Is Micronucleus Assay a Suitable Biomarker for Evaluating the Cancer Risk in Professionals Exposed to Antineoplastic Drugs? A Systematic Review
Thiago Guedes Pinto, Lorrany da Silva Avanci, Gabriel Carvalhal de Aguiar, Daniel Vitor de Souza, Patricia Ramos Cury, Ana Claudia Muniz Renno, Daniel Araki Ribeiro

TL;DR
This paper reviews whether the micronucleus assay can be used to assess cancer risk in healthcare workers exposed to anticancer drugs.
Contribution
It systematically evaluates the reliability of the micronucleus assay as a biomarker for genotoxic effects in professionals handling antineoplastic drugs.
Findings
23 out of 28 studies observed genotoxic effects linked to anticancer drugs.
The micronucleus assay is suggested as a suitable biomonitoring tool for assessing cancer risk in exposed professionals.
Most studies were of high quality, supporting the reliability of the findings.
Abstract
The widespread use of antineoplastic drugs in cancer treatment has led to significant concerns regarding the potential health risks posed to healthcare professionals involved in the preparation, administration, and handling of these chemical compounds, including genotoxicity. This systematic review investigates the genotoxicity of various anticancer drugs through the micronucleus assay in mammalian cells through a comprehensive analysis of studies retrieved from PubMed, SCOPUS, and Web of Science. A systematic search conducted in May 2025 identified 28 relevant studies, all of which employed the micronucleus assay. The results indicated that 23 of the reviewed studies observed genotoxic effects linked to several drugs. As for the quality assessment, all studies (but one) were categorized as either strong or moderate; therefore, we consider our findings to be reliable. These findings…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
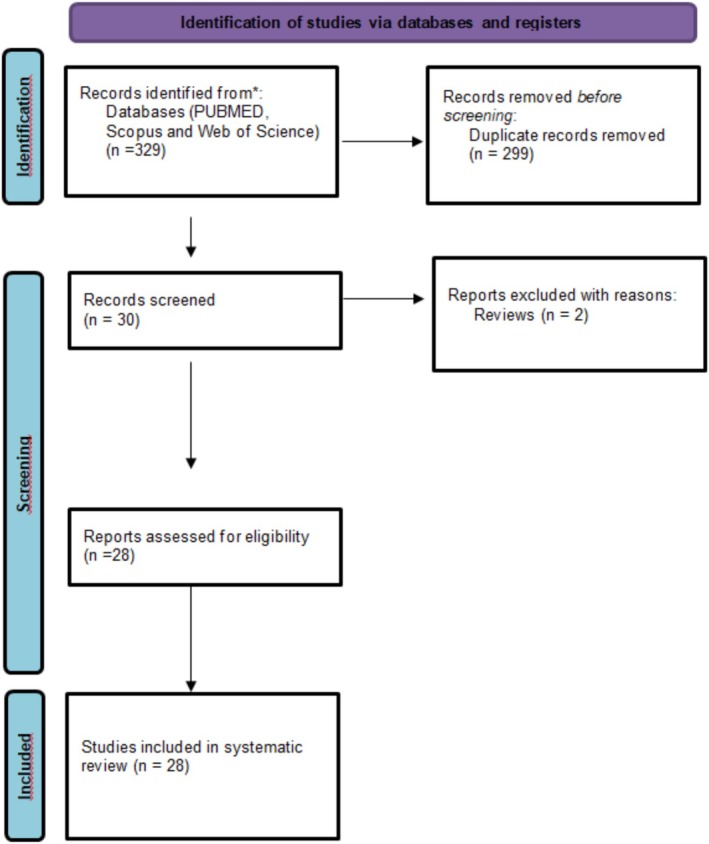 FIGURE 1
FIGURE 1| Electronic databases used | Search strategy (May, 2025) |
|---|---|
|
PubMed Web of Science
| (oncologic drugs) OR (chemotherapeutic drugs) OR (anticancer drugs) AND (DNA Damages) OR (Damage, DNA) OR (Damages, DNA) OR (DNA Injury) OR (DNA Injuries) OR (Injuries, DNA) OR (Injury, DNA) OR (Genotoxic Stress) OR (Genotoxic Stresses) OR (Stresses, Genotoxic) OR (Genotoxicity) OR (Mutagenicity) OR (micronucleus assay) (micronucleated cell) AND (mammalian) OR (mammalian cells). |
| Author | Year of publication | Country | Type of drug | Exposure period/time | Exposure dosages |
|---|---|---|---|---|---|
| Ness et al. |
| Brazil | Not informed |
Mean: 96 months Daily occupational exposure load of at least 6 h | Not informed |
| Pajic et al. |
| Serbia |
Bleomycin sulfate Mitomycin Daunorubicin Actinomycine Aminouracil mustard Metotrexate Mercaptopurine Cladribin Teniposide Vinblastine Vincristine Bisulfan Chlorambucil Cisplatin Procarbazine Streptozocin Tamoxifen citrate |
Daily: 1–6 h average Continually for 5–30 years | Not informed |
| Aristizabal‐Pachon; Castillo, |
| Colombia |
Bleomycin Carboplatin Cyclophosphamide cisplatin Doxorubicin Fluorouracil Pacli taxel |
Exposure time (months): 41.10 ± 23.6 Exposure by day (hours) < 4 ( 24 individuals with less than 42 months and 16 individuals with 42 or more months. | Not informed |
| Santos et al. |
| Brazil |
Cyclophosphamide Ifosfamide |
Hours/day: 6.43 ± 0.25 Months worked: 43.95 ± 5.78 h of daily exposure Pharmacists: 5.60 ± 1.85 Hours of daily exposure: Nurses: 7.33 ± 0.95 Months of exhibition Pharmacists: 45.41 ± 41.20 Months of exhibition– Nurses: 41.70 ± 38.96 | Not informed |
| Ursini et al. |
| Italy |
5‐Fluorouracil Cytarabine gemcitabine Azacytidine Daunorubicin doxorubicin Epirubicin |
Group exposed—Administrator antineoplastic: 15.6 ± 7.3 years Preparators antineoplastic: 18.4 ± 10.2 years | Not informed |
| Mahmoodi et al. |
| Iran |
Taxol Taxoter Methotrexate Cisplatin Carboplatin Adriamycin 5‐Fluorouracil Vincristine Cyclophosphamide Melphalan Actinomycin Ifosfamide Andoxal Gemzar Mebtra Velcade Busolfan Cyclosporin Oxaloplatin Vepside Doxorubicin Bleomycin sulfate | Job duties handling chemotherapy for the past 6 months | Not informed |
| Ladeira et al. |
| Portugal | 5‐Fluorouracil | Years of employment: 6.01 (mean ± SD, year) Range 0.17–30 | Not informed |
| Mrđanović et al. |
| Serbia |
Cyclophosphamide Etoposide Cisplatin Doxorubicin Mitomycin c 5‐Fluorouracil Methotrexate Vincristine Carboplatin Paclitaxel | Exposure time to cytostatics: 10 years | Not informed |
| Villarini et al. |
| Italy |
5‐Fluorouracil Cytarabine Cyclophosphamide Gemcitabine Ifosfamide Rituximab Methotrexate Etoposide Carboplatin Dacarbazine Paclitaxel Trastuzumab Others | Job senioritya ≤10 years: 31, 11–20 years: 13 and ≥ 20 years: 4 | Not informed |
| El‐Ebiary et al. |
| Egypt |
Cyclophosphamide Cisplatin Adriamycin Mitomycin C 5‐fluorouracil Methotrexate |
Years of exposure (mean SD) = Pharmacists: 5.8 ± 3.34 Nurse: 10.3 ± 4.52 | On average, 550 doses of different drug mixtures are prepared and administered every week |
| Bouraoui et al. |
| Tunísia |
Bleomycin Melphalan Cisplatin Busulfan Cyclophosphamide |
The mean handling time was 6 h/day 55% of our exposed have duration of exposure less than 5 years and only 25% superior to 10 years. | Not informed |
| Kopjar et al. |
| Croatia | Not informed |
