotic Material on Aortic Annulus After Valve ExplantationIntraoperative image of the aortic annulus after explantation of the mechanical aortic valve, revealing consolidated thrombotic material involving approximately one-third of the annular circumference.
Differential Diagnosis
Key differential diagnoses include mechanical valve thrombosis, atrial fibrillation, infective endocarditis, thrombophilia and other hypercoagulable states, paradoxical embolism, aortic dissection, mural thrombus, large-vessel atherosclerosis, and cryptogenic stroke.
Investigations
Repeated brain magnetic resonance imaging revealed multifocal ischemic lesions (Table 1, Figure 1). Serial transthoracic echocardiography (TTE) and transesophageal echocardiography (TEE) (Video 1), as well as electrocardiogram (ECG)-gated multidetector cardiac computed tomography (MDCT), showed no evidence of prosthetic obstruction, pannus, or thrombus (Figure 2). MDCT was performed with a dual source computed tomography scanner (Siemens Somatom Force) using an ECG-gated full-cycle retrospective protocol and high tube voltage (140 kV) to counteract valve artifacts. However, cinefluoroscopy (Video 2) and MDCT (Video 3) were consistent in showing a 10° reduction in opening angle of one leaflet, raising concern for subtle mechanical restriction (Figure 3). Repeated ECGs and extended Holter monitoring confirmed sustained sinus rhythm. Duplex ultrasound and computed tomography angiography showed no evidence of carotid artery disease. Thrombophilia and coagulation testing were unremarkable. Despite this comprehensive work-up, the embolic source remained undetermined until mechanical valve thrombosis was confirmed intraoperatively.Table 1. Clinical Timeline and Diagnostic-Therapeutic CourseEvent No.Time PointClinical EventPresenting SymptomsDiagnostic Work-UpInterventionCardiacCerebralOtherBaselineMechanical aortic valve replacement (22 mm) and ascending aortic tube graft (26 mm)Lifelong warfarin—target INR 2-3Self-management training1+6 y, 9 moIschemic strokeINR: 1.4Aphasia, right-sided hemisensory deficitsTEE: UnchangedNo signs of valve thrombosisBrain MRI:
- 1.Thrombus in a left M2 segment
- 2.Diffusion restriction in left insular and parietal cortex 24-hour brain MRI: 3 small DWI lesions in the same regionECG: SR, LBBBThrombectomy (recanalization)LMWH bridgingWarfarin continued—target INR 2-3Stroke rehabilitation2+8 y, 3 moClinical suspicion of TIATransient paresthesia left arm followed by right-sided headacheTEE: UnchangedNo signs of valve thrombosisBrain MRI: No diffusion restrictionsTranscranial Doppler: Microembolism in right intracranial arteriesCarotid US: Minor plaque in the proximal left ICAECG: SR, narrow QRS complexesSuppl. aspirin for 1 month (75 mg daily)Warfarin—target INR 2.5-3.53+9 yClinical suspicion of TIAParesthesia left armTTE: Normal aorta valve prosthesisTEE: Unchanged. No signs of valve thrombosisMyocardial perfusion imaging: NormalBrain MRI: Silent punctate diffusion restriction in the left medial temporal lobeMRA cervical and intracerebral arteries: NormalTranscranial Doppler: Microembolism in right intracranial arteriesECG: SR, narrow QRSHolter monitoring: SR, rare PAC and PVCWarfarin continued4+9 y, 8 moClinical suspicion of TIATransient right leg motor impairment with foot dropBrain CT: No acute findingsCarotid US: No significant carotid stenosisECG: SR, LBBBWarfarin continued5+9 y, 10 moClinical suspicion of TIAAcute-onset headache, transient weakness, and paresthesia right legBrain CT: NormalECG: SR, LBBBWarfarin continued6+9 y, 11 moIschemic strokeAcute-onset frontal headache with paresthesia right legBrain CT: No acute findingsBrain MRI: 3 silent cortical diffusion restrictions in the left hemisphereECG: SR, LBBB7+9 y, 11 moIschemic stroke24-hour before admission: transient right visual field defectAt admission: transient left upper extremity weakness, left-sided paresthesia, dysarthria, and lip tinglingTTE: Normal aortic valve