A Heart Under Stress: Anaesthetic Strategy for a Pregnant Patient With Long QT Syndrome
Maria J Nascimento, Marta Silva, Ana Bernardino, Joana Carvalhas

TL;DR
This paper discusses the safe anesthetic management of a pregnant woman with Long QT Syndrome during a caesarean section.
Contribution
The paper presents a novel anaesthetic strategy for managing LQTS1 patients during childbirth.
Findings
Total intravenous anaesthesia with propofol and remifentanil was safely used in a high-risk LQTS1 patient.
Multidisciplinary planning and monitoring minimized arrhythmic risks during the procedure.
Electrolyte optimization and sympathetic control were critical for successful outcomes.
Abstract
Long QT syndrome (LQTS) is a cardiac channelopathy associated with a high risk of malignant arrhythmias. Hormonal changes during pregnancy, especially in the peripartum period, increase the risk of adverse cardiac events in women with LQTS. Anaesthetic management in these patients is challenging, as there are no established guidelines and most anaesthetic agents prolong the QT interval. This report describes the anaesthetic management of an elective caesarean section in a 34-year-old pregnant woman, 35 weeks pregnant, with congenital LQTS type 1 (LQTS1), a corrected QT interval (QTc) of 597 milliseconds (ms) on the admission day, and a high cardiovascular risk. Given the high arrhythmic risk, perioperative planning and management were undertaken by a multidisciplinary team to optimise patient outcomes and minimise risks. Total intravenous anaesthesia with propofol and remifentanil was…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
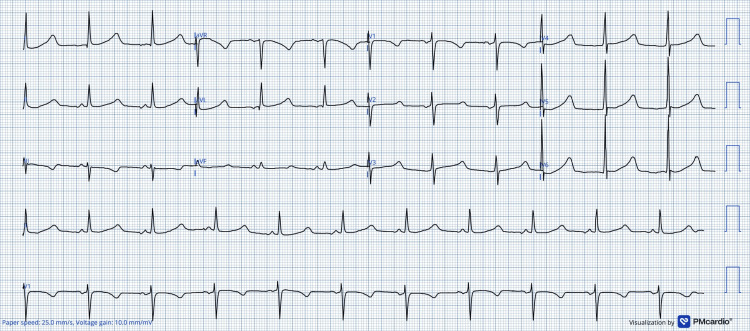 Figure 1
Figure 1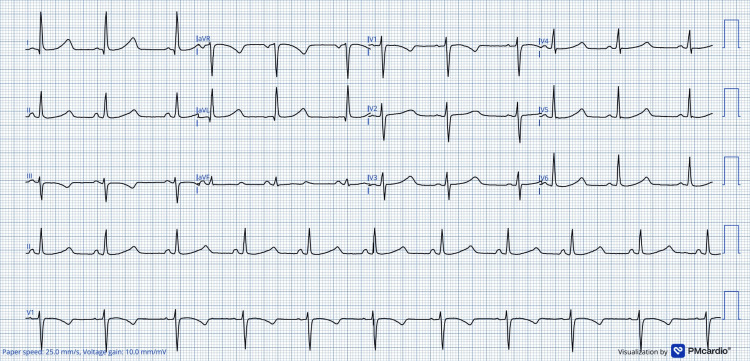 Figure 2
Figure 2 Figure 3
Figure 3| Timepoint | QTc / ECG findings | Electrolytes | Key interventions | Clinical outcome |
| Admission (31 weeks’gestation) | QTc 597 ms; Maternal high-risk LQTS1; Suspected foetal AV block | Persistent low potassium (<3.8 mmol/L) and magnesium (<1.9 mg/dL) | Increased beta-blocker dose; IV potassium and magnesium supplementation; Spironolactone added; Multidisciplinary planning | QTc improved after optimisation |
| Preoperative period (35 weeks’ gestation) | QTc 457 ms | Optimised or within target range | ICD interrogation; Avoidance of QT-prolonging drugs; Plan for elective caesarean section | Patient prepared for elective caesarean section |
| Induction and maintenance | Five-lead ECG and defibrillation pads applied as precaution; Arterial line; No arrhythmias reported | Monitored; Mild hypokalaemia corrected intraoperatively | Midazolam 2 mg; MgSO₄ 2 g; Remifentanil infusion; Induction with lidocaine, propofol and rocuronium; Maintenance with TIVA | Stable induction; Successful intubation; Haemodynamically stable |
| Delivery | No arrhythmias reported | — | Remifentanil stopped 3 minutes before delivery | Neonate APGAR 8/9/9 |
| Post-delivery | No arrhythmias reported | Continued monitoring | Multimodal analgesia with fentanyl, paracetamol, ketorolac and TAP block; Uterotonics: sulprostone and misoprostol; MgSO₄ 2 g | Uneventful emergence and extubation |
| Postoperative period | Maternal course uneventful | Maintained | Cardiac intensive care unit monitoring for 72 hours | No arrhythmic events |