Exposed subjects handled a diversity of antineoplastic drugs. Mean exposure time for the exposed group was 12.9 years | Not informed |
| Rombaldi et al. |
| Brazil | Not informed | 5 days of work | Not informed |
| Cornetta et al. |
| Italy |
Azathioprine Busulfan Cyclophosphamide Citarabine Doxorubicin Etoposide Fluorouracil Hydroxyurea Methotrexate Thiotepa Tretinoin Vincristine | 30 nonconsecutive working days | |
| Rekhadevi et al. |
| India | Most frequently antineoplastic drugs: cisplatin, carboplatin, adriamycin, bleomycin, endoxane |
Years of employment: 6–23 years Mean: ± 13,61 years | Not informed |
| Cavallo et al. |
| Italy |
Day‐care hospital nurse: Aneugens (vincristine and paclitaxel) 30–40 Alkylating agents (cyclophosphamide) 70–80 Others (5‐fluorouracil, methotrexate, epirubicin, gemcitabinea, cisplatin) Ward nurse: Aneugens (vinorelbineb, vincristine, paclitaxel, docetaxelb) Alkylating agents (cyclophosphamide, ifosfamideb) Others (etoposideb, epirubicin, cisplatin, bleomycinb, doxorubicinb, 5‐fluorouracil, cytarabinb, methotrexate, carboplatinb, ET–743b, epiadriamycinb) |
Day‐care hospital nurse: Aneugens: 30–40 times at week; alkylating agents: 70–80 times at week; others: 10–60 times at week. Ward nurse: Aneugens: 3–10 times at week; alkylating agents: 1–10 times at week; others: 2–10 times at week. | Not informed |
| Hongping et al. |
| China | Antineoplastic drug vincristine | Exposure years: 1–20 years | Not informed |
| Hongping et al. |
| China | Cyclophosphamide, vincristine, vinblastine, cis‐platinum, 5‐fluorouracil, bleomycin, MTX, and adriamycin. | Exposure years: 1–14 years | Not informed |
| Cavallo et al. |
| Italy |
Cyclophosphamide 5‐Fluorouracil Ifosfamide Cytarabine Gemcitabine |
Day‐care hospital nurse: 300 administration/week Ward nurse: 35 administration/week Pharmacy technicals: responsible for the preparation. | Not informed |
| Yang et al. |
| China | Not informed |
Nurses: average exposure duration: 5.5 years; Exposure to average 8.25 chemotherapeutic preparations daily | Not informed |
| Hessel et al. |
| Germany |
Cyclophosphamide Ifosfamide Doxorubicin Epirubicin Daunorubicin Idarubicin Cisplatin Carboplatin | Exposure to antineoplastic agents ranged from 1 to 144 months (mean 53 months). | Not informed |
| Maluf and Erdtmann |
| Brazil | Antineoplastic drugs include alkilants (e.g., cyclophosphamide), antimetabolics (e.g., fluoruracyl), spindle poisons (e.g., vincristeine), antibiotics (e.g., doxorubicin), and hormonal therapies (e.g., diethylstilbestrol). | A follow‐up study carried out 4 years. | Not informed |
| Pilger et al. |
| Austria |
Bleomycin Carboplatin Cisplatin Cyclophosphamide Dacarbazine Doxorubicin Epirubicin Etoposide Fluorouracil Gemcitabine Ifosfamide Methotrexate Vincristine Vinorelbine Others cytostatic drugs in minor frequency | 2 years of monitoring | Not informed |
| Kašuba et al. |
| Croatia | (5‐Fluorouracil, cyclophos‐phamide, cisplatinum, methotrexate, vincristine, vinblastine). |
Exposure period 1–14 years (8 nurses) Exposure period 20–31 years (12 nurses) | Not informed |
| Fucic et al. |
| Croatia |
Endoxan Vincristin Adriablastin 5‐Fu Alexan Bleomycin | Exposure period: 6 years, on average |
Over a week: Endoxan 4000 mg Vincristin 6 mg Adriablastin 150 mg 5‐Fu 1000 mg Alexan 200 mg Bleomycin 15 mg |
| Kevekordes et al. |
| Germany | Cisplatin, cyclophosphamide, iphosphamide, vincristin, doxorubicin, dactinomycin, cytosine arabinoside, and methotrexate | Exposure period: 2 months after a new safety hood was installed and 7 months later | Not informed |
| Machado‐Santelli et al. |
| Brazil | Vincristine, vinblastine, aracytosine C, 5‐fluorouracyl, cyclofosfamide, cisplatin, methotrexate, bleomycin, mitomycin, and adriablastin | We considered as exposed only individuals who regularly make up dilutions of the drugs | Not informed |
| Anwar et al. |
| Egypt | Cyclophosphamide, phenylalanine mustard, thiotepa, busulfan, methotrexate, 5‐fluorouracil, 6‐mercaptopurine, vinblastine, adriamycin, bleomycin, mitomycin C, and cisplatinum | Duration of exposure (months): 79.9 ± 46.2 | Not informed |
| Authors | Cell type |
| Gender | Age | No. evaluated units in the MN assay | Stain | Evaluated parameters for the MN assay | Inclusion criteria | Cito‐toxicity analysis | Blind analysis | Proper statistical description | Control group |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ness et al. |
Buccal epithelial cells Lymphocytes from peripheral blood |
Control: Nurse: 5 Pharmacist/Pharmacytechnician: 10 Other professions: 20 Exposed: Nurse: 20 Pharmacist/Pharmacytechnician: 9 Other professions: 0 |
Male (12) Female (52) |
Not exposed: 42.00 years Exposed: 41.00 years | 1000 cells | GelRed | Cell counting | Yes | No | No | Yes (Shapiro–Wilk, Student's | Yes |
| Pajic et al. | Lymphocytes from peripheral blood |
Control: 201 Exposed: 222 |
Control: Male (99) and female (102) Exposed: Male (106) and female (116) |
Control: 42.31 ± 8.02 Exposed: 40 ± 13 | 1000 binucleated cells | Giemsa | Cell counting | Yes | Yes (apoptotic cells count, necrotic cells count and nuclear division index) | Yes | Yes (Kolmogorov–Smirnov test, Student | Yes |
| Aristizabal‐Pachon and Castillo | Lymphocytes from peripheral blood |
Control: 40 Exposed drug administration: 12 Pharmacy: 26 Other: 2 |
Control female (32) and male (8) Exposed female (32) and male (8) |
