Comparative Outcomes of Fully Threaded Headless Compression Screws and Partially Threaded Screws in Medial Malleolus Fracture Fixation: A Systematic Review and Meta-Analysis
Ward Hamsho, Muhammad Y Raufi, Mohamed Elgendy, Mohamed Elrouby, Mohammad Alnajjar

TL;DR
This study compares two types of screws used to treat ankle fractures and finds that one type causes fewer complications and fewer follow-up surgeries.
Contribution
The study provides a systematic review and meta-analysis comparing clinical outcomes of fully threaded headless compression screws versus partially threaded screws in medial malleolus fractures.
Findings
Fully threaded headless compression screws significantly reduce the risk of symptomatic hardware and implant removal.
Functional outcomes and union rates are comparable between the two screw types.
Post-operative pain is significantly lower with fully threaded headless compression screws.
Abstract
Medial malleolus fractures are common injuries, and screw fixation is the standard treatment. The choice between fully threaded headless compression screws (FTHCSs) and partially threaded screws (PTSs) remains controversial, particularly regarding soft-tissue irritation and reoperation rates. This systematic review and meta-analysis aimed to compare the clinical and functional outcomes of FTHCSs versus PTSs for medial malleolus fracture fixation. This review was conducted according to the PROSPERO protocol (Registration ID: CRD420251170989) and Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. A systematic search identified comparative studies evaluating FTHCSs against PTSs for medial malleolus fractures. Data, including functional scores of the American Orthopaedic Foot and Ankle…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
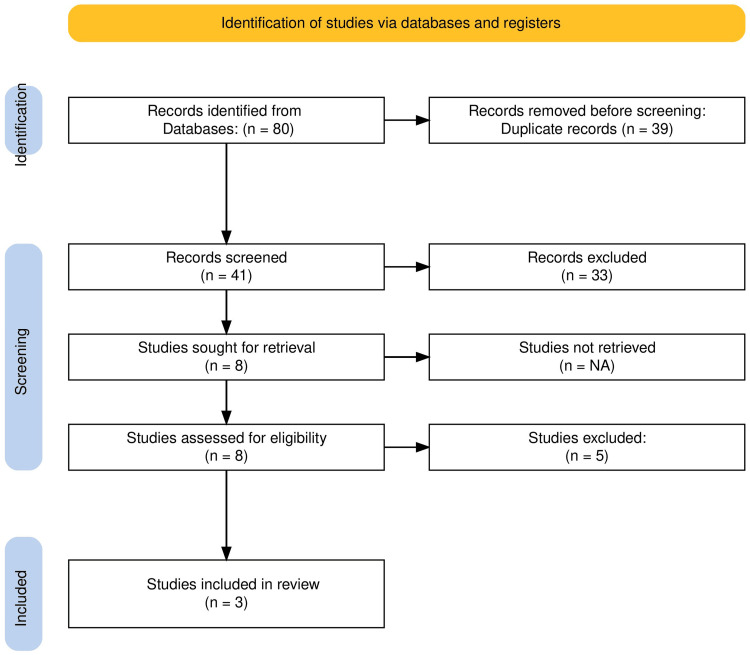 Figure 1
Figure 1 Figure 2
Figure 2 Figure 3
Figure 3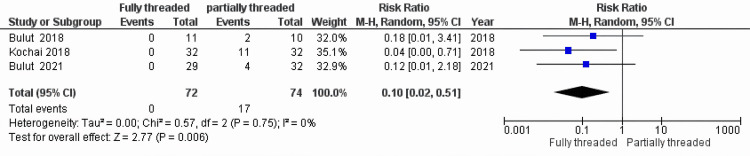 Figure 4
Figure 4| MINORS Criteria | Bulut et al. (2021) [ | Bulut et al. (2018) [ | Kochai et al. (2018) [ |
| 1. Clearly stated aim | 2 | 2 | 2 |
| 2. Inclusion of consecutive patients | 1 | 1 | 1 |
| 3. Prospective collection of data | 0 | 0 | 0 |
| 4. Endpoints appropriate to study aim | 2 | 2 | 2 |
| 5. Unbiased assessment of study endpoint | 1 | 1 | 1 |
| 6. Follow-up period appropriate | 2 | 2 | 2 |
| 7. Lost to follow-up <5% | 1 | 0 | 2 |
| 8. Prospective calculation of study size | 0 | 0 | 0 |
| 9. Adequate control group | 2 | 2 | 2 |
| 10. Contemporary groups | 2 | 2 | 2 |
| 11. Baseline equivalence of groups | 1 | 1 | 0 |
| 12. Adequate statistical analyses | 2 | 2 | 1 |
| Total Score (max 24) | 16 | 15 | 15 |
| Study (Year) | Design | Total Patients (N) | FTHCS Male (n) | FTHCS Female (n) | PTS Male (n) | PTS Female (n) | PTS Age (mean±SD) | FTHCS Age (mean±SD) | Mean Follow-up (months) | Fracture Type |
| Bulut et al. (2021) [ | Retrospective Comparative | 61 | 15 | 14 | 17 | 15 | 42±15.6 | 43.7±13.1 | 22.1 | Isolated/Bi-/Trimalleolar |
| Bulut et al. (2018) [ | Retrospective Comparative | 21 | 8 | 3 | 8 | 2 | 30.4±8.5 | 37.6±14.1 | 22.5–27 | Isolated |