prosthesisTEE: Unchanged. No signs of valve thrombosisMultidetector cardiac CT and fluoroscopy: Both discs mobile but 10° angle differenceBrain MRI: 2 punctate diffusion restrictions in left occipital and frontal regions. Microbleed in right thalamus and left frontal regionCT angiography of carotid and intracerebral arteries: NormalECG: SR, LBBBHolter monitoring: SR, rare PVCThrombophilia work-up deferred—no impact on managementWarfarin continuedSuppl. low-dose aspirin for 1 month+9 y, 11 moMultidisciplinary Team Conference8+9 y, 11 moIschemic strokeLeft-sided hemiparesis and facial paresis, dysarthriaBrain MRI: Punctate diffusion restriction in rightcorona radiataECG: SR and LBBBThrombophilia work-up: NormalWarfarin continuedAspirin continued for 3 months+10 ySecond opinion at a University Hospital, Department of Neurology9+10 y, 1 moIschemic strokeRight homonymous hemianopiaBrain MRI: Cortical diffusion restriction in left hemisphereWarfarin and aspirin continued+10 y, 2 moBioprosthetic aortic valve (21 mm) and prophylactic occlusion left atrial appendageCardiacRehabilitationLifelongAspirin therapyCT = computed tomography; DWI = diffusion-weighted imaging; ECG = electrocardiogram; ICA = internal carotid artery; INR = international normalized ratio; LBBB = left bundle branch block; LMWH = low molecular weight heparin; M2 = 2nd segment of the middle cerebral artery; MRA = magnetic resonance angiography; MRI = magnetic resonance imaging; PAC = premature atrial contraction; PVC = premature ventricular contraction; SR = sinus rhythm; TEE = transesophageal echocardiogram; TIA = transient ischemic attack; TTE = transthoracic echocardiogram; US = ultrasound.Visual SummaryTimeline of EventsTimeline of clinical events, anticoagulation adjustments, and diagnostics after mechanical valve implantation, ending with redo valve replacement and left atrial appendage occlusion. Arrows = key events; x = diagnostic test.Figure 1. Brain Magnetic Resonance Imaging demonstrating Recurrent Multifocal Ischemic EventsBrain magnetic resonance imaging (MRI) demonstrating multifocal ischemic events during the clinical course. A and B correspond to the initial stroke; C to E represent selected imaging from transient ischemic attack 5, 7, and 8. (A) Diffusion-weighted MRI showing acute ischemia in the left insular and parietal cortex. (B) MRI (time-of-flight angiography) demonstrating thrombus in the left M2 segment. (C) MRI revealing 2 of 3 silent cortical infarcts in the left hemisphere. (D) MRI showing punctate diffusion restriction in the right corona radiata. (E) MRI showing cortical diffusion restriction in the left hemisphere. M2 = 2nd segment of the middle cerebral artery.Figure 2. Transesophageal EchocardiographyHigh-esophageal long-axis views (upper panels) and short-axis views (lower panels) are displayed in diastole (left panels) and systole (right panels). The red arrows highlight symmetric disk motion. Leaflet mobility is preserved, with no paravalvular leak or other evidence of prosthetic valve dysfunction.
Management
After mechanical valve replacement, the patient initiated lifelong warfarin with self-managed anticoagulation targeting an INR of 2.0 to 3.0. Approximately 1 year before the initial stroke, depressive symptoms led to inconsistent INR monitoring and subtherapeutic control despite a continued fixed-dose regimen.
After this stroke, she received re-education in self-management. Recurrent cerebral thromboembolic events occurred despite therapeutic anticoagulation, prompting escalation of the INR target to 2.5 to 3.5 and addition of low-dose aspirin, in line with current guidelines.1
Multifocal ischemic lesions across distinct vascular territories suggestive of a cardioembolic source prompted the multidisciplinary team to recommend redo surgery. The decision followed a shared decision-making process with active patient involvement based on the clinical suspicion of mechanical valve thrombosis despite inconclusive evidence.