Control: 30.80 ± 5.5 years Exposed: 32.05 ± 5.1 years | 1000 binucleated cells | Giemsa | Cell counting | Yes | Yes (lymphocytes were isolated was assayed for viability) | No | Yes (chi‐square, Fisher's, Pearson's χ2, Student | Yes |
| Santos et al. |
Buccal epithelial cells Urine |
Control: 10 Exposed: 49 |
Control female (5) and male (5) Exposed female (35) and male (14) |
Control minimum: 21 and maximum: 50 years Exposed minimum: 24 and maximum: 57 years | 1000 cells |
Giemsa Ethidium bromide | Cell counting | Yes | No | No | Yes (Tukey–Kramer, Kruskal–Wallis, Dunn according) | Yes |
| Ursini et al. |
Buccal epithelial cells Urine |
Control: 53 Exposed administrator: 25 and preparator: 17 |
Control female (13) and male (15) Exposed administrator female (20) and male (5) Preparators female (8) and male (9) |
Control: 40.9 ± 11.0 years Exposed administrator: 40.0 ± 9.2 years and Preparators: 42.8 ± 9.3 years | 2000 cells |
Acridine Orange Gel red | Cell counting (MN, NB, CC, BE) | Yes | Yes (advanced stage of necrosis and apoptosis) | No | Yes (ANOVA, Mann–Whitney | Yes |
| Mahmoodi et al. | Lymphocytes from peripheral blood |
Control: 74 Exposed tochemo‐therapeutics: 81 | Female and male |
Control female 35.35 ± 7.95 and male 33.87 ± 6.58 years Exposed tochemo‐therapeutics: female 35.35 ± 7.95 and male 35.61 ± 7.5 years | 500 binucleated cells | Giemsa | Cell counting | Yes | No | Yes | Yes (Student's | Yes |
| Ladeira et al. | Lymphocytes from peripheral blood |
Control: 111 Exposed nurses: 27 |
Control female (54) and male (57) Exposed nurses female (5) and male (22) |
Control: 34.25 ± 0.88 years Exposed: 34.89 ± 1.47 years | — | Cell counting (MN, lymphocytes) | Yes | No | Yes | Yes (Shapiro–Wilk test, Mann–Whitney test) | Yes | |
| Mrđanović et al. | Lymphocytes from peripheral blood |
Control: 20 Exposed: 15 | Only female |
Control: 35.5 years Exposed: 38 years | 1000 binucleated cells | Giemsa | Cell counting (MN and BN) | Yes | No | No | Yes (Mann–Whitey | Yes |
| Villarini et al. | Lymphocytes from peripheral blood |
Control: 50 Exposed: 48 |
Control female (38) and male (12) Exposed nurses female (41) and male (7) |
Control: 36.56 ± 11.17 years Exposed: 39.81 ± 9.56 years | 1000 binucleated cells | Giemsa | Cell counting (MN and BN) | Yes | No | Yes | Yes (Mann–Whitney | Yes |
| El‐Ebiary et al. | Lymphocytes from peripheral blood |
Control: 30 Exposed: Pharmacists: 18 Nurses: 20 | Only female |
Control: 30.86 ± 5.77 years Pharmacists: 31.38 ± 4.39 years Nurses: 31.1 ± 4.96 years | 1000 binucleated cells | Giemsa | Cell counting | Yes | No | Yes | Yes (Student's | Yes |
| Bouraoui et al. | Lymphocytes from peripheral blood |
Control: 20 Exposed: 20 nurses | Females (16) and male (4) |
Control: 33.8 ± 8.37 years Exposed: 35.85 ± 8.05 years | 2000 binucleated cells | Giemsa | Cell counting | Yes | No | No | Yes (Student's | Yes |
| Kopjar et al. | Lymphocytes from peripheral blood |
Control: 50 Exposed nurses: 50 | Only female |
Control: 37.98 ± 78.96 years Exposed: 37.00 ± 78.87 | 1000 binucleated cells | Giemsa | Cell counting | Yes | No | Yes | Yes ((Mann–Whitney | Yes |
| Rombaldi et al. | Lymphocytes from peripheral blood |
Control: 20 Exposed: 20 |
Control: Male (2) and female (18) Exposed: Male (2) and female (18) |
Control: 23–56 years Exposed: 21–54 years | 1000 cells | Giemsa | Cell counting | Yes | No | Yes | Yes ( | Yes |
| Cornetta et al. | Lymphocytes from peripheral blood |
Control: 73 Exposed: 83 |
Control: Male (20) and female (53) Exposed: Male (16) and female (64) |
Control: 23–56 years Exposed: 26–58 years | 1000 cells | Giemsa | Cell counting | Yes | No | Yes | Yes (Mann–Whitney | Yes |
| Rekhadevi et al. |
Lymphocytes from peripheral blood Buccal epithelial cells |
Control: 60 Exposed: 60 | Only female |
Control: 37.95 ± 5.64 years Exposed: 38.21 ± 5.61 years |
500 binucleated cells (lymphocytes) 1000 cells (buccal epithelial cells) |
Giemsa (MN lymphocytes) DAPI (MN buccal epithelial cells) | Cell counting | Yes | No | Yes | Yes (Student's | Yes |
| Cavallo et al. |
Lymphocytes from peripheral blood Buccal epithelial cells |
Control: 20 Exposed: Day‐care hospital nurse: 10 Ward nurse: 13 |
Control: Male (3) and females (17) Exposed: Day‐care hospital nurse: Male (2) and females (8) Ward nurse: Male (2) and females (11) |
Control: 35.5 ± 8.6 years Day‐care hospital nurse mean age: 37.6 ± 6.1 years Ward nurses: mean age, 32.7 ± 7.7 years |
1000 binucleated cells (MN Lymphocytes) 2000 cells (MN buccal epithelial cells) 110 binucleated cells (FISH MN) |
Giemsa (lymphocytes) Acridine Orange (buccal epithelial cells) DAPI (FISH) | Cell counting (MN and FISH) | Yes | No | Yes | Yes (one‐way ANOVA, chi‐square test, Student | Yes |
| Hongping et al. | Lymphocytes from peripheral blood |
Control: 15 Exposed: 15 | Female (9) and male (6) |
44.17 ± 2.40 years (male) 43.33 ± 1.14 years (female) |
1000 binucleated cells | Giemsa | Cell counting | Yes | Yes (proliferation index) | No | Yes (Wilcoxon's rank sum test and Kendall's test) | Yes |
| Hongping et al. | Lymphocytes from peripheral blood |
Control: 21 Exposed: 21 |
Control female (10) and male (11) Exposed female (10) and male (11) |
Control: 21–55 years Exposed: 19–50 years | 1000 binucleated cells (MN) | Giemsa | Cell counting | Yes | Yes (lymphocytes were isolated was assayed for viability) | No | Yes (Student | Yes |