| Neonatal assessment | Neonatal ECG with prolonged QTc | — | Beta-blocker therapy initiated | Follow-up with cardiology |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac electrophysiology and arrhythmias · Ion channel regulation and function · Cardiovascular Issues in Pregnancy
Introduction
Long QT syndrome (LQTS) is a life-threatening cardiac channelopathy caused by abnormal ion channel function, leading to prolongation of ventricular repolarisation and predisposing affected individuals to malignant arrhythmias such as polymorphic ventricular tachycardia (VT) [1]. These arrhythmias may result in syncope or sudden cardiac death (SCD) [1]. LQTS affects approximately 1 in 2,000 individuals and is primarily inherited [1]. Approximately 80-90% of cases are linked to mutations in three specific genes - KCNQ1 (LQTS1), KCNH2 (LQTS2), which are potassium-channel genes, and SCN5A (LQTS3), a sodium-channel gene [2,3]. Congenital LQTS may manifest at any stage of life and can be detected from the foetal period to adulthood [4].
Diagnosis relies on electrocardiographic findings, clinical presentation and genetic analysis [3]. A prolonged QT interval on an electrocardiogram (ECG) is the key indicator for an LQTS diagnosis. The normal range of QTc differs by age and sex, with prolonged QTc being defined as >470 ms in women older than 15 years [5]. Women with LQTS generally exhibit longer QT intervals and a higher risk of VT or SCD compared with men, largely due to hormonal fluctuations throughout the menstrual cycle, pregnancy and the postpartum period. Consequently, pregnancy and the peripartum period are associated with an increased arrhythmic risk in this population [1,2,5].
While cardiovascular management of pregnant patients with LQTS is relatively well-described, specific guidelines for anaesthetic management remain unavailable [1,3]. Published literature on anaesthetic management in pregnant women with congenital LQTS is limited to small case series and isolated case reports, with no consensus regarding the optimal anaesthetic technique, particularly in high-risk patients [3]. Given the lack of established anaesthetic guidelines for these patients, multidisciplinary planning is essential to ensure maternal and foetal safety [1,2].
Case presentation
A primigravida in her 30s, with a known diagnosis of LQTS1, was hospitalised at 31 weeks of gestation following the identification of an atrioventricular (AV) block on routine foetal echocardiography, raising suspicion of foetal LQTS. She had been under close surveillance throughout pregnancy, including beta-blocker adjustments and electrolyte monitoring.
Her medical history included two cardiac ablations and implantable cardioverter-defibrillator (ICD) implantation due to sustained VT and recurrent cardiogenic syncope, despite beta-blockers and left sympathectomy.
At admission, her QTc interval was markedly prolonged at 597 ms (Figure 1), necessitating enhanced monitoring and therapeutic adjustments, including an increased beta-blocker dose, the addition of oral spironolactone, and intravenous potassium and magnesium supplementation, due to persistently low serum levels.
Admission ECGECG performed on hospital admission showing marked QTc prolongation (QTc 597 ms). A digital ECG converter was used to increase the resolution of the original image.
A multidisciplinary meeting involving anaesthesiologists, obstetricians and cardiologists concluded that she was a high-risk patient and an elective caesarean delivery at 35 weeks was the safest course of action. This decision aimed to pre-empt the risks of prolonged maternal intravenous ion supplementation, the potential for spontaneous labour triggering life-threatening arrhythmias and recurrent episodes of foetal bradycardia due to AV block.
ICD interrogation confirmed appropriate function. Her last shock occurred at seven weeks of gestation, triggered by anxiety. Multiple anxiety episodes during hospitalisation were managed with alprazolam 1 mg.
Preoperative blood analysis was normal, and therapeutic adjustments reduced her QTc to 457 ms (Figure 2).
Preoperative ECGECG obtained following pharmacologic and electrolyte optimisation, demonstrating substantial QTc improvement (QTc 457 ms) prior to elective caesarean delivery. A digital ECG converter was used to increase the resolution of the original image.
On the day of the surgery, American Society of Anesthesiologists (ASA) standard monitoring was implemented. The ICD remained active, with defibrillation pads and a five-lead ECG applied as precaution. An arterial line was placed. Bispectral index (BIS), neuromuscular monitoring (TOF) and urine output were continuously monitored.
Prior to anaesthetic induction, the patient received 2 mg of midazolam and 2 g of magnesium sulphate. A remifentanil infusion was initiated at 0.03 µg/kg/min. Rapid sequence induction was performed using 1 mg/kg lidocaine, 2.5 mg/kg propofol and 1 mg/kg rocuronium. Intubation was successful using videolaryngoscopy.
Anaesthesia was maintained with total intravenous anaesthesia (TIVA) of propofol (target controlled infusion effect-site of 3 µg/mL) and remifentanil titrated to 0.08 µg/kg/min. Dexamethasone 4 mg was administered.
Remifentanil was discontinued three minutes before delivery. The newborn had APGAR (Appearance, Pulse, Grimace, Activity, Respiration) scores of eight, nine, and nine. Post-delivery analgesia included 200 µg fentanyl, 1 g paracetamol, and 30 mg ketorolac. Sulprostone and misoprostol were used as uterotonics.
The patient remained stable, with no arrhythmias. Mild hypokalaemia was corrected intraoperatively. Before extubation, 2 g magnesium sulphate and a bilateral transversus abdominis plane (TAP) block with 0.2% ropivacaine (30 mL per side) were administered. Sugammadex was used for reversal. Extubation occurred under remifentanil 0.02 µg/kg/min.
She was monitored for 6 hours in the post-anaesthesia care unit and then transferred to the cardiac intensive care unit, where she remained for 72 hours. The immediate postpartum period was uneventful. Postoperative pain management included paracetamol and ketorolac.
The newborn's ECG, performed three hours after birth, showed prolonged QTc (Figure 3), and beta-blocker therapy was started. Both mother and baby continued follow-up with cardiology after hospital discharge.
Partial ECG of the newbornPostnatal partial ECG from the newborn, due to poor technical quality, revealing marked QTc prolongation (QTc 600 ms), supporting the diagnosis of congenital LQTS and guiding early therapeutic intervention. A digital ECG converter was used to increase the resolution of the original image.
Table 1 summarises the timeline of key clinical parameters, perioperative interventions and outcomes.
Discussion
Pregnancy-related hormonal changes affect cardiac repolarisation, increasing arrhythmic risk [1,2]. Labour and delivery further elevate this risk through sympathetic stimulation and exposure to QT-prolonging drugs [3,4,6].
LQT1 is particularly susceptible to arrhythmias triggered by adrenergic stimulation or emotional stress [1,5]. Beta-blockers are the cornerstone of treatment during and after pregnancy, significantly reducing adverse cardiac events, particularly in LQT1 [3,5]. In high-risk cases, ICD placement and left cardiac sympathetic denervation are adjunctive strategies [3].
Preoperative evaluation and multidisciplinary planning are critical for anaesthetic management [1,2], including a careful review of electrolytes such as potassium, magnesium and calcium, which influence QT dynamics [3,4].
The patient was deemed at high risk for peripartum cardiac events due to her history of recurrent VT despite multiple interventions, her elevated emotional stress levels, highlighted by an ICD shock triggered by an anxiety episode early in pregnancy, and her markedly prolonged QTc on admission [1,2]. Caesarean delivery is preferred in high-risk LQTS patients [1].
A thorough preoperative evaluation included a medical history review, physical examination and medication screening to avoid QT-prolonging drugs. Beta-blockers were continued throughout the perioperative period as recommended [1-5]. A 12-lead ECG and laboratory tests, particularly serum electrolytes, were assessed and optimised, as electrolyte imbalances, such as hypokalaemia, hypomagnesaemia, and hypocalcaemia, can exacerbate QT prolongation [3,5]. Intravenous potassium and magnesium supplementation was initiated to correct persistent electrolyte abnormalities. Spironolactone was also added for its potassium-sparing effect to support the correction and stabilisation of serum potassium levels. Through these therapeutic adjustments, the patient’s QTc was successfully reduced to normal values before caesarean delivery, illustrating that QTc can be significantly improved with optimisation strategies.
Sympathetic modulation is a critical goal in preventing life-threatening arrhythmias in pregnant patients with LQTS [1-3]. However, there are no clinical trials defining optimal anaesthetic management in this population, and current evidence is largely derived from case reports and small series [1,3,4,7].
Several case reports have described the safe use of epidural or combined spinal-epidural anaesthesia in patients with LQTS [1]. In contrast, single-shot spinal anaesthesia is generally discouraged due to the potential for abrupt haemodynamic changes, which may increase the risk of malignant arrhythmias or other adverse cardiac events. Epidural anaesthesia is associated with more gradual haemodynamic changes and is therefore often preferred over spinal techniques [1,3]. Nevertheless, a major limitation of neuraxial anaesthesia is the risk of high sympathetic blockade, which may result in hypotension and bradycardia, parasympathetic predominance and the subsequent need for sympathomimetic agents that can further prolong the QTc interval [1,3,4].
Although epidural anaesthesia is typically safe [1,3,7], it was relatively contraindicated in this case due to severe anxiety and previous arrhythmic responses to emotional stress. In patients with LQT1, severe anxiety is a well-recognised trigger for arrhythmias [1,3,4], supporting the decision to pursue general anaesthesia. General anaesthesia was also chosen to allow better haemodynamic control and rapid intervention in the event of an acute cardiac episode. In addition, suspected foetal LQTS further increased maternal anxiety, reinforcing the choice of general anaesthesia as the preferred approach to mitigate stress-related arrhythmogenic triggers.
General anaesthesia for LQTS requires careful planning and execution. As referred to before, anxiety can precipitate arrhythmias; thus, anxiolytic premedication is recommended [3]. Midazolam was used, as it does not prolong QTc or disrupt cardiac conduction [3]. Normothermia, oxygen supplementation and normocapnia were ensured to avoid additional QT-prolonging triggers [3,8].
Sympathetic stimulation during induction and emergence was managed with opioids and lidocaine to blunt the sympathetic response [3,4]. Prophylactic intravenous magnesium sulphate (2-4 g) was also given to mitigate the risk of VT, as it can effectively prevent and terminate VT [3,5].
Pain is also a trigger to adrenergic response, so optimal analgesic management is required [3,4]. Opioids such as fentanyl or remifentanil blunt hemodynamic response and are considered useful and safe in patients with LQTS [4,8]. Remifentanil was chosen for its short half-life and rapid metabolism, with infusion discontinued just before umbilical cord clamping to minimise neonatal opioid exposure.
Propofol-based TIVA was utilised due to its favourable QT profile. Other intravenous anaesthetics, such as etomidate and thiopental, prolong the QTc interval more than propofol, and all halogenated volatile anaesthetics are also known to extend QTc [3,4,6].
Non-depolarising neuromuscular blockers are generally safe, while succinylcholine should be avoided due to its potential for QT prolongation and vagal-induced asystole [3,4,8]. Neuromuscular block reversal with sugammadex was preferred over anticholinesterase-anticholinergic reversal [3,8,9].
Postoperative nausea and vomiting prophylaxis should not be performed with first-generation 5-HT3 receptor antagonists or droperidol, as they can also prolong QTc [4,6]. Metoclopramide and dexamethasone can be safely administered in these patients [3,4]. Despite a high Apfel score, only dexamethasone was used to minimise QT-prolongation risks, with TIVA contributing as a nausea-reducing strategy.
Sulprostone and misoprostol were used as alternative uterotonics because oxytocin is considered potentially arrhythmogenic and should be avoided or used with caution in patients with LQTS, particularly when administered as a rapid intravenous bolus [4,5].
Given the risk of VT, continuous intra-arterial blood pressure and electrolyte monitoring were maintained throughout surgery [1,4].
For patients with an ICD, special precautions are required [1,3,4]. However, after cardiology consultation, it was determined that the ICD could remain active since the surgical site was infraumbilical and diathermy was not required. Defibrillation pads were positioned as a precaution, and a cardiologist was present throughout the procedure.
Postoperative management of patients with LQTS should include permanence in a postsurgical intensive care unit for at least 24h-48h [4]. The QT interval should be monitored, and the ICD should have the original programming setting restored [3,4]. Other goals of postoperative care include adequate pain control and a quiet environment [1,3]. Multimodal analgesia was the option, with regional techniques and analgesics from various pharmacological classes.
Close follow-up in the early postpartum period is crucial [1,2,5]. Therefore, monitoring by a cardiologist within the first weeks postpartum and then monthly for the first nine months is recommended to evaluate treatment efficacy, ECG changes and symptom progression [5].
Conclusions
The uniqueness of this case lies not merely in the presence of LQT1, but in the convergence of multiple high-risk elements, including prior episodes of sustained VT, foetal conduction abnormalities and pronounced maternal anxiety, which collectively heightened perioperative risk. Regional anaesthesia was considered, but deemed inappropriate given the patient's severe anxiety and previous arrhythmic responses to stress. In the absence of established guidelines, this case underscores the importance of multidisciplinary collaboration and careful planning, with anaesthetic management tailored to the patient’s physiological and psychological profile to minimise arrhythmogenic risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Long QT syndrome management during and after pregnancy Medicina (Kaunas) Marcinkeviciene A Rinkuniene D Puodziukynas A 16945820223642223310.3390/medicina 58111694 PMC 9696301 · doi ↗ · pubmed ↗
- 2Arrhythmic risk during pregnancy and postpartum in patients with long QT syndrome Herzschrittmacherther Elektrophysiol Asatryan B Rieder M Castiglione A Odening KE 1801853220213378275410.1007/s 00399-021-00757-4PMC 8166676 · doi ↗ · pubmed ↗
- 3Perioperative management of patients with congenital or acquired disorders of the QT interval Br J Anaesth O'Hare M Maldonado Y Munro J Ackerman MJ Ramakrishna H Sorajja D 62964412020182957610510.1016/j.bja.2017.12.040 · doi ↗ · pubmed ↗
- 4Brief review: anesthetic implications of long QT syndrome in pregnancy Can J Anaesth Drake E Preston R Douglas J 5615725420071760204310.1007/BF 03022321 · doi ↗ · pubmed ↗
- 5Management of long QT syndrome in women before, during, and after pregnancy US Cardiol Taylor C Stambler BS 015202110.15420/usc.2021.02PMC 1166476239720507 · doi ↗ · pubmed ↗
- 6Drugs to be avoided in patients with long QT syndrome: focus on the anaesthesiological management World J Cardiol Fazio G Vernuccio F Grutta G Re GL 8793520132367555410.4330/wjc.v 5.i 4.87PMC 3653016 · doi ↗ · pubmed ↗
- 7Long QT syndrome: anaesthetic management at delivery Int J Obstet Anesth Behl S Wauchob TD 3473501420051614051710.1016/j.ijoa.2005.04.005 · doi ↗ · pubmed ↗
- 8Anaesthetic considerations in pregnant patients with cardiac arrhythmia BJA Educ Bhatia K D'Souza R MalhaméI Thorne S 1962062320233712416910.1016/j.bjae.2023.01.008PMC 10140473 · doi ↗ · pubmed ↗