Measurement of the Distance between the Mitral Annulus and the Left Circumflex Coronary Artery Using Multiplanar Reconstruction of Intraoperative Transoesophageal Echocardiography Images
Yuki Kuroda, Yoshiharu Soga, Takehiko Matsuo, Shinichi Tsumaru, Keisuke Hakamada, Yuki Wada, Yuta Kitagata, Ryo Imada, Akira Marui, Nobuhisa Ohno

TL;DR
This study uses imaging to measure the distance between the mitral annulus and a coronary artery during heart surgery, finding shorter distances in patients with a specific heart condition.
Contribution
The study introduces a less invasive method using multiplanar reconstruction of TEE images to assess anatomical distances related to mitral valve surgery.
Findings
The left circumflex coronary artery is closest to the mitral annulus at 70-90 degrees counterclockwise from the anteroposterior axis.
Patients with mitral annular disjunction had significantly shorter distances between the mitral annulus and the left circumflex coronary artery.
MPR of TEE images is a useful tool for identifying patients with a short mitral annulus-left circumflex coronary artery distance.
Abstract
We aimed to describe the anatomical distance between the mitral annulus and the left circumflex coronary artery (LCX) using multiplanar reconstruction (MPR) of transoesophageal echocardiography (TEE) images and to investigate its association with mitral annular disjunction (MAD). A single-centre retrospective cohort study included 54 patients who underwent mitral valve repair for mitral regurgitation between January 2020 and July 2021. We measured the distance between the mitral annulus and the LCX (ML distance) using MPR of intraoperative TEE images. As an exploratory analysis, we compared the ML distance between patients with MAD (group D: N = 11) and those without (group N: N = 43). The LCX was closest to the mitral annulus at 70-90 degrees counterclockwise from the anteroposterior axis. No cases of LCX injury were observed. MAD was most frequently observed at P1, and all patients…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
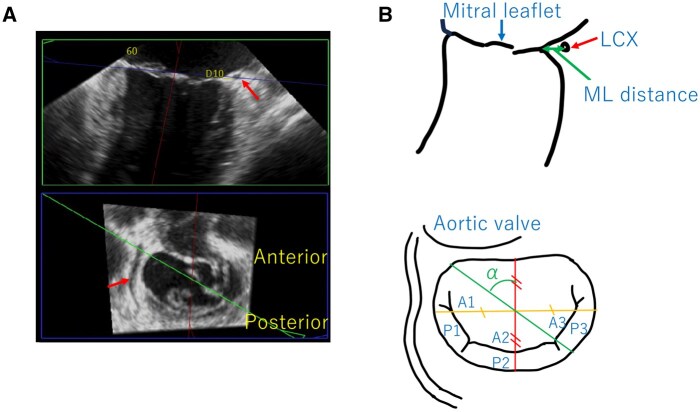 Figure 1
Figure 1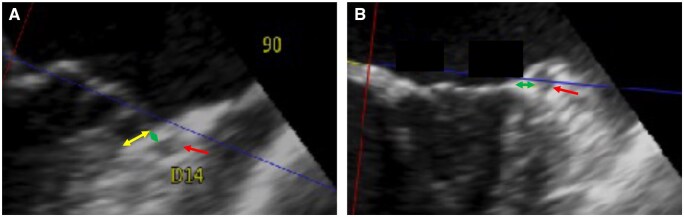 Figure 2
Figure 2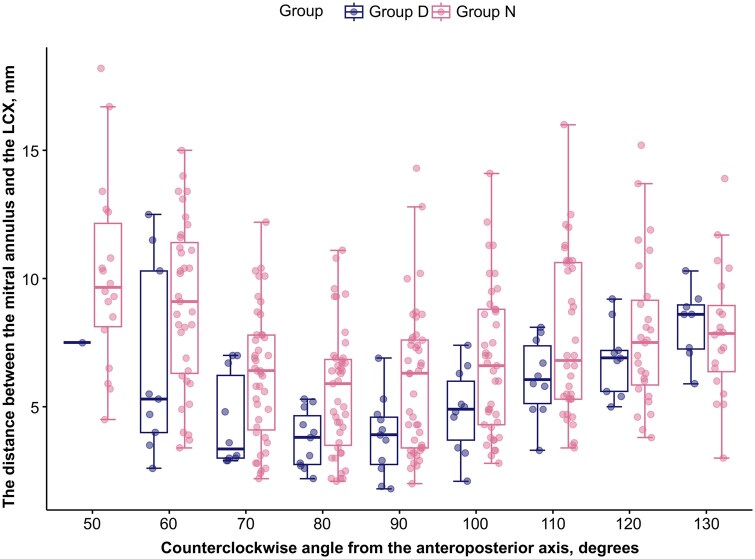 Figure 3
Figure 3| Characteristic | Overall | Group N | Group D |
|
|---|---|---|---|---|
|
|
|
| ||
| Age, years | 62.2 (13.7) | 61.9 (14.2) | 63.6 (12.0) | .71 |
| Male, | 40 (74%) | 32 (74%) | 8 (73%) | 1.00 |
| Body surface area, m2 | 1.7 (0.2) | 1.7 (0.2) | 1.7 (0.2) | .62 |
| Hypertension, | 33 (61%) | 27 (63%) | 6 (55%) | .73 |
| Diabetes mellitus | 6 (11%) | 6 (14%) | 0 (0%) | .33 |
| Dyslipidaemia, | 17 (31%) | 15 (35%) | 2 (18%) | .47 |
| Left ventricular end-diastolic diameter, mm | 52.9 (5.9) | 53.5 (5.9) | 50.3 (5.5) | .11 |
| Left ventricular end-systolic diameter, mm | 34.2 (4.3) | 34.6 (4.4) | 32.9 (4.1) | .26 |
| Left ventricular ejection fraction, % | 64.1 (4.5) | 64.3 (4.2) | 63.3 (5.6) | .51 |
| Surgical approach, | .50 | |||
| Median sternotomy | 31 (57%) | 26 (60%) | 5 (45%) | |
| Right thoracotomy | 23 (43%) | 17 (40%) | 6 (55%) | |
| Procedure, | ||||
| Resection | 40 (74%) | 32 (74%) | 8 (73%) | 1.00 |
| Neochordae | 22 (41%) | 16 (37%) | 6 (55%) | .32 |
| Edge to edge | 8 (15%) | 8 (19%) | 0 (0%) | .18 |