| Cavallo et al. |
Lymphocytes from peripheral blood Buccal epithelial cells |
Control: 20 Exposed: Day‐care hospital nurse: 10 Ward nurse: 13 Pharmacy technician: 5 |
Control: Male (5) and females (25) Exposed: Day‐care hospital nurse: Male (2) and females (10) Ward nurse: Male (2) and females (11) Pharmacy technicians: Male (3) and female (2) |
Control: 34.9 ± 8.5 Exposed: Day‐care hospital nurse: 37.6 ± 5.5 Ward nurse: 32.7 ± 7.7 Pharmacy technicians: 35.8 ± 9.9 |
1000 binucleated cells (MN lymphocytes) 2000 cells (MN buccal epithelial cells) |
Giemsa (MN Lymphocytes) Acridine Orange (MN buccal epithelial cells) | Cell counting | Yes | No | No | Yes (one‐way ANOVA, | Yes |
| Yang et al. | Lymphocytes from peripheral blood |
Control: 16 Exposed: 16 | Only female |
Control: Not informed Exposed: Nurses average age of 29 years; | 1000 binucleated cells | Giemsa | Cell counting | Yes | No | No | Yes (Rank sum test) | Yes |
| Hessel et al. | Lymphocytes from peripheral blood |
Control: 60 Exposed: 93 |
Control: Male (19) and female (41) Exposed: Male (12) and female (81) |
37.2 ± 10.4 (control) 36.5 ± 8.9 (exposed) | 1000 cells | Giemsa | Cell counting | Yes | No | Yes | Yes (Spearman's rank correlation) | Yes |
| Maluf and Erdtmann | Lymphocytes from peripheral blood |
Control: Control: 4 years before (10) Control 4 years after (12) Exposed: Nurses 4 years before (10) Nurses 4 years after (12) | Not informed, but the sex was matched. |
Control: Control: 4 years before (31.5 ± 5.38) Control 4 years after (34.75 ± 5.42) Exposed: Nurses 4 years before (29.8 ± 7.79) Nurses 4 years after (34.42 ± 4.48) | 2000 binucleated cells | Giemsa | Cell counting | Yes | No | No | Yes (Mann–Whitney | Yes |
| Pilger et al. | Lymphocytes from peripheral blood |
Control: 39 Exposed: 39 | Male and female | 24–54 years | 2000 cells | DAPI | Cell courting | Yes | No | Yes | Yes (ANOVA) | Yes |
| Kašuba et al. | Lymphocytes from peripheral blood |
Control: Control for micronucleus assay: 16 Control for SCE assay: 20 Exposed: 20 | Not informed |
Control: Control for micronucleus assay: 21–50 years old Exposed: Nurses (21–50 years old) | 1000 binucleated cells | Giemsa | Cell counting | Yes | No | No | Yes (chi‐square test) | Yes |
| Fucic et al. | Lymphocytes from peripheral blood |
Control: 40 Exposed: 38 |
Control: Only female Exposed: Not informed |
Control: Not informed Exposed: 21–45 years old | 500 cells | Not informed | Cell counting | Yes | Yes (mitotic activity) | Yes | Yes (test of proportions, Kolmogorov–Smirnov test) | Yes |
| Kevekordes et al. | Lymphocytes from peripheral blood |
Control: 10 Exposed: 10 | Only female |
Control: Not described Exposed: 23 ± 38 years | 1000 binucleated cells (CBMN) | Giemsa | Cell counting (MN) | Yes | No | No | Yes (Wilcoxon, and Mann–Whitney | Yes |
| Machado‐Santelli et al. | Buccal ephithelial cells |
Control: 25 Exposed: 25 | Female and male |
Control: 34.60 ± 1.54 years Exposed: 32.08 ± 1.29 years | 1000 cells | Feulgen fast green | Cell counting | Yes | No | Yes | Yes (chi‐square test and Student's | Yes |
| Anwar et al. | Lymphocytes from peripheral blood |
Control: 20 Exposed: 20 | Female |
Control: 28.5 ± 5.25 years Exposed: 29.6 ± 5.4 years | 1000 binucleated cells | Giemsa | Cell counting | Yes | No | Yes | Yes (chi‐square test) | Yes |
| Authors | Genotoxicity | Observations |
|---|---|---|
| Ness et al. | No significant difference |
The study population was composed of 81.3% of women. The exposed group used PPE. |
| Pajic et al. |
⬆ MN ⬆NBUD Lymphocytes |
Higher MN frequencies were associated with female sex and older age, but smoking did not influence DNA damage. Cytostasis and cytotoxicity parameters showed no variation related to exposure, sex, age, or smoking. Strong correlation between MN and NBUD. Exposure length dependent. |
| Aristizabal‐Pachon and Castillo |
⬆ MN Lymphocytes | No significant differences were found related to age and gender in the two groups. However related to gender, we found a significant increase of DNA damage in females when compared to males in exposed individuals. |
| Santos et al. |
⬆ MN Lymphocytes | — |
| Ursini et al. |
⬆ MN Lymphocytes | — |
| Mahmoodi et al. |
⬆ MN Lymphocytes | — |
| Ladeira et al. |
⬆ MN Lymphocytes | Hospital A showed a higher percentage of contaminated samples (50%) than Hospital B (8.57%), but no difference was found between contamination levels. (5‐fluorouracil). |
| Mrđanović et al. |
⬆ MN Lymphocytes AO supplementation: micronucleus frequency and was significantly reduced | The group exposed subjects was taking antioxidative supplementation by oral administration of one capsule per day of Oligogal Se. |
| Villarini et al. | No significant differences | Mo correlations were found between job seniority, age, smoking habits and MN rates. |
| El‐Ebiary et al. | No significant differences | Statistical analysis detected a significant difference in years of exposure between nurses and pharmacists. |
| Bouraoui et al. |
⬆ MN Lymphocytes | — |
| Kopjar et al. |
⬆ MN Lymphocytes | We also noticed that age significantly contributed to the increase of comet tail length among nonsmokers. |
| Rombaldi et al. |
⬆ MN Lymphocytes | Within the experimental group, no difference was observed between participants with different exposure times prior to the experiment, but rather between participants of younger and older ages. |