Surgical re-exploration involved replacement of the mechanical valve with a bioprosthetic valve and prophylactic left atrial appendage occlusion. Intraoperative inspection showed normal valve function and a subvalvular thrombus involving approximately one-third of the annular circumference (Figure 4), confirmed by histopathology. Postoperatively, warfarin was discontinued and low-dose aspirin monotherapy maintained.Figure 3. Fluoroscopic and CT Evaluation of the Implanted Bileaflet Mechanical ValveFluoroscopic (A) and multidetector computed tomography (B) assessment of the implanted bileaflet mechanical valve. Both imaging modalities revealed reduced leaflet opening, with one leaflet at 60° to 65° and the other at 70° to 75°. According to the manufacturer, the leaflets open to 85° when fully functional, whereas normally functioning ATS valves in vivo open to approximately 70°,10 highlighting the subtle restriction of the first leaflet.
Outcome and Follow-Up
Recovery was uneventful except for complete heart block requiring permanent pacemaker implantation 14 days postoperatively. TTE demonstrated a well-functioning bioprosthetic aortic valve, preexisting mild mitral regurgitation, and preserved ventricular function.
Eight months postoperatively, the patient had completed cardiac rehabilitation and remained free of thromboembolic events. Aspirin monotherapy was maintained.
Discussion
This case illustrates the complexity of diagnosing mechanical valve thrombosis and managing recurrent cerebral thromboembolic events in patients with mechanical aortic valves. Although the initial ischemic stroke occurred during a period of subtherapeutic anticoagulation, it was followed by multiple thromboembolic events despite sustained therapeutic INR and escalation of antithrombotic treatment.
Repeated cardiac imaging failed to reveal definitive thrombus despite increasing clinical suspicion of cardioembolic events. Diagnosis was ultimately confirmed intraoperatively, underscoring limitations of current imaging modalities.
Mechanical valve thrombosis is an uncommon but potentially life-threatening cause of thromboembolism and acute valve dysfunction, with thromboembolic events occurring in approximately 5% of patients with mechanical aortic valves, with the highest risk occurring in the early postoperative period.2 Limitations of current imaging modalities remain a central challenge in the timely diagnosis and management of mechanical valve thrombosis. Although TEE remains the gold standard for prosthetic valve assessment, it often fails to directly visualize thrombus. Diagnosis frequently relies on indirect findings, including restricted leaflet motion, abnormal transvalvular flow pattern, elevated gradients, or central regurgitation.3 Sensitivity is particularly limited for detecting small, nonobstructive thrombi in mechanical aortic valve prostheses, with reported miss rates of 17% to 50% and up to 80% for TTE.3^,^4 Technical factors such as acoustic shadowing, suboptimal leaflet visualization, and difficulty distinguishing thrombus from pannus or imaging artifacts contribute to limitations.4
In the present case, repeated TTE, TEE, and supplemental MDCT failed to identify the thrombus despite increasing clinical suspicion of a cardiac embolic source. This underscores the limited sensitivity of current cardiac imaging modalities due to spatial resolution constraints and imaging artifacts.4, 5, 6 The present subvalvular thrombus was circumferential and closely adherent to the annular wall, which likely contributed to its being overlooked. Retrospectively, the subtle reduction in one leaflet's opening observed on fluoroscopy and MDCT—though not confirmed intraoperatively—may have warranted greater diagnostic consideration.3^,^6
The therapeutic implications of these diagnostic challenges are significant. Current European guidelines recommend redo surgery primarily for obstructive mechanical valve thrombosis or embolism associated with thrombi larger than 10 mm but offer limited guidance for nonobstructive thrombi or cumulative embolic burden.1 This gap may prolong exposure to thromboembolic risk due to diagnostic uncertainty and hesitancy to deviate from established treatment algorithms. Recurrent strokes in this patient resulted in multiple acute hospital admissions and substantial distress and anxiety, reflecting an existential threat despite the absence of persistent neurologic deficits. These limitations highlight the need for a more nuanced, risk-adapted approach beyond existing guideline thresholds. Clinicians should recognize these diagnostic limitations, maintain a high index of suspicion, and engage a multidisciplinary team involving cardiology, neurology, and cardiac surgery with coagulation experts consulted as needed. Shared decision-making with the patient should incorporate embolic history, individualized risk-benefit analysis, and quality-of-life considerations to inform patient-centered management.