| Folding | 2 (3.7%) | 2 (4.7%) | 0 (0%) | 1.00 |
| Overall | Group N | Group D |
| |
|---|---|---|---|---|
|
|
|
| ||
| Anteroposterior diameter, mm | 33.2 (4.3) | 33.2 (4.2) | 33.1 (4.5) | .94 |
| Transverse diameter, mm | 36.3 (4.2) | 35.6 (3.9) | 39.2 (4.5) | .011 |
| Anteroposterior diameter (3D), mm | 34.3 (3.7) | 34.1 (3.8) | 34.8 (3.6) | .58 |
| Transverse diameter (3D), mm | 40.4 (4.4) | 39.7 (4.4) | 43.0 (3.4) | .025 |
| Perimeter, mm | 125.1 (11.8) | 123.9 (12.2) | 130.0 (9.5) | .13 |
| Anterolateral commissure, degrees | 65.0 [60.0, 70.0] | 65.0 [60.0, 70.0] | 65.0 [60.0, 70.0] | .63 |
| Cleft of P1-P2, degrees | 125.0 [120.0, 130.0] | 125.0 [120.0, 130.0] | 125.0 [120.0, 132.5] | .77 |
| Localization of MAD, | ||||
| P1 | 11 (100%) | 0 (NA%) | 11 (100%) | NA |
| P2 | 1 (9.1%) | 0 (NA%) | 1 (9.1%) | NA |
| P3 | 2 (18%) | 0 (NA%) | 2 (18%) | NA |
| Minimum ML distance | 4.5 (2.1) | 4.9 (2.1) | 3.2 (1.1) | .012 |
| Angles, degrees | Overall | Group N | Group D | Coefficient | 95% CI |
|
|---|---|---|---|---|---|---|
|
|
|
| ||||
| 50 | 10.0 (3.6) | 10.1 (3.6) | 7.5 (NA) | −2.61 | −9.92, 4.71 | .49 |
| 60 | 8.5 (3.4) | 9.0 (3.2) | 6.7 (3.7) | −2.37 | −4.81, 0.08 | .064 |
| 70 | 5.9 (2.5) | 6.2 (2.6) | 4.4 (1.8) | −1.84 | −3.52, −0.16 | .036 |
| 80 | 5.2 (2.3) | 5.6 (2.4) | 3.7 (1.1) | −1.87 | −3.35, −0.39 | .017 |
| 90 | 5.5 (2.7) | 5.9 (2.8) | 3.8 (1.5) | −2.10 | −3.84, −0.36 | .022 |
| 100 | 6.4 (2.7) | 6.7 (2.8) | 4.9 (1.6) | −1.89 | −3.74, −0.05 | .0497 |
| 110 | 7.4 (3.0) | 7.7 (3.2) | 6.1 (1.5) | −1.58 | −3.62, 0.46 | .14 |
| 120 | 7.6 (2.6) | 7.8 (2.9) | 6.9 (1.4) | −0.97 | −2.96, 1.03 | .35 |
| 130 | 8.0 (2.2) | 7.9 (2.5) | 8.2 (1.4) | 0.35 | −1.53, 2.22 | .72 |
| Angles, degrees | Balanced | Left dominant | Right dominant |
|
|---|---|---|---|---|
|
|
|
| ||
| 50 | 9.2 (1.7) | 7.7 (2.0) | 10.6 (3.9) | .47 |
| 60 | 6.0 (2.3) | 6.7 (2.8) | 9.0 (3.5) | .15 |
| 70 | 3.5 (2.0) | 4.2 (1.5) | 6.2 (2.5) | .047 |
| 80 | 2.7 (0.8) | 3.2 (1.2) | 5.6 (2.3) | .012 |
| 90 | 2.7 (0.6) | 3.5 (1.3) | 5.9 (2.7) | .029 |
| 100 | 4.0 (0.6) | 4.5 (0.8) | 6.8 (2.8) | .067 |
| 110 | 4.9 (0.4) | 5.5 (1.3) | 7.8 (3.0) | .085 |
| 120 | 6.1 (1.2) | 5.9 (1.6) | 8.0 (2.7) | .15 |
| 130 | 7.6 (0.4) | 6.8 (2.4) | 8.3 (2.3) | .38 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiac and Coronary Surgery Techniques · Congenital Heart Disease Studies
INTRODUCTION
One of the complications associated with mitral valve surgery is injury to the left circumflex coronary artery (LCX).1 The LCX is close to the mitral annulus in the vicinity of the anterolateral commissure and P1.2
Detection of the anatomical relationship between the LCX and the mitral annulus using three-dimensional computed tomography (3D CT) has been reported.3 We have been measuring the distance between the mitral annulus and the LCX (ML distance) using multiplanar reconstruction (MPR) of the intraoperative transoesophageal echocardiography (TEE) images, which we routinely perform during cardiovascular surgery. When the close proximity of the LCX to the mitral annulus is identified by TEE, the surgeons are alerted. During the process of evaluating the ML distance using TEE, we frequently observed that the ML distance was particularly short in patients with mitral annular disjunction (MAD).