| Cornetta et al. |
⬆MN Lymphocytes | When gender is taken into account, females show a significant higher MN value when compared to males in control and exposed group. |
| Rekhadevi et al. |
⬆ MN Oral cells and lymphocytes | |
| Cavallo et al. |
⬆ MN Exfoliated buccal cells |
Significant association between vinorelbine exposure and presence of centromeric signal (FISH MN+). The higher percentage of small MN associated with exposure to alkylating agents confirms the clastogenic activity of these drugs. Administration of antineoplastic drugs in wards was associated with increased FISH MN + frequency. |
| Hongping et al. |
⬆ MN Lymphocytes | |
| Hongping et al. |
⬆ MN Lymphocytes | Correlation between exposure years and micronucleus formation |
| Cavallo et al. |
⬆ MN Buccal cell |
Detection of α‐fluoro‐β‐alanine exclusively in exposed nurses highlights occupational absorption. Increased MN frequency in buccal cells but not in lymphocytes may reflect local exposure (oral cavity). High contamination in administration areas reinforces occupational risk. |
| Yang et al. |
⬆ MN Lymphocytes | — |
| Hessel et al. | No significant changes | The only monitoring consists of serum levels of platinum (a main component of cytostatic drugs) and anthracyclines, but it is important to note that serum levels of platinum and anthracyclines were not elevated in this case. |
| Maluf and Erdtmann |
⬆ MN Lymphocytes | No associations were found with age, sex, or smoking habits. |
| Pilger et al. | No significant differences | Positive results were observed only for accidental exposure to the drugs among pharmacy personnel. However, the exposure doses are not measured. |
| Kašuba et al. |
⬆ MN Lymphocytes | A significant increase in micronucleated lymphocytes was observed in nurses exposed to cytostatic drugs with longer exposure periods, but not significant when compared to shorter exposure period. |
| Fucic et al. |
⬆ MN Lymphocytes | 20 subjects had an insufficient number of cells for mitotic activity analysis. |
| Kevekordes et al. |
⬆ MN Lymphocytes | |
| Machado‐Santelli et al. |
⬆ MN Lymphocytes | Smokers and nonsmokers do not differ significantly with respect to the incidence of micronuclei. |
| Anwar et al. |
⬆ MN Lymphocytes |
| Author | No. confounders | Detail | Rating |
|---|---|---|---|
| Ness et al. | 1 | Blind analysis | Moderate |
| Pajic et al. | 0 | — | Strong |
| Aristizabal‐Pachon and Castillo | 1 | Blind analysis | Moderate |
| Santos et al. | 1 | Blind analysis | Moderate |
| Ursini et al. | 1 | Blind analysis | Moderate |
| Mahmoodi et al. | 1 | Amount of evaluated cells | Moderate |
| Ladeira et al. | 0 | — | Strong |
| Mrđanović et al. | 0 | — | Strong |
| Villarini et al. | 0 | — | Strong |
| El‐Ebiary et al. | 0 | — | Strong |
| Bouraoui et al. | 1 | Blind analysis | Moderate |
| Kopjar et al. | 0 | — | Strong |
| Rombaldi et al. | 0 | — | Strong |
| Cornetta et al. | 0 | — | Strong |
| Rekhadevi et al. | 1 | Amount of evaluated cells | Moderate |
| Cavallo et al. | 0 | — | Strong |
| Hongping et al. | 1 | Blind analysis | Moderate |
| Hongping et al. | 1 | Blind analysis | Moderate |
| Cavallo et al. | 1 | Blind analysis | Moderate |
| Yang et al. | 1 | Blind analysis | Moderate |
| Hessel et al. | 0 | — | Strong |
| Maluf and Erdtmann | 1 | Blind analysis | Moderate |
| Pilger et al. | 0 | — | Strong |
| Kašuba et al. | 1 | Blind analysis | Moderate |
| Fucic et al. | 1 | Amount of evaluated cells | Moderate |
| Kevekordes et al. | 1 | Blind analysis | Moderate |
| Machado‐Santelli et al. | 2 | Blind analysis and amount of evaluated cells | Weak |
| Anwar et al. | 0 | — | Strong |
- —Conselho Nacional de Desenvolvimento Científico e Tecnológico10.13039/501100003593
- —Coordenação de Aperfeiçoamento de Pessoal de Nível Superior10.13039/501100002322
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSafe Handling of Antineoplastic Drugs · Carcinogens and Genotoxicity Assessment · Effects and risks of endocrine disrupting chemicals
Introduction
1
The widespread use of antineoplastic drugs in cancer treatment has led to significant concerns regarding the potential health risks posed to healthcare professionals involved in the preparation, administration, and/or handling of these agents (Roussel et al. 2019). These drugs are designed to target rapidly dividing cancer cells, but due to their nonselectivity, they can also damage normal, healthy cells, leading to harmful genotoxic and carcinogenic effects (Villarini et al. 2010; Villarini et al. 2016).
Chemotherapy agents encompass a broad range of drugs, including alkylating agents, antimetabolites, topoisomerase inhibitors, and plant alkaloids (Connor et al. 2005). These drugs vary in their mechanisms of action and genotoxic potential, which makes the evaluation of exposure risk a complex scenario. To overcome the question, occupational exposure to these drugs has been evaluated under different contexts and paradigms, demonstrating increased rates of genetic damage in healthcare professionals, as measured by different biomarkers, the micronucleus assay being the most commonly used (Ness et al. 2021; Pajic et al. 2021). This biomarker is broadly used in genotoxicity studies to assess the chromosome breakage induced by chemical substances found in the environment (Connor et al. 2005).