The initial ischemic stroke occurred during a period of depressive mood that compromised the patient's otherwise well-managed self-anticoagulation, resulting in subtherapeutic INR. Although self-management of warfarin has been associated with improved time in therapeutic range and reduced thromboembolic complications in selected patients, its effectiveness relies on adherence and psychological stability. In patients with mechanical heart valves, nonadherence remains a major contributor to adverse events, with depression and insufficient knowledge about anticoagulation identified as key risk factors.7 Consequently, it has been proposed that routine evaluation of both adherence and mental health should be integrated into the follow-up of patients on long-term warfarin therapy to ensure safe and effective anticoagulation.7
Reluctance to pursue redo aortic valve replacement may reflect overestimation of the surgical risk. However, excluding infective endocarditis, contemporary data show excellent outcomes, with operative mortality as low as 2.5% and pacemaker implantation rates below 4%.8 In series reporting higher mortality, the primary determinants of adverse outcomes were endocarditis and operative urgency.9 This supports earlier surgical consideration in patients with recurrent embolic events and acceptable surgical risk, particularly when medical therapy has been exhausted.
Conclusions
Nonobstructive thrombosis of mechanical aortic valves remains a diagnostic challenge due to the limited sensitivity of current imaging modalities. In cases of recurrent embolic events with inconclusive work-up, sustained clinical suspicion of a cardiac source should prompt multidisciplinary team evaluation with active patient involvement. Shared decision-making may support surgical re-exploration to secure a definitive diagnosis and prevent further embolic complications.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Vahanian A.Beyersdorf F.Praz F.2021 ESC/EACTS guidelines for the management of valvular heart disease: developed by the task force for the management of valvular heart disease of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS)Eur Heart J 432022561632
- 2Korteland N.M.Fiocco M.Bekkers J.A.Mechanical aortic valve replacement in non-elderly adults: meta-analysis and microsimulation Eur Heart J 382017337033772904564710.1093/eurheartj/ehx 199 · doi ↗ · pubmed ↗
- 3Kim J.Y.Suh Y.J.Han K.Kim Y.J.Choi B.W.Diagnostic value of advanced imaging modalities for the detection and differentiation of prosthetic valve obstruction: a systematic review and meta-analysis JACC Cardiovasc Imaging 122019218221923077223610.1016/j.jcmg.2018.11.033 · doi ↗ · pubmed ↗
- 4Daniel W.G.Erbel R.Kasper W.Comparison of transthoracic and transesophageal echocardiography for detection of abnormalities of prosthetic and bioprosthetic valves in the mitral and aortic positions Am J Cardiol 711993210215842198510.1016/0002-9149(93)90740-4 · doi ↗ · pubmed ↗
- 5Symersky P.Schaefer-Prokop C.M.Mollet N.R.Prospective ECG triggering reduces prosthetic heart valve-induced artefacts compared with retrospective ECG gating on 256-slice CT Eur Radiol 222012127112772220544610.1007/s 00330-011-2358-1PMC 3348472 · doi ↗ · pubmed ↗
- 6Jiménez C.E.S.Papolos A.I.Kenigsberg B.B.Management of mechanical prosthetic heart valve thrombosis: JACC review topic of the week J Am Coll Cardiol 812023211521273722536610.1016/j.jacc.2023.03.412 · doi ↗ · pubmed ↗
- 7Park S.Jang I.Factors affecting medication adherence in patients with mechanical heart valves taking warfarin: the role of knowledge on warfarin, medication belief, depression, and self-efficacy Int J Environ Res Public Health 182021521410.3390/ijerph 1810521434068932 PMC 8156383 · doi ↗ · pubmed ↗
- 8Kang Y.Lee S.Kim H.Recent outcomes of surgical redo aortic valve replacement in prosthetic valve failure Thorac Cardiovasc Surg 7320252792873844291610.1055/a-2281-1897 PMC 12115537 · doi ↗ · pubmed ↗