| Kochai et al. (2018) [ | Retrospective Comparative | 64 | 24 | 8 | 23 | 9 | ≈36.8±9 | ≈37.8±9.8 | 55–58 | Isolated |
| Total | 146 | 47 | 25 | 48 | 26 |
| Study (year) | Bulut et al. (2021) [ | Bulut et al. (2018) [ | Kochai et al. (2018) [ |
| AOFAS PTS | 92.6 | 93.1 | 85.6 |
| AOFAS FTHCS | 95.1 | 96.7 | 86.4 |
| AOFAS P value | p=0.136 | p=0.239 | p=0.73 |
| VAS PTS | 2.1 | 2.7 | - |
| VAS FTHCS | 0.2 | 0.09 | - |
| VAS P value | p<0.001 | p=0.003 | - |
| Hardware Removal PTS | 4 | 2 | 11 |
| Hardware Removal FTHCS | 0 | 0 | 0 |
| Hardware removal P value | p=0.114 | p=0.233 | p=0.037 |
| Symptomatic Hardware PTS | 21 | 7 | 11 |
| Symptomatic Hardware FTHCS | 4 | 1 | 0 |
| Symptomatic Hardware P value | p<0.001 | p = 0.004 | p=0.037 |
| Time to Union PTS (weeks) | 9.6 | ≈10.9 | 12 |
| Time to Union FTHCS (weeks) | 9.5 | ≈9.6 | 9 |
| Time to Union P value | p=0.827 | p=0.448 | p<0.0001 |
| Union Rate | 100% (both groups) | 100% (both groups) | 100% (both groups) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsFoot and Ankle Surgery · Lower Extremity Biomechanics and Pathologies · Bone fractures and treatments
Introduction and background
Medial malleolus fractures are among the most common ankle injuries, frequently occurring in isolation or as part of bi- or trimalleolar fracture patterns [1]. Anatomical reduction and stable internal fixation are crucial for restoring ankle joint congruity and achieving optimal long-term outcomes [2]. The gold standard for fixation is typically a lag screw technique, which utilizes a partially threaded screw (PTS) to generate interfragmentary compression [3]. Alternative fixation options, such as tension band wiring, have also been described for specific fracture patterns [3]. So far, AO principles have recommended using 4-mm partially threaded screws to achieve that [4]. While effective for compression, the prominent head of the PTS, which often lies directly beneath the thin soft-tissue envelope of the medial malleolus, is a well-recognized source of soft-tissue irritation, pain, and subsequent need for implant removal [5]. This has led to the increasing use of fully threaded headless compression screws (FTHCSs), which can be countersunk below the articular surface or bone cortex, theoretically mitigating hardware-related complications while still providing interfragmentary compression and stability [6]. Despite the theoretical advantages of FTHCSs, there is a lack of consensus regarding their superiority over traditional PTSs in terms of clinical and functional outcomes. Specifically, it is unclear whether the reduced hardware prominence translates into better functional scores or lower reoperation rates without compromising fracture union. The objective of this systematic review and meta-analysis was to compare the clinical and functional outcomes of FTHCSs versus PTSs for medial malleolus fracture fixation. Our primary hypothesis was that FTHCSs would be associated with a lower rate of hardware-related complications and reoperations while maintaining non-inferior union rates and functional scores.