Micronuclei are small extranuclear bodies that form during cell division when chromosome fragments or whole chromosomes fail to incorporate into daughter nuclei, often as a result of exposure to genotoxic agents (Bonassi et al. 2011). This makes the micronucleus assay a valuable tool in biomonitoring studies, especially among individuals exposed to potentially genotoxic substances in occupational or environmental settings (Bonassi et al. 2011).
Numerous studies have shown an elevated frequency of genetic damage in healthcare professionals exposed to chemotherapy agents. Particularly, healthcare workers in hospitals have been reported to have a higher incidence of micronuclei when compared to unexposed populations (Gianfredi et al. 2017; Villarini et al. 2016). This was strongly evident in workers involved in drug preparation, such as nurses and pharmacists, where exposure levels can be significantly higher (Connor et al. 2005), potentially through inhalation of aerosols or direct dermal contact with these agents (Roussel et al. 2019). However, the data on this subject are not entirely consistent, with some studies showing no significant genetic damage in exposed workers. This inconsistency may arise from factors such as differences in study design, methodological variations, and the use of protective measures in the workplace (Gianfredi et al. 2017).
Given these challenges described above, the aim of this systematic review was to critically assess the evidence regarding the genotoxic effects through micronuclei incidence of chemotherapy drugs on healthcare workers. Furthermore, this review also seeks to evaluate the quality and reliability of the studies published on this topic. By consolidating the available evidence, this review aims to provide a clearer understanding of the occupational risks associated with chemotherapy drug exposure (Roussel et al. 2019). We understand the findings of this review will contribute to the broader understanding of the cancer risk faced by healthcare workers in oncology settings and may inspire future studies on new guidelines for improving safety protocols in these environments.
Material and Methods
2
This systematic review was conducted in accordance with the PRISMA 2020 guidelines and structured around the PICO model: P (Mammalian cells), I (Chemotherapeutic drugs), C (Control group), O (Genotoxicity through micronuclei formation).
Studies were deemed eligible if they fulfilled the following criteria: (1) experimental studies assessing genetic damage and/or cell death triggered by chemotherapeutic agents; (2) publications written in English; (3) data reported in compliance with internationally recognized scientific standards and suitable for extraction.
Studies were excluded based on the following criteria: (1) conference proceedings, literature reviews, editorials, or correspondence pieces; (2) full text not available in English; (3) studies with missing or nonextractable data; (4) research involving nonmammalian cell lines; (5) absence of genotoxicity assessment through the micronucleus assay; (6) unclear or incomplete outcome reporting.
Search Strategy
2.1
A comprehensive literature search was carried out in May 2025 using the electronic databases PubMed, SCOPUS, and Web of Science. The search strategy combined relevant descriptors using Boolean operators: (“Chemotherapeutic drug” OR “Antineoplastic agent”) AND (“Genotoxicity” OR “Mutagenicity”) AND (“Micronucleus assay”) AND (“Mammalian cells”).
To ensure thorough coverage, we also performed manual screening of reference lists from selected articles. The search was not restricted by publication date. Five independent reviewers (TGP, LSA, GCA, DVS, and DAR) conducted the initial screening of titles and abstracts. Full‐text articles were retrieved and assessed for eligibility. Any disagreements were resolved through discussion until consensus was reached. The complete search strategy is detailed in Table 1.
Data Extraction and Quality Assessment
2.2
After independently extracting data from eligible studies by examining titles, abstracts, and full texts, the reviewers (TGP, LSA, GCA, DVS, and DAR) organized the relevant data following the methodology described by Guedes Pinto et al. (2024), which includes the following details: authors, publication year and country, cell types, exposure duration, assay conducted, number of cells evaluated, geno‐ and cytotoxicity assays utilized, blind analysis status, statistical methods, negative control, and key findings.
In parallel with data extraction, a risk of bias assessment was conducted using a tailored evaluation checklist adapted from previous systematic toxicology reviews by Guedes Pinto et al. (2024). The quality of the included studies was independently assessed by four reviewers (TGP, LSA, GCA, DVS, and DAR), with different relevant variables (confounders) considered in the evaluation (such as staining methods, minimum amount of evaluated cells, inclusion of blind analysis, and control groups, proper statistical analysis). In terms of the methodology for classifying the studies, those in which all variables were controlled were classified as strong. Conversely, studies where up to one confounder was not controlled were rated as moderate, and those with two or more uncontrolled confounders were considered weak at final rating, as described by Guedes Pinto et al. (2024).
Results
3
Study Selection
3.1
The initial online search yielded 329 scientific records; however, 299 of these were duplicates and thus excluded. Following an assessment of the titles and abstracts, 2 studies were deemed irrelevant for the purposes of this research and were removed. This exclusion applied to reviews. Full manuscripts from 28 studies were carefully read by the authors of this article. The flow chart of the study is shown in Figure 1.
Flow chart of the study evaluating the occupational exposure to antineoplastic drugs by micronucleus assay.
General Characteristics of the Included Studies
3.2
The most important characteristics of the studies included in the systematic review are summarized in Table 2. A total of 28 studies were evaluated, including six studies conducted in Italy, four in Brazil, three in Serbia, two in China, and the remaining studies distributed across countries such as Colombia, Egypt, Germany, India, Iran, Portugal, Spain, Tunisia, Croatia, Austria, Thailand, United Kingdom, France, Greece, and others. The types of drugs investigated were mainly antineoplastic agents, including commonly studied compounds such as cyclophosphamide, 5‐fluorouracil, bleomycin, cisplatin, doxorubicin, vincristine, methotrexate, and many others. Exposure periods ranged widely from several months to more than 20 years, with daily occupational exposure times varying between less than 1 h up to 7–8 h or more, depending on the study population and work setting. Most studies did not report exact exposure dosages. These data are detailed in Table 2.
Table 3 provides a comprehensive summary of the primary methodological and demographic characteristics of the 28 studies included in this systematic review, having all of them conducted the micronucleus assay. The selected studies evaluated genotoxic effects of chemotherapeutic agents on mammalian cells in vivo, primarily focusing on lymphocytes from peripheral blood and buccal epithelial cells. The number of participants, gender distribution, and age ranges are reported for both control and exposed groups.
The number of evaluated units (e.g., binucleated cells or metaphases), staining techniques (such as Giemsa, Ethidium Bromide, DAPI, or Acridine Orange), and types of endpoints assessed (e.g., micronucleus frequency) are specified for each study. Among the studies that performed the micronucleus assay in peripheral blood, only 2 evaluated less than 1000 cells, which was considered a confounder as per the methodological standard for ensuring reliable quantification of nuclear abnormalities. As for the ones that conducted the assay in oral cells, two was also the number of studies that failed to analyze the minimum number of required cells (2000 in oral cells).
The inclusion of cytotoxicity analysis and whether studies performed blind evaluation or presented a proper statistical description were also considered, along with the use of control groups. Most studies included a negative control and applied robust statistical analyses (e.g., Student's t test, Mann–Whitney U test, ANOVA, Kruskal–Wallis), although blind assessments were less frequently reported. This heterogeneity in methodological quality and design highlights the need for cautious interpretation of genotoxicity outcomes across studies.
Main Results
3.3
Of the 28 studies reviewed, 23 reported genotoxic effects associated with occupational exposure to antineoplastic drugs, as detected by the micronucleus assay. All studies assessed peripheral blood lymphocytes, while only three also evaluated oral mucosal cells. In these three studies, an increased frequency of micronuclei was consistently observed in oral cells, even in cases where no significant changes were detected in lymphocytes. In contrast, five studies found no statistically significant genotoxic differences between exposed and control groups in either cell type.
Cytotoxicity was less frequently assessed, with only five studies providing relevant data. Among them, some reported altered cell viability, enzymatic activity (e.g., catalase and glutathione peroxidase), or mitotic delay. However, these findings were less consistent than genotoxic outcomes, highlighting a gap in cytotoxicity assessment.
Among the few studies that analyzed genetic polymorphisms, such as XRCC1, XRCC3, and hOGG1, no statistically significant associations were found with DNA damage, although some studies reported higher genotoxic effects in females. Importantly, Pilger et al. (2000) distinguished accidental from routine exposure, showing that accidental handling of chemotherapeutic agents can result in elevated genotoxic markers, even when routine exposure levels appear safe.
Overall, these findings reinforce the genotoxic potential of occupational exposure to antineoplastic drugs, particularly through increased micronucleus frequency. The limited assessment of cytotoxicity and polymorphisms points to the need for broader, integrative biomonitoring protocols in healthcare professionals exposed to such compounds (see Table 4).
Quality Assessment
3.4
The methodological quality of the 28 studies included in this review indicates a generally solid foundation for the evidence presented. Almost all studies were rated as either strong or moderate, reflecting acceptable to high methodological rigor. Specifically, 12 of the studies received a strong rating, while 15 were classified as moderate and 1 was classified as weak. These studies commonly employed blind analysis, reported cytotoxicity alongside genotoxicity, and considered relevant confounding factors such as sex, age, and smoking status. Such methodological features enhance the reliability of their findings.
In addition, it is important to highlight that the observed grading assessment supports the consistency of the observed associations between occupational exposure to antineoplastic drugs and genotoxic outcomes. This quality profile reinforces the strength of the evidence base for this systematic review (see Table 5).
Discussion
4
This systematic review aimed to evaluate the genotoxic effects through the micronucleus assay of occupational exposure to antineoplastic drugs among healthcare professionals. The findings of this review demonstrate a consistent pattern of genotoxic effects associated with exposure to antineoplastic agents. Among the 28 studies included, the vast majority reported increased frequencies of micronuclei in exposed individuals compared to control groups. Notably, micronucleus formation as an endpoint underscores its sensitivity as a biomarker for genotoxicity in occupational biomonitoring, as validated by Bonassi et al. (2011), who demonstrated that increased micronucleus frequency reliably predicts cancer risk and reflects chromosomal damage in exposed human populations.
Conversely, cytotoxicity was less frequently assessed, appearing in only a minority of studies. When evaluated, indicators such as cell viability, apoptosis, and necrosis yielded inconsistent findings. This may be due to methodological limitations or variability in the parameters chosen for cytotoxicity detection. Nonetheless, the presence of cytotoxicity in some cohorts reinforces the biological impact of chronic exposure to cytotoxic agents, especially among pharmacists and nurses handling high volumes of chemotherapy drugs without adequate protective measures.
Among the 28 studies reviewed, only three included the micronucleus assay in oral mucosal cells. Notably, all three reported a significant increase in micronuclei frequency in oral cells, even in cases where no genotoxic alterations were detected in peripheral blood lymphocytes. This finding highlights the potential sensitivity of the oral mucosa as a biomarker for occupational exposure to antineoplastic agents. Despite its diagnostic value and the fact that it is a noninvasive collection method, the use of oral cell assays remains underexplored in the current literature within the field (Thomas et al. 2009).
Furthermore, it is important to highlight that a minimum number of cells is required to ensure the reliability of micronucleus assay results. A total of 1000 cells per subject for peripheral blood lymphocytes and 2000 for oral mucosa cells, as recommended by OECD guidelines (OECD 2016). Among the studies reviewed, this criterion was met or exceeded in nearly all cases that assessed peripheral blood, reinforcing the methodological quality of the findings (only one study analyzing blood samples failed to reach the recommended cell count threshold).
As for oral cell evaluation, two out of the three studies that assessed this tissue failed to reach the recommended threshold of 2000 cells per individual (Bonassi et al. 2011). Despite the reduced number of cells analyzed, both studies still reported an increased frequency of micronuclei, reinforcing the high sensitivity of the oral mucosa as a biomarker site for genotoxic effects. This finding aligns with prior evidence suggesting that epithelial tissues, particularly those with high cell turnover like the oral mucosa, are effective indicators in biomonitoring protocols (Bonassi et al. 2011; Ceppi et al. 2009).
It is important to stress that the genotoxic effects observed were often more pronounced in female participants, as reported in several studies, suggesting that biological sex may modulate susceptibility to genotoxic effects. Although the underlying mechanisms remain unclear and warrant further investigation, sex‐related differences in DNA repair capacity and hormonal influences have been proposed (Hartmann and Speit 2014). Additionally, duration and intensity of exposure were critical factors, with professionals having longer exposure histories, often exceeding 5–10 years, consistently exhibiting higher rates of genotoxic damage, reinforcing the dose–response relationship seen in occupational genotoxicology (Bolognesi 2003).
This variability in genotoxicity induced by antineoplastic drugs may be primarily attributed to genetic polymorphisms that influence DNA repair mechanisms, oxidative stress responses, and apoptosis pathways. For this reason, understanding a genetic component in the variability of population responses to chemicals could be highly valuable for determining individual doses in chemotherapy and selecting individuals for occupations involving chronic exposure (Sivadas et al. 2025). Furthermore, lifestyle factors, such as smoking, can exacerbate the genotoxic effects by generating additional oxidative stress, further complicating the relationship between antineoplastic drugs and genetic damage (Katoh and Katoh 2009). In this study, only a few studies evaluated polymorphisms in DNA repair genes (e.g., XRCC1, XRCC3, hOGG1). While no consistent associations were observed, the inclusion of genetic variables represents an important direction for future research, particularly in identifying subgroups of workers at elevated risk.
The quality of the studies conducted is an important consideration when evaluating the risks of chemotherapy drug exposure. Small sample sizes, lack of control groups, and failure to account for confounding factors can affect the reliability of findings (Connor et al. 2005; Villarini et al. 2016). These factors must be carefully considered when interpreting the results of these studies. Despite the variation in study designs and geographical contexts, a notable strength of this review lies in the overall quality of the included studies. According to our quality assessment, all studies, except one (27 out of the 28), were classified as moderate or strong, reflecting solid methodological rigor. This enhances the credibility of the observed associations and reinforces the urgency of mitigating occupational exposure to these hazardous substances.
Nevertheless, some limitations must be acknowledged. A minority of studies failed to perform blind analyses or fully adjust for confounders such as age, sex, smoking status, and use of personal protective equipment. In addition, cytotoxicity was often overlooked, and dosage or drug concentrations were rarely quantified, impeding a detailed dose–response analysis. A further limitation is the lack of segregation between different chemotherapeutic agents, because each drug's distinct mechanism of action complicates isolating their specific genotoxic effects. Further studies could focus on this segregation.
From a public health perspective, these findings have significant implications. Antineoplastic drugs are inherently clastogenic and aneugenic, designed to target rapidly dividing cancer cells (De Flora 2000). However, their handling by healthcare workers without rigorous safety protocols results in unintended genotoxic consequences. The accumulation of chromosomal damage over time may elevate long‐term cancer risk, underscoring the need for systematic biomonitoring, mandatory use of PPE, proper ventilation systems, and ongoing training on safe handling practices in hospitals and pharmacies (Sessink and Bos 1999).
In conclusion, this systematic review provides robust evidence that occupational exposure to antineoplastic agents is associated with increased genotoxicity in healthcare professionals, particularly nurses and pharmacists, increasing the cancer risk. Therefore, the micronucleus assay is a suitable biomarker for biomonitoring these professionals. Given the high quality of the majority of included studies, these results offer a reliable basis for improving workplace safety regulations, expanding surveillance programs, and promoting institutional awareness regarding the hidden risks of handling antineoplastic drugs.
Author Contributions
Study design: Thiago Guedes Pinto, Lorrany da Silva Avanci, Daniel Vitor de Souza, Gabriel Carvalhal de Aguiar, and Daniel Araki Ribeiro. Data search: Thiago Guedes Pinto, Daniel Vitor de Souza, and Daniel Araki Ribeiro. Data analysis: Thiago Guedes Pinto, Lorrany da Silva Avanci, Daniel Vitor de Souza, Gabriel Carvalhal de Aguiar, Patricia Ramos Cury, Ana Claudia Muniz Renno, and Daniel Araki Ribeiro. Writing the paper: Thiago Guedes Pinto, Lorrany da Silva Avanci, Daniel Vitor de Souza, Gabriel Carvalhal de Aguiar, Patricia Ramos Cury, Ana Claudia Muniz Renno, and Daniel Araki Ribeiro.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Anwar, W. A. , S. I. Salama , M. M. El Serafy , S. A. Hemida , and A. S. Hafez . 1994. “Chromosomal Aberrations and Micronucleus Frequency in Nurses Occupationally Exposed to Cytotoxic Drugs.” Mutagenesis 9, no. 4: 315–317.7968572 10.1093/mutage/9.4.315 · doi ↗ · pubmed ↗
- 2Aristizabal‐Pachon, A. F. , and W. O. Castillo . 2020. “Genotoxic Evaluation of Occupational Exposure to Antineoplastic Drugs.” Toxicology Research 36, no. 1: 29–36.10.1007/s 43188-019-00003-7PMC 698862531998624 · doi ↗ · pubmed ↗
- 3Bolognesi, C. 2003. “Genotoxicity of Occupational Exposures: A Biomonitoring Approach.” Mutation Research 543, no. 3: 205–225. 10.1016/s 1383-5742(03)00065-6.12787816 · doi ↗ · pubmed ↗
- 4Bonassi, S. , A. Znaor , M. Ceppi , et al. 2011. “An Increased Micronucleus Frequency in Peripheral Blood Lymphocytes Predicts the Risk of Cancer in Humans.” Carcinogenesis 28, no. 3: 625–631.10.1093/carcin/bgl 17716973674 · doi ↗ · pubmed ↗
- 5Bouraoui, S. , A. Brahem , F. Tabka , N. Mrizek , A. Saad , and H. Elghezal . 2011. “Assessment of Chromosomal Aberrations, Micronuclei and Proliferation Rate Index in Peripheral Lymphocytes From Tunisian nurses Handling Cytotoxic Drugs.” Environmental Toxicology and Pharmacology 31, no. 1: 250–257.21787692 10.1016/j.etap.2010.11.004 · doi ↗ · pubmed ↗
- 6Cavallo, D. , C. L. Ursini , E. Omodeo‐Salè , and S. Iavicoli . 2007. “Micronucleus Induction and FISH Analysis in Buccal Cells and Lymphocytes of Nurses Administering Antineoplastic Drugs.” Mutation Research 628, no. 1: 11–18.17223378 10.1016/j.mrgentox.2006.10.014 · doi ↗ · pubmed ↗
- 7Cavallo, D. , C. L. Ursini , B. Perniconi , et al. 2005. “Evaluation of Genotoxic Effects Induced by Exposure to Antineoplastic Drugs in Lymphocytes and Exfoliated Buccal Cells of Oncology Nurses and Pharmacy Employees.” Mutation Research 587, no. 1–2: 45–51.16202645 10.1016/j.mrgentox.2005.07.008 · doi ↗ · pubmed ↗
- 8Ceppi, M. , B. Biasotti , M. Fenech , and S. Bonassi . 2009. “Human Population Studies With the Exfoliated Buccal Micronucleus Assay: Statistical and Epidemiological Issues.” Mutation Research 705, no. 1: 11–19. 10.1016/j.mrrev.2009.11.001.19932192 · doi ↗ · pubmed ↗