Quality of life and associated factors in institutionalized older adults: implications for gerontological nursing. Analytical study
Claudia Consuelo Torres Contreras, Albeiro Vargas Romero

TL;DR
This study explores factors affecting the quality of life in older adults living in nursing homes, emphasizing the importance of physical activity and cognitive health.
Contribution
The study identifies functional capacity and cognitive integrity as key determinants of well-being in institutionalized older adults.
Findings
Low scores in material well-being and interpersonal relations suggest resource and social support limitations.
Cognitive impairment and motor impairment significantly reduce the likelihood of high quality-of-life scores.
Physical and productive activities show a positive trend with better quality-of-life outcomes.
Abstract
Population aging and the rise in chronic diseases demand strengthening strategies to promote the well-being of institutionalized older adults. The FUMAT scale enables the assessment of quality of life across eight dimensions of well-being. To analyze the factors associated with the quality-of-life profile of institutionalized older adults. A cross-sectional analytical study was conducted with 250 permanent residents (≥3 months) of a nursing home in Bucaramanga, Colombia. Individuals aged 60 years or older with a reliable informant were included; those with terminal illness, acute psychiatric disorders, or clinical instability were excluded. The FUMAT scale, Barthel Index, PULSES profile, FRAIL scale, Downton Fall Risk Index, and the Short Portable Mental Status Questionnaire (SPMSQ) were applied. Descriptive and bivariate analyses were performed using Pearson's chi-square test,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
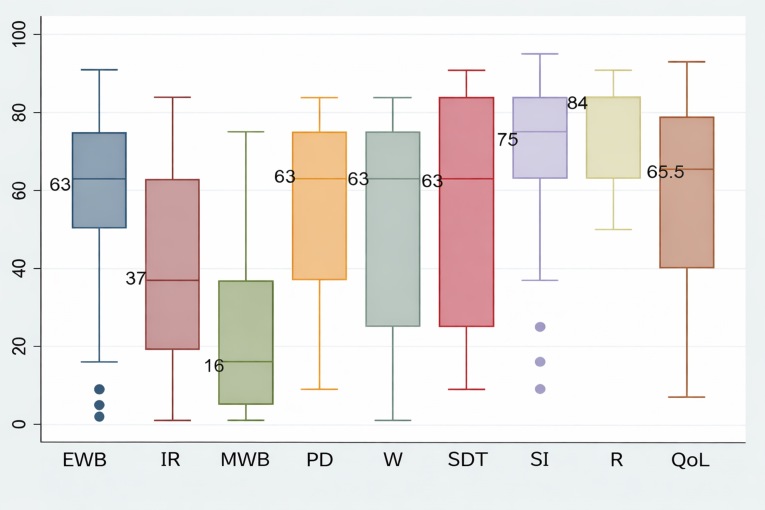 Figure 1
Figure 1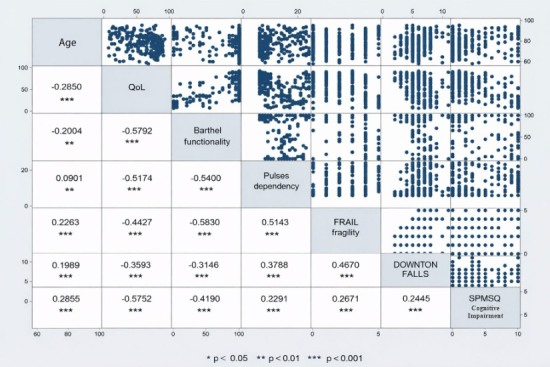 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAging, Health, and Disability · Nursing care and research · Aging and Gerontology Research
Introduction
Increased life expectancy and declining birth rates have led to an inversion of the population pyramid1. In Colombia, the National Administrative Department of Statistics (DANE) reported a 14.6% decline in births2, while projections from the World Health Organization (WHO) indicate sustained growth in population ageing both globally and across Latin American countries3. This phenomenon requires that care for older adults focus not only on prolonging life, but also on ensuring optimal living conditions. The increase in chronic diseases and the growing demand for specialized services have reinforced the role of nursing as a fundamental axis in promoting active and dignified aging4. From this perspective, the study and implementation of strategies aimed at improving quality of life become a priority, considering dimensions such as physical and emotional well-being, interpersonal relationships, self-determination, personal development, and social inclusion5,6.