Review
Methods
Protocol and Registration
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [7]. The protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (Registration ID: CRD420251170989).
Search Strategy and Study Selection
A systematic electronic search was performed in PubMed, Embase, and the Cochrane Library (CENTRAL) from inception to October 2025. The search strategy combined terms related to the intervention ("Fully threaded" OR "headless" OR "Compression"), the comparator ("Partially threaded" OR "Lag"), and the condition ("medial malleolus" OR "medial malleolar"). No language or publication date restrictions were applied.
Two independent reviewers screened titles and abstracts manually using a standardized electronic data collection sheet (Excel), followed by full-text review of potentially eligible articles. Disagreements were resolved by consensus with a third reviewer. Inclusion criteria were (1) adult patients (≥18 years) with medial malleolus fractures; (2) studies comparing FTHCSs with PTS fixation; and (3) reporting on at least one clinical or functional outcome. Exclusion criteria included non-human studies, case reports, abstracts, and reviews. The study selection process is detailed in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram (Figure 1) [7].
PRISMA flow diagram. Flowchart detailing the study selection process, from initial search results to the final inclusion of three studies in the systematic review and meta-analysis. PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Data Extraction and Risk of Bias Assessment
Data extraction was performed independently by two reviewers using a standardized electronic form. Extracted variables included study design, patient demographics, fracture type, follow-up duration, and outcomes (union rate, time to union, complications, reoperation, AOFAS score, and VAS pain). The methodological quality of the included non-randomized comparative studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) checklist [8]. A score of 0, 1, or 2 was assigned to each of the 12 items, with a maximum score of 24 (Table 1).
Data Synthesis and Statistical Analysis
If two or more studies reported comparable outcomes, a meta-analysis was performed where appropriate. For dichotomous outcomes (symptomatic hardware, implant removal), the risk ratio (RR) with 95% CI was calculated. For continuous outcomes (AOFAS score), the mean difference (MD) with 95% CI was calculated.
A random-effects model (Mantel-Haenszel for RR, inverse variance for MD) was used for all pooled analyses to account for potential clinical and methodological heterogeneity among the included studies. Statistical heterogeneity was quantified using the I² statistic, where values of 0% to 40% were considered low, 30% to 60% moderate, and 50% to 90% substantial [10]. For the visual analog scale (VAS) pain scores, formal meta-analysis was not performed as only two studies [5,9] reported VAS outcomes, both demonstrating statistically significant reductions in pain for the FTHCS group. Given the limited number of studies, quantitative pooling was unlikely to provide additional meaningful insight; therefore, VAS outcomes were summarized narratively. All statistical analyses were performed using Review Manager (RevMan5.4).
Publication bias was not formally assessed due to the small number of included studies (n=3).
Quality of Evidence Assessment
Given that all included studies are retrospective comparative studies (Level III evidence) with moderate MINORS scores, the overall quality of evidence for all outcomes will be rated as low or very low according to the GRADE approach, primarily due to the risk of bias and study design limitations [11].
Results
Study Characteristics
The systematic search yielded three retrospective comparative studies [5,6,9] that met the inclusion criteria, involving a total of 146 patients. All included studies were published between 2018 and 2021 and originated from Turkey. Table 2 describes the characteristics of the included studies.
Functional Outcome: American Orthopaedic Foot and Ankle Society (AOFAS) Scores
The pooled analysis of the AOFAS score included all three studies (Figure 2) [5,6,9]. The FTHCS group showed a MD of 1.64 points (95% CI: -0.01, 3.28) compared to the PTS group. This difference was marginally statistically significant (P=0.05), although it demonstrated a trend favouring FTHCS. Statistical heterogeneity was negligible (I²=0%) (Table 3).
Forest plot for the functional outcome - American Orthopaedic Foot and Ankle Society (AOFAS) scores.Meta-analysis of the mean difference (MD) in AOFAS scores between the fully threaded headless compression screw (FTHCS) and partially threaded screw (PTS) groups. The diamond represents the pooled effect size and 95% CI.Bulut et al. (2018) [9]; Kochai et al. (2018) [6]; Bulut et al. (2021) [5]
Symptomatic Hardware
The meta-analysis for symptomatic hardware included all three studies (Figure 3) [5,6,9]. The pooled RR was 0.17 (95% CI: 0.08, 0.38), which was highly statistically significant (P < 0.0001). This indicates that FTHCS fixation is associated with an 83% reduction in the risk of developing symptomatic hardware compared to PTS. Statistical heterogeneity was negligible (I²=0%) (Table 3).
Forest plot for symptomatic hardware.Meta-analysis of the risk ratio (RR) for symptomatic hardware between the FTHCS and PTS groups. The diamond represents the pooled effect size and 95% CI.Bulut et al. (2018) [9]; Kochai et al. (2018) [6]; Bulut et al. (2021) [5]FTHCS: Fully threaded headless compression screw; PTS: Partially threaded screw
Implant Removal
The meta-analysis for implant removal included all three studies (Figure 4) [5,6,9]. The pooled RR was 0.10 (95% CI: 0.02, 0.51), which was statistically significant (P = 0.006). This suggests that FTHCS fixation is associated with a 90% reduction in the risk of requiring secondary surgery for implant removal compared to PTS. Statistical heterogeneity was negligible (I²=0%) (Table 3).
Forest plot for implant removal.Meta-analysis of the risk ratio (RR) for implant removal between the FTHCS and PTS groups. The diamond represents the pooled effect size and 95% CI.Bulut et al. (2018) [9]; Kochai et al. (2018) [6]; Bulut et al. (2021) [5]FTHCS: Fully threaded headless compression screw; PTS: partially threaded screw
Other Clinical Outcomes
Union rate and time to union: All three studies reported a 100% union rate in both the FTHCS and PTS groups, with no reported non-unions [5,6,9]. Regarding time to union, only Kochai et al. [6] reported a significant difference, favouring FTHCSs (9 weeks vs. 12 weeks, P<0.0001). The other two studies found no significant difference (Table 3).
Pain scores (VAS): Two studies [5,9] reported significantly lower VAS pain scores in the FTHCS group compared to the PTS group (P<0.001 and P=0.003, respectively) (Table 3). These outcomes are presented as a narrative synthesis, as explained in the Data Synthesis and Statistical Analysis section, due to the limited number of studies reporting VAS.
Discussion
This systematic review and meta-analysis, encompassing 146 patients from three comparative studies, provides quantitative evidence on the use of FTHCSs versus PTSs for medial malleolus fracture fixation. The most compelling finding is the significant reduction in hardware-related complications associated with FTHCSs. Specifically, FTHCSs reduced the risk of symptomatic hardware by 83% and the risk of implant removal by 90% compared to PTSs.
The primary mechanism for this difference is likely the design of the FTHCS, which allows for complete countersinking beneath the bone surface, eliminating the soft-tissue irritation caused by the prominent head of the PTS [5]. Given that the need for implant removal is a major cause of reoperation and patient morbidity following ankle fracture fixation, this finding has significant clinical implications. The high rate of implant removal in the PTS group (up to 34% in the study by Kochai et al. [6]) highlights a substantial drawback of this traditional technique.
In terms of functional outcome, the pooled AOFAS score showed a borderline statistically significant trend favouring FTHCSs (MD = 1.64, P=0.05). While this difference is marginally statistically significant, it shows that the FTHCS is potentially better in restoring function. Furthermore, the narrative synthesis of pain scores, with two studies reporting significantly lower VAS scores for FTHCSs, aligns with the reduced symptomatic hardware and supports the overall functional benefit of FTHCSs.
Crucially, the FTHCS group demonstrated comparable fracture healing, with a 100% union rate in all included studies, suggesting that the mechanical stability provided by FTHCS is sufficient for medial malleolus fixation. The one study that reported a significantly shorter time to union with FTHCSs suggests a potential biological advantage, possibly due to the uniform compression along the entire screw length [6], but this requires confirmation from further studies.
Limitations
The findings of this meta-analysis must be interpreted in light of several limitations. First, only three studies were included with a small total sample size (146 patients), all of which were retrospective comparative studies (Level III evidence) with a moderate risk of bias (MINORS scores 15-16/24). The lack of high-quality randomized controlled trials significantly limits the strength of the evidence. Second, all included studies originated from a single country (Turkey), which may limit the generalizability of the findings, and two of them were done by the same author. Third, the small number of studies precluded a formal assessment of publication bias. Finally, there was clinical heterogeneity in the inclusion of both isolated and bi-/trimalleolar fractures in one study [5], although the statistical heterogeneity was low for the pooled outcomes.
Conclusions
Despite the limitations, the consistent and statistically significant findings regarding symptomatic hardware, good functional outcomes, and implant removal strongly support the use of FTHCSs for medial malleolus fracture fixation. Future research should focus on high-quality, multi-center randomized controlled trials to confirm these findings and to perform a robust cost-effectiveness analysis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Epidemiology of adult fractures: a review Injury Court-Brown CM Caesar B 6916973720061681478710.1016/j.injury.2006.04.130 · doi ↗ · pubmed ↗
- 2Fractures of the lower end of the tibia into the ankle Injury Rüedi T 13013451973477476410.1016/s 0020-1383(73)80089-0 · doi ↗ · pubmed ↗
- 3The Rationale of Operative Fracture Care Schatzker J Tile M Berlin, Heidelberg Springer 2005
- 4Medial, transverse fracture: lag screws 11 2025 2025 https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/malleoli/basic-technique/medial-transverse-fracture-lag-screws
- 5Fully threaded headless compression screw versus partially threaded cancellous lag screw in medial malleolus fractures: clinical and radiological outcomes Eur J Trauma Emerg Surg Bulut T Gursoy M Ertem H 1791854720213145599010.1007/s 00068-019-01207-0 · doi ↗ · pubmed ↗
- 6A comparative study of three commonly used fixation techniques for isolated medial malleolus fracture Eklem Hastalik Cerrahisi Kochai A Türker M ÇiçekliÖ Özdemir U Bayam L ErkorkmazÜ Şükür E 104109292018 https://pubmed.ncbi.nlm.nih.gov/30016610/3001661010.5606/ehc.2018.61449 · doi ↗ · pubmed ↗
- 7The PRISMA 2020 statement: an updated guideline for reporting systematic reviews Syst Rev Page MJ Mc Kenzie JE Bossuyt PM 891020213378134810.1186/s 13643-021-01626-4PMC 8008539 · doi ↗ · pubmed ↗
- 8Methodological index for non-randomized studies (minors): development and validation of a new instrument ANZ J Surg Slim K Nini E Forestier D Kwiatkowski F Panis Y Chipponi J 7127167320031295678710.1046/j.1445-2197.2003.02748.x · doi ↗ · pubmed ↗