MAD is a specific anatomical abnormality associated with mitral valve prolapse, characterized by a separation between the left atrium/mitral valve annulus and left ventricular myocardium.4^,^5 MAD was reported to be associated with annular contractile dysfunction and non-sustained ventricular tachycardia.6
We aimed to describe the anatomical distance between the mitral annulus and the LCX using MPR of TEE images and to investigate its association with MAD.
METHODS
Ethical statement
This single-centre retrospective cohort study was approved by the Institutional Review Board of Kokura Memorial Hospital (21100601; approval date: October 6, 2021). Because of the retrospective nature of the study, the requirement for written informed consent was waived. The collection and storage of biological materials and data in this study were conducted in accordance with the principles of the WMA Declaration of Taipei.
Study design
We measured the anatomical parameters of the mitral valve and the ML distance in 54 patients who underwent mitral valve repair for degenerative mitral regurgitation at Kokura Memorial Hospital between January 2020 and July 2021. Combined procedures such as aortic valve surgeries, tricuspid valve surgeries, and arrhythmia surgeries were included. We excluded cases where the mitral annulus was extremely large, and the LCX was outside the visible range of three-dimensional TEE. Furthermore, as an exploratory analysis, we compared the distance based on the presence or absence of MAD: patients with MAD (group D, N = 11, 20%) and patients without MAD (group N, N = 43, 80%). Patient characteristics and operative data were obtained from medical records. Baseline characteristics and anatomical parameters obtained from transthoracic and transoesophageal echocardiography were compared between the groups. Also, we compared the ML distance according to the coronary bed anatomy.
Measurement methods
Intraoperative TEE was performed routinely. We performed TEE using EPIC CVx (Philips, Amsterdam, The Netherlands). We confirmed the LCX in the mitral commissural view and captured the 3D images with the Full Volume mode. Captured images were post-processed using commercially available software (3DQ, Philips, Amsterdam, The Netherlands). We adjusted one of the MPR cross-sections to the height of the mitral valve attachment in the end-systolic phase, and adjusted the other two cross-sections so that they became cross-sections perpendicular to the previous cross-section and included the anteroposterior and transverse diameters of the mitral annulus. Using the intersection of the anteroposterior and transverse diameter cross-sections as the centre, we rotated the cross-section perpendicular to the mitral valve attachment cross-section and measured the ML distance. Measurements of the ML distance were taken in sections every 10 degrees (50-130 degrees) counterclockwise from the anteroposterior axis of the mitral valve (Figures 1 and 2). We defined MAD as >2 mm of separation between the left atrium/mitral valve annulus and left ventricular myocardium on the cross-section perpendicular to the mitral valve attachment cross-section. All measurements were performed by a single observer with over 10 years of experience in intraoperative TEE and measurements of the mitral valve.
MPR Images Obtained from TEE Images (A) and Their Schematic Diagram (B). (A) The upper image is a long-axis image of the lower image cut by the cross-section of the green line. Red arrows show the LCX. (B) The upper image is a long-axis image of the lower image cut by the cross-section of the green line. The ML distance is the distance between the mitral annulus and the LCX. α is the counterclockwise angle from the anteroposterior axis. MPR, multiplanar reconstruction; TEE, transoesophageal echocardiography; LCX, left circumflex coronary artery
Long Axis MPR Images at 90 Degrees Counterclockwise Angle from the Anteroposterior Axis in Patients with MAD (A) and Patients without MAD (B). The yellow arrow shows MAD. Red arrows show the LCX. Green arrows show the distance between the mitral annulus and the LCX. MPR, multiplanar reconstruction; MAD, mitral annular disjunction; LCX, left circumflex coronary artery
Statistical analysis
Categorical variables were presented as numbers (percentages) and were compared using Fisher’s exact test. Continuous variables were presented as mean (standard deviation) or median (interquartile range [IQR]) and were compared using the t-test, 1-way ANOVA, or the Wilcoxon rank-sum test. Effect sizes and 95% confidence intervals were estimated using the linear regression models. All statistical analyses were conducted using R statistical software version 4.4.1 (R Core Team (2024). R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/.). All reported P values were two-tailed, and P values less than .05 were considered statistically significant.
RESULTS
Patient characteristics
Baseline characteristics, including age, sex, body surface area (BSA), and underlying diseases, were not significantly different between the groups (Table 1). Left ventricular function was also not significantly different between the groups.
Anatomical parameters of the mitral valve by TEE
In the overall cohort, the anteroposterior and transverse diameters were 33.2 (4.3) mm and 36.3 (4.2) mm, respectively (Table 2). The anteroposterior diameter and perimeter of the mitral annulus were not different between group D and group N, while the transverse diameter was significantly larger in group D than in group N. The position of the anterolateral commissure was often near 65 degrees counterclockwise from the anteroposterior axis, and the position of the P1-P2 cleft was often near 125 degrees. These positions were similar between the groups. MAD was most frequently observed at P1, and all patients in group D had disjunction at P1.
The distance between the mitral annulus and the LCX
The LCX was closest to the mitral annulus at 70-90 degrees counterclockwise from the anteroposterior axis (5.9 [2.5] mm at 70 degrees, 5.2 [2.3] mm at 80 degrees, and 5.5 [2.7] mm at 90 degrees). In approximately 15% of the cases, the ML distance was less than 3 mm at 70-90 degrees (Table 3 and Figure 3). In the overall cohort, no cases of LCX injury were observed. The minimum value of ML distance in this series was 1.8 mm in one of the cases in group D.
The Distance between the Mitral Annulus and the LCX in Group D and Group N. LCX, left circumflex coronary artery
Overall, the ML distance was shorter in group D than in group N and was significantly shorter at 70-100 degrees (4.4 [1.8] mm versus 6.2 [2.6] mm, P = 0.036 at 70 degrees; 3.7 [1.1] mm versus 5.6 [2.4] mm, P = 0.017 at 80 degrees; 3.8 [1.5] mm versus 5.9 [2.8] mm, P = 0.022 at 90 degrees; and 4.9 [1.6] mm versus 6.7 [2.8] mm, P = 0.0497) (Table 3 and Figures 2 and 3). The minimum ML distance was significantly shorter in group D than in group N (3.2 [1.1] mm versus 4.9 [2.1] mm, P = 0.012) (Table 2).
Regarding the association between the ML distance and the coronary bed anatomy, the distance was significantly shorter in the balanced and left dominant groups compared to the right dominant group at 70-90 degrees (Table 4).
DISCUSSION
The main findings of this study were as follows: (1) Intraoperative TEE combined with software-based MPR images is less invasive and useful for studying the relationship between the mitral annulus and the LCX. (2) The LCX was closest to the mitral annulus at 70-90 degrees counterclockwise from the anteroposterior axis (at P1 near the anterolateral commissure). (3) The distance between the mitral annulus and the LCX was significantly shorter at 70-100 degrees in patients with MAD than in patients without MAD. We could avoid LCX injury during mitral valve surgery using MPR of intraoperative TEE for measurement of the ML distance and placing annuloplasty sutures with attention to the risk of LCX injury, though no comparative study was performed. Furthermore, few reports exist regarding the association of MAD with the proximity of the LCX to the mitral annulus. Our results from the exploratory analysis suggested the association between MAD and short ML distance, though further studies with a larger sample size would be needed to confirm this possibility.
LCX injury is a rare complication during mitral valve surgery, and the incidence has been reported to be as high as 1.8%.7 One of the reasons for this complication is that the LCX may run a course close to the mitral annulus. Various reports have appeared in the literature about the modalities for visualizing the relationship between the mitral annulus and the LCX. Ender et al reported the usefulness of intraoperative TEE in visualizing the LCX.8 It is reliable and routinely performed in cardiac surgery, though it is operator-dependent. Ghersin et al studied the three-dimensional relationship between the mitral annulus and the coronary arteries using cardiac CT scans.9 This modality was more reproducible and could visualize the LCX at a wider angle. However, contrast-enhanced CT cannot be performed for all patients for reasons such as chronic kidney disease and an allergy for contrast agents. We used the post-processed MPR images obtained from intraoperative TEE to study the relationship between the mitral annulus and the LCX. This method is more reproducible than TEE alone and can accurately identify the mitral annulus (leaflet attachment) and the LCX, as it can be played as a video.
Our data showed that the closest proximity area of the LCX to the mitral annulus was at a 70-90 degree counterclockwise angle from the anteroposterior axis, which corresponds to P1 near the anterolateral commissure. Our results are compatible with previous studies.2^,^9^,^10 Furthermore, we showed that the ML distance was shorter, especially in patients with MAD than in patients without MAD, and that this tendency is pronounced around 70-100 degrees in our model. Our results suggested the possibility of the anatomical association between the ML distance and MAD, though it was an exploratory analysis. Amongst patients with mitral valve prolapse, the prevalence of MAD has been reported to vary between 20% and 58%.11 We included only patients who underwent mitral valve repair for degenerative mitral regurgitation, and almost all of them had mitral valve prolapse. Therefore, the 20% prevalence of MAD in our cohort was consistent with the previous reports. It has been reported that MAD was located most frequently at P1 and P2, and less commonly at P3.12^,^13 Indeed, in our study, all patients with MAD had disjunction at P1. Although the reason for the association between MAD and short ML distance remains unclear, we believe there may be an embryological predisposition. Kishimoto et al3 also identified MAD and left coronary dominance as factors related to the proximity between the mitral annulus and LCX. In this study, left coronary dominance was also associated with proximity between the mitral annulus and LCX.
Though several possible mechanisms of LCX injury are possible: direct laceration of the vessel, complete encircling by a suture, and distortion due to tissue retraction,14 recognizing the ML distance seems to be helpful in order to avoid LCX injury. MPR of intraoperative TEE images would be helpful to identify patients with a short ML distance. No cases of LCX injury were observed in our study, and we could not identify the distance associated with a high risk of LCX injury. However, according to the previous reports, LCX injuries were observed in patients with an ML distance of 3-3.5 mm.15 In our study, approximately 15% of the patients had an ML distance less than 3 mm at 70-90 degrees. To prevent the LCX injury, it is important to place sutures towards the left ventricle and avoid deep sutures near P1 during annuloplasty, especially in patients with a short ML distance. Furthermore, when MAD or left coronary dominance is recognized preoperatively, surgeons can anticipate a high-risk anatomy for LCX injury and place sutures cautiously.
Our study has several limitations. First, the subgroup analysis according to the presence or absence of MAD was exploratory, and the small number of patients enrolled in this study limits our conclusion regarding the association between the ML distance and MAD. Also, observer bias may be present, as recognition of MAD could occur at the same time as measurement of the distance, though measurements were performed before investigating the association between MAD and short ML distance. Confirmation in a larger series with more robust imaging modalities, such as CT scans, would be needed. Second, measurement of the distance by TEE is limited in the systolic phase due to the limited range of the echo beam. According to the report by Ghersin et al, the distance between the mitral annulus and the LCX is similar between different phases of the cardiac cycle.9 Third, because measurements were performed by a single experienced observer, interobserver agreement could not be assessed. Also, while there appears to be no major deviation compared to previous reports,2^,^9 we would evaluate external validity in future studies. Fourth, measurements of the distance by TEE have a technical limitation. It is difficult to measure the distance in patients