Globally, the inversion of the population pyramid is progressing rapidly, particularly in developing countries, resulting in aging communities7. This process, together with age-related physiological changes, increases the risk of falls, functional decline, and increased mortality, thereby affecting quality of life, particularly among institutionalized individuals. Understanding these factors is essential for nursing to design interventions that promote autonomy, social participation, and functional and cognitive integrity8–10.
The quality of life in later life is a multidimensional concept influenced by socioeconomic factors, lifestyles, health, housing, and social support11. In Colombia, the population is undergoing rapid aging: the percentage of older adults rose from 6.9% in 1985 to 13.8% in 2020, with projections exceeding 16% by 2030. This phenomenon is further compounded by economic vulnerability, as only 23% receive a pension, 5% actively contribute to the pension system, and 70% make no contributions, which, in turn, increases the risk of institutionalization and abandonment12.
National studies demonstrate that social support and functional capacity are determinants of quality of life among older adults13, which should be understood in conjunction with environmental and cultural aspects, access to services, personal satisfaction, and recreational activities14. In this context, caregivers require evidence-based training to strengthen the physical and emotional well-being of older adults15, while care planning should incorporate strategies to promote physical and cognitive functioning and social participation16.
From an interdisciplinary approach, nursing holds a strategic position in the comprehensive assessment and early detection of risks among institutionalized individuals17. In addition to providing direct care, professionals should influence public policies aimed at reducing inequalities, ensuring access to services, and promoting social inclusion18.
The FUMAT scale has become the standard tool for assessing quality of life in nursing homes. Based on the model developed by Schalock and Verdugo, the scale assesses eight fundamental dimensions: emotional well-being, physical well-being, material well-being, self-determination, personal development, interpersonal relationships, social inclusion, and rights6. Its excellent psychometric properties have enabled its use in numerous studies, including one conducted in Cúcuta, Colombia, aimed at characterizing quality-of-life profiles19. The scale facilitates the planning of personalized care, comprehensive monitoring of physical, psychological, and social well-being, and identification of areas of vulnerability20–23. Nevertheless, the necessity persists to generate contextualized evidence that reflects the sociocultural realities of institutional settings. In response to this, the present study aimed to analyze the factors associated with the quality-of-life profiles among institutionalized older adults, contributing to the design of comprehensive, ethical, and humanized care strategies.
Materials and Methods
Design
A cross-sectional analytical study was conducted with institutionalized older adults in a nursing home in northern Bucaramanga during 2024. The population under study consisted of users of the Albeiro Vargas and Ángeles Custodios Foundation, which serves approximately 300 individuals from a low socioeconomic status. The sample size (n = 250) was determined using Epidat 3.1, taking as a reference the variability in physical well-being reported in a Spanish study (mean 44.52 ± 22.55)24, with an alpha error of 0.03 and a beta error of 0.80. Furthermore, the findings of Morales et al. in Ecuador25, which reported a 62.04% prevalence of excellent quality of life, were taken into consideration. This resulted in an alpha error of 0.024 and a beta of 0.80.
Convenience sampling was used. Individuals aged 60 years or older were included if they were permanent residents for at least three months and had a reliable informant. Individuals with terminal illness, acute psychiatric disorders, or clinical instability were excluded from the study.
Data was collected by the principal investigator, a nurse in postdoctoral training, following a three- month period of interaction and observation at the nursing home, which enabled an understanding of the participants’ social and functional dynamics. The FUMAT scale was administered with the support of gerontologists and caregivers, who acted as key informants to ensure the validity and reliability of the responses. The remaining instruments were administered directly by the researcher in accordance with standardized procedures. This methodological strategy ensured objectivity, consistency, and accuracy, faithfully reflecting the real conditions of institutionalized older adults.
Instruments
The FUMAT scale is an instrument designed to evaluate the quality of life of older adults, including those with severe physical disability or cognitive impairment, based on the model developed by Schalock and Verdugo4. It exhibits high content validity and internal consistency (α=0.95) and adequate reliability (r=0.90). Its application, intended for professionals familiar with the individual, does not require the direct participation of the person assessed and is based on observable behaviors. The scale consists of 57 items phrased in the third person, with four response options, and assesses eight dimensions: emotional well-being, interpersonal relationships, material well-being, personal development, physical well-being, self-determination, social inclusion, and rights6,26. The scale enables the creation of an individual profile using standardized scores that are comparable across dimensions, as well as an overall index and a percentile that reflect the level of quality of life, with higher values indicating better well-being.
Additionally, functional assessment instruments widely used in nursing practice were employed. The Barthel Index is a widely used instrument for assessing independence in basic activities of daily living among individuals with functional impairment, especially older adults. The instrument has demonstrated high reliability and validity across multiple studies, with internal consistency exceeding 0.85. The Barthel Index assesses ten basic activities and assigns scores ranging from 0 to 100, with lower scores denoting increased dependence: 0 to 20 (total dependence), 21 to 60 (severe dependence), 61 to 90 (moderate dependence), 91 to 99 (mild dependence), and 100 (independence). This scale enables the identification of the level of functional independence, guides care planning, and supports the assessment of the effectiveness of interventions aimed at maintaining or restoring autonomy27–29.
The PULSES profile assesses disability and functional status across different clinical settings, including rehabilitation and older adult care. It examines six dimensions: physical condition, upper and lower limb function, sensory stability, excretory function, and social and mental status. The instrument has demonstrated high interobserver reliability (r > 0.80) and good internal consistency (α = 0.75– 0.90). Each dimension is scored on a scale from 1 (independence) to 4 (severe dependence), with a total possible score of 6 to 24 points. Lower values indicate higher functional independence. Its comprehensive score facilitates categorization of disability, guides clinical decisions, prioritizes interventions, and monitors functional progression, making it a widely used instrument for planning autonomy-centered care30–32.
The FRAIL scale identifies frailty in older adults and enables the prediction of risks such as disability, hospitalization, and mortality. It assesses five dimensions: fatigue, resistance, aerobic capacity, illness, and loss of weight. Each item is scored 0 or 1, yielding a total score ranging from 0 to 5 that classifies individuals as robust (0), pre-frail (1–2), or frail (3–5). The scale has been validated across various geriatric populations and clinical settings, demonstrating high sensitivity, specificity, and interobserver reproducibility33–35.
The Downton Fall Risk Index assesses the risk of falls in older adults through five items: previous falls, medication use, sensory deficits, mental state, and gait. Each item is scored as 0 or 1, with a maximum total score of 5; values of 3 or higher indicate high risk. The instrument has demonstrated good sensitivity and specificity in detecting the risk of falls in the geriatric population; however, its clinical application has been characterized by high sensitivity and low specificity36–38.
The Pfeiffer’s SPMSQ is a brief instrument for detecting cognitive impairment in older adults. It assesses orientation, memory, calculation, and general knowledge through ten items administered rapidly. The instrument demonstrated good interobserver reliability (0.73) and intraobserver reliability (0.93), supporting its consistency. Each incorrect response is counted as an error, and the total number of errors is used to classify cognitive impairment as follows: 0–2 errors (normal), 3–4 (mild), 5–7 (moderate), and 8–10 (severe)39–41.
Data analysis
A descriptive analysis was performed according to the nature of the variables. Absolute and relative frequencies were calculated for qualitative variables, while medians and interquartile ranges were reported for quantitative variables. Distributional assumptions were assessed using the Shapiro– Francia test. Box-and-whisker plots were generated to illustrate the percentiles of the FUMAT Quality of Life Index (FUMAT-QOLI) dimensions.
The outcome variable, the FUMAT Quality of Life Index, was categorized into tertiles; the first and second tertiles were grouped and compared with the third tertile, resulting in the creation of a dichotomous nominal variable. Pearson’s chi-square test or Fisher’s exact test was used for qualitative variables, and the Mann–Whitney U test was applied for quantitative variables.
Correlation analysis was conducted using Spearman’s rho, and a correlation matrix was generated to examine the relationships between age and the scores of the FUMAT-QOLI, the Barthel Index, the PULSES profile, the FRAIL scale, the Downton Fall Risk Index, and the SPMSQ. To identify factors associated with the upper tertile of the QLI, multivariate logistic regression was performed following the steps proposed by Hosmer and Lemeshow42, including variables with p <0.05 in the bivariate analysis and age, given its clinical relevance. Model’s fit was assessed using the Hosmer–Lemeshow test. All analyses were conducted using Stata v17 and, in accordance with the open science guidelines, the data were deposited in Mendeley Data43.
Ethical considerations
The research was conducted in accordance with the principles of confidentiality and data protection, thereby ensuring that participants were the focus of ethical protection. Data collection was conducted with only free, voluntary, informed consent, and all information was stored in protected files under the custody of the principal investigator, thereby preserving participants’ privacy and confidentiality. Data obtained through instruments, techniques, and interviews were used exclusively for the purposes of the study. The nursing home provided adequate spaces that ensured privacy, confidentiality, and compliance with biosafety standards. Participants’ rights were safeguarded in accordance with national and international regulations, ensuring that neither healthcare staff nor the services provided were affected during the research process. The study received approval from the Bioethics Committee, as documented in Minutes No. 007 dated April 17, 2023.
Results
Of the 250 participants, 63.60% (n=159) were female, and 36.40% (n=91) were male, with a median age of 77.6 years (interquartile range [IQR: 70.23–84]). Table 1 presents a comparison between participants in the initial two tertiles of the FUMAT Quality of Life Index (FUMAT-QOLI) and those in the third tertile (highest scores). Statistically significant age differences were identified: participants in terciles 1 and 2 had a median age of 79.84 years (IQR: 72.38–84.95), whereas those in the third tertile had a median age of 73.65 years (IQR: 67.86–79.23) (p < 0.001), indicating a better quality of life among the younger age groups.
Regarding educational level, participants with no education or only primary education were mainly concentrated in the third tertile, whereas those with secondary or professional education were more frequently represented in tertiles 1 and 2. This suggests an association between educational attainment and self-perceived well-being.
Regarding personal medical history, statistically significant associations (p <0.05) were observed among participants with psychiatric, degenerative, and respiratory diseases, as well as among those who reported the use of tranquilizers or antidepressants. Similarly, individuals with mental, cognitive, motor, or multiple disabilities exhibited a lower proportion among those with the highest FUMAT- QOLI scores. Conversely, individuals who reported engaging in regular physical activity and productive activities were concentrated in the third tertile, supporting the positive relationship between active aging and the perception of a better quality of life.
Table 1. Comparison of FUMAT-QOLI tertiles with participant characteristics CharacteristicsTotal % (n) (250)Tertiles 1/2 lower level7–76 (171)Tertile 3 higher level77–93 (79)p-valueSex 0.573 Female 63.60 (159)64.91 (111)60.76 (48) Male 36.40 (91)35.09 (60)39.24 (31)Age, median (IQR) 77.60 [70.23; 84.00]79.84 [72.38; 84.95]73.65 [67.86; 79.23]<0.001 Marital status0.852 Married/Cohabiting 25.15 (43)25.15 (43)24.05 (19) Single/Divorced/Widowed 74.85 (128)74.85 (128)75.95 (60)Level of education 0.002 None 25.60 (64)22.22 (38)32.91 (26) Primary education 55.20 (138)52.63 (90)60.76 (48) Secondary education 8.80 (22)11.11 (19)3.80 (3) Professional education 3.60 (9)4.09 (7)2.53 (2) Do not know / No response 6.80 (17)9.94 (17)0Health insurance regime 0.704 Subsidized80.80 (202)80.70 (138)81.01 (64) Contributory17.60 (44)18.13 (31)16.46 (13) Other 1.60 (4)1.17 (2)2.53 (2)Personal medical history Cardiovascular 63.60 (159)63.74 (109)63.29 (50)1.000 Metabolic 28.00 (70)25.15 (43)34.18 (27)0.172 Psychiatric 38.40 (96)47.37 (81)18.99 (15)<0.001 Degenerative 35.20 (88)42.11 (72)20.25 (16)0.001 Respiratory 16.40 (41)21.05 (36)6.33 (5)0.003 Neoplasia-cancer 4.80 (12)6.43 (11)1.27 (1)0.110 Medications Diuretics 19.20 (48)19.88 (34)17.72 (14)0.687 Tranquilizers 32.80 (82)42.11 (72)12.66 (10)<0.001 Antiparkinsonian 6.00 (15)7.02 (12)3.80 (3)0.401 Antidepressants 27.60 (69)36.26 (62)8.86 (7)<0.001 Antihypertensive 56.40 (141)55.56 (95)58.23 (46)0.692 Impairment Vision impairment 54.00 (135)54.97 (94)51.90 (41)0.650 Hearing loss27.20 (68)29.82 (51)21.52 (17)0.170 Mental 34.80 (87)45.03 (77)12.66 (10)<0.001 Cognitive 35.20 (88)46.78 (80)10.13 (8)<0.001 Motor 36.40 (91)46.20 (79)15.19 (12)<0.001 Multiple 39.20 (98)52.05 (89)11.39 (9)<0.001 Physical activity 52.80 (132)43.86 (75)72.15 (57)<0.001 Productive activity 54.00 (135)43.86 (75)75.95 (60)<0.001P-values: Pearson’s chi-square test and Fisher’s exact test for qualitative variables. Mann-Whitney U test for age.
The medians of the percentiles for the FUMAT-QOLI dimension are shown in Figure 1. The dimensions with the lowest scores were material well-being, with a median of 16 (IQR: 5–37), followed by interpersonal relationships, with a median of 37 (IQR: 19–63). Conversely, the highest scores were observed for the rights dimension, with a median of 84 (IQR: 63–84), and social inclusion, with a median 75 (IQR: 63–84). Overall, the FUMAT-QOLI showed a median score of 65.5 (IQR: 40–79).
Figure 1. Percentiles of dimensions and the FUMAT quality of life indexEWB: Emotional well-being, IR: Interpersonal relationships, MWB: Material well-being, PD: Personal development, W: Physical wellbeing, SDT: Self-Determination, SI: Social inclusion, R: Rights, QoL: Quality of life Index.
In Spearman’s correlation matrix (Figure 2), age exhibited a negative and statistically significant correlation with the FUMAT-QOLI (Rho = –0.29, p < 0.001) and with functional independence, as measured by the Barthel Index (Rho = –0.20, p <0.01). Although both associations were statistically significant, their magnitudes corresponded to weak correlations; therefore, while increasing age tended to be associated with reduced functional independence and quality of life, this relationship was not strong. No statistically significant correlation was identified between age and the PULSES profile of dependence.
Figure 2. Correlation matrix of variablesSpearman’s rho. p-value: * <0.05 ** <0.01 *** <0.001
The strongest correlations were observed between the FUMAT-QOLI and the functional status (Barthel Index) (Rho = 0.5792, p < 0.001), suggesting a direct association between functional autonomy and a better perceived well-being. Similarly, a strong negative correlation was found between FUMAT-QOLI and cognitive impairment (SPMSQ) (Rho = -0.5752, p < 0.001), indicating that cognitive impairment is associated with lower quality of life.
Likewise, significant associations were observed among frailty (FRAIL scale), dependence (PULSES profile), and the risk of falls (Downton Index), with positive correlation coefficients among these measures, indicating their interdependence in the overall functional status of institutionalized older adults.
Table 2 presents the comparison between tertiles of the FUMAT-QOLI and the categories of functional status, dependence, frailty, risk of falls, and cognitive impairment. The results indicate statistically significant associations between the quality-of-life index and the Barthel Index, the PULSES profile, the FRAIL scale, and the SPMSQ (p < 0.001), whereas no statistically significant differences were observed for the Downton Fall Risk Index (p = 0.384).
Table 2. Comparison of FUMAT-QOLI tertiles with functional status, dependence, frailty, risk of falls, and cognitive impairment.CharacteristicsTotal % (n) (250)Percentile FUMAT-QOLI p-valueTertile 1/27–76 (171)Tertile 377–93 (79)Functional status (Barthel Index)<0.001 Total dependence9.60 (24)14.04 (24)0 Severe dependence4.80 (12)7.02 (12)0 Moderate dependence6.40 (16)9.36 (16)0 Mild dependence14.00 (35)15.20 (26)11.39 (9) Independent65.20 (163)54.39 (93)88.61 (70)Dependence (PULSES profile)<0.001 Mild impairment49.20 (123)36.84 (63)75.95 (60) Moderate impairment or dependence15.20 (38)16.37 (28)12.66 (10) Severe impairment or dependence35.60 (89)46.78 (80)11.39 (9)Frailty (FRAIL scale)<0.001 Not frail76.80 (192)68.42 (117)94.94 (75) Frail23.20 (58)31.58 (54)5.06 (4)Downton Fall Risk0.384 Moderate risk2.40 (6)1.75 (3)3.80 (3) High risk97.60 (244)98.25 (168)96.20 (76)Cognitive impairment (SPMSQ)<0.001 Normal60.00 (150)46.20 (79)89.87 (71) Minimal6.00 (15)8.19 (14)1.27 (1) Moderate17.20 (43)21.64 (37)7.59 (6) Severe16.80 (42)23.98 (41)1.27 (1)p-value: Pearson’s chi-square test and Fisher’s exact test
Regarding functional status, as measured by the Barthel Index, the categories of total, severe, and moderate dependence were observed exclusively among participants in tertiles 1 and 2. Conversely, no participants in the third tertile (indicating better quality of life) presented these conditions. In this latter group, 88.61% were classified as independent, compared with 54.39% in the lower tertiles.
With respect to functional dependence (PULSES profile), the mild impairment category predominated in the third tertile (75.95%), whereas severe dependence was more prevalent in tertiles 1 and 2 (46.78%), confirming an inverse relationship between dependence and quality of life.
According to the FRAIL scale, 94.94% of participants in the third tertile were classified as not frail, compared with 68.42% in tertiles 1 and 2. This finding indicates a significant association between lower frailty and better quality of life.
Although no statistically significant differences were observed in the Downton fall risk index, a homogeneous high-risk tendency was maintained across all groups.
Finally, according to Pfeiffer’s SPMSQ, 89.87% of participants in the third tertile were classified as having intact cognitive function, whereas only 46.20% of those in the lower tertiles fell into this category. Moderate and severe impairment levels were concentrated in tertiles 1 and 2, with proportions of 21.64% and 23.98%, respectively, reinforcing the influence of cognitive status on the overall perception of quality of life.
Multivariate analysis showed that participants with cognitive impairment were less likely to be in the highest tertile of the FUMAT-QOLI scores (OR = 0.34, 95% CI: 0.12; 0.91, p = 0.033), as well as participants with motor impairment (OR = 0.30, 95% CI: 0.14; 0.64, p = 0.002). When participants reported engaging in physical activity and productive activities, they showed a greater likelihood of belonging to the group with the highest scores. While these associations were not statistically significant, a trend was identified. See Table 3.
Table 3. Multivariate logistic regression model for belonging to the highest tertile of FUMAT- QOLI scoresVariablesOR (95% CI)p-valueAge0.98 (0.94 - 1.01)0.345Respiratory condition0.39 (0.13 - 1.18)0.099ImpairmentMental0.48 (0.19 - 1.21)0.121Cognitive0.34 (0.12 - 0.91)0.033Motor0.30 (0.14 - 0.64)0.002Physical activity1.70 (0.87 - 3.29)0.116Productive activity2.01 (0.98 - 3.86)0.054p-value: Wald test.
Discussion
The findings of this study have significant implications for nursing practice in the field of gerontology. The association between engagement in productive and physical activities and higher scores on the FUMAT scale underscores the importance of nursing interventions that promote mobility, adapted exercise, and social integration as essential strategies for preserving and enhancing quality of life in older adults. Likewise, identifying cognitive and motor disabilities as factors that reduce quality of life underscores the need for a preventive and early care approach, in which nursing assumes an active role in detecting functional impairments and designing personalized care plans.
The study identified that participation in productive and physical activities is strongly associated with higher scores on the FUMAT scale. Similar results were reported in a study conducted in Chile among older women, which observed significant differences in subjective quality-of-life perceptions between physically active and inactive individuals, with the former reporting higher levels of satisfaction and overall well-being following the COVID-19 pandemic44.
Compared with international studies that have employed the FUMAT scale, the dimension of material well-being exhibited the lowest scores in this study. This finding aligns with regional evidence from Paraguay45, where a study among 33 residents of peri-urban nursing homes in Asunción reported material well-being as one of the lowest-scoring dimensions (45 ± 30). These figures underscore the role of social determinants in quality of life. Studies conducted in Ecuador22, Cúcuta, Colombia46, and Mexico47 reported analogous trends, namely, lower ratings of material well-being compared with other dimensions. By contrast, a study conducted in Spain that employed a short version of the FUMAT scale (24 items) identified social inclusion, self-determination, and physical well-being as the lowest-scoring dimensions. These findings suggest that differences in sociocultural context and in the version of the instrument may modulate the dimensional profiles observed48.
In this study, the dimensions that obtained the highest scores were rights, social inclusion, and self-determination, reflecting a positive perception of aspects related to participation, integration, and personal autonomy. Similar results were observed in a study conducted in Ecuador22 involving 137 older adults, in which the highest-scoring dimensions were self-determination (63 points) and personal development and rights (50 points each). Similarly, a study conducted in Spain24 with a sample of 25 older adults revealed that the highest-scoring dimensions were personal development (57 points), social inclusion (52 points), and physical well-being (45 points). These findings confirmed the consistency of these domains as relevant indicators of perceived well-being in old age.
These results enable the identification of the material well-being dimension of the scale as the lowest-scoring across the different studies, indicating that it remains a factor limiting the quality of life of institutionalized older adults. This finding underscores the importance of strengthening public policies49 to protect the economic well-being of this population.
The present study demonstrated that cognitive and motor impairments significantly impact quality of life, consistent with previous research conducted in similar contexts, in which frailty and cognitive impairment have been identified as determinants of perceived well-being among older adults50–53. These findings enrich the body of knowledge in gerontological nursing by providing local evidence that supports person-centered care practices and encourages professionals to strengthen comprehensive assessment as a basis for effective interventions. Promoting physical activity, preventing cognitive and motor impairments, and ensuring social inclusion not only enhance health outcomes but also reflect nursing’s commitment to the humanization of care for institutionalized older adults.
Another relevant point of comparison emerges from the analysis of the QOLI in relation to mental health variables. In the present study, psychiatric history and the use of tranquilizers or antidepressants were found to be associated with lower quality of life. This finding is consistent with other studies highlighting the negative impact of mental disorders on older adults54. However, the present study underscores the need for nursing interventions aimed at promoting mental health and reducing polypharmacy. These interventions have the potential to enhance the overall well-being of this population55.
Among its strengths, the study provides robust empirical evidence through a solid methodological design based on validated instruments and multivariate analysis. As a result, factors associated with quality of life were identified with high reliability. Furthermore, the research encompasses a substantial sample of older adults, thereby enhancing its external validity and enabling the extrapolation of its findings to similar contexts.
With regard to contributions to nursing practice, education, and research, the study highlights key elements for strengthening care, such as the need to include person-centered interventions that promote physical activity and social participation as effective strategies for improving quality of life in nursing homes56. Furthermore, the role of nursing in assessing physical and cognitive functioning is essential for early detection of impairments that affect quality of life57.
From the perspective of nursing education, new directions emerge for undergraduate and graduate nursing curricula, including the comprehensive assessment of older adults, the use of validated scales in this population, such as the FUMAT scale, and care planning focused on the dimensions of material, emotional, and social well-being26. In this way, nursing professional competence can be strengthened, promoting active aging among individuals both within and without institutionalization.
Amongthe limitations tobe considered, first, the study was conducted in a single nursing home, limiting the generalizability of the results to other older adult populations with different sociodemographic characteristics or living conditions.
Regarding future lines of research, it would be relevant to conduct longitudinal studies to assess changes in quality of life in this population over time and to identify more accurate predictors. Examples include a study conducted in Spain that examined the effects of a community-based home care intervention58; research in Peru reporting the impact of a social program among older adults living in extreme poverty, with the participation of 634 older adults59; and studies assessing outcomes in nursing homes involving individuals with cognitive impairment56. It is also recommended to expand the research to different types of older people’s homes, including urban and rural settings60, to evaluate potential variations in quality of life according to context, including hospital settings61.
In view of the above, new lines of research may be considered to evaluate the effects of nursing interventions on the prevention or limitation of disability and cognitive impairment. In this way, best care practices can be explored that foster the inclusion and social participation of older adults across different clinical and community settings, including nursing homes.
Furthermore, it would be relevant to consider validating the 24-item FUMAT scale62. Measuring quality of life in individuals with intellectual disabilities or multiple disabilities63 also remains a challenge, as does examining the effects of various interventions, such as physical activity plans, dance programs, music therapy64–67, and the prevention of polypharmacy68, among others that involve the role of gerontological nursing. These efforts would contribute to continued progress toward excellence in care, promoting humanized care, active aging, and dignified treatment of older adults.
Conclusions
This study highlights the positive influence of participation in productive activities and physical activity on the quality of life of older adults and encourages health professionals to prioritize the prevention of cognitive and motor impairments in this population. Furthermore, this study makes a significant contribution to the strengthening of gerontological practice by identifying key factors that impact the quality of life of institutionalized older adults.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Organización Mundial de la Salud Reunión de Ministros de Salud del G 7 en Kobe: alcanzar la cobertura sanitaria universal centrándose en el envejecimiento saludable y activo [Internet]201623 enero 09, 2025 https://www.who.int/es/director-general/speeches/detail/g 7-kobe-health-ministers-meeting-attaining-universal-health-coverage-focusing-on-healthy-and-active-ageing
- 2DANE. Departamento Administrativo Nacional de Estadística Colombia registró la tasa de nacimientos más baja de la última década y crecieron las defunciones relacionadas con enfermedades transmitidas por mosquitos 2024 octubre 07, 2025 https://www.dane.gov.co/files/operaciones/EEVV/cp-EEVV-Itrim 2024.pdf
- 3Word Health Organization Ageing and health 202569 octubre 07, 2025 https://www.who.int/news-room/fact-sheets/detail/ageing-and-health
- 4Stephany T Nursing and aging Am J Nurs 2019119101010.1097/01.NAJ.0000586068.10122.4331567226 · doi ↗ · pubmed ↗
- 5García L Quevedo M La Rosa Y Leyva A Calidad de vida percibida por adultos mayores Revsita Electrónica Medinay 20202711625 https://www.medigraphic.com/pdfs/revciemedhab/cmh-2020/cmh 201c.pdf
- 6Gómez L Verdugo M Arias B Navas P Evaluación de la calidad de vida en personas mayores y con discapacidad : la Escala Fumat Interv Psicosoc 20081718999 https://journals.copmadrid.org/pi/art/5938 b 4d 054136 e 5d 59ada 6ec 9c 295d 7a?utm_source=chatgpt.com
- 7Ministerio de Salud y Protección Social de Colombia Decreto 681 de 2022. Por medio del cual se adiciona el capitulo 7 al Tiyulo 2 de la parte 9 del Libro 2 del Decreto 780 de 2016 relativo a la Politica Publica Nacional de Envejecimiento y Vejez 2022-20312022 https://www.minsalud.gov.co/Normatividad_Nuevo/Decreto%20No.%20681%20de%202022.pdf
- 8Venegas-Sanabria C Iván Cavero-Redondo I Martínez-Vizcaino V Cano-Gutierrez A Álvarez- Bueno C Effect of multicomponent exercise in cognitive impairment : a systematic review and meta - analysis BMC Geriatr 20222261710.1186/s 12877-022-03302-1PMC 931633435879665 · doi ↗ · pubmed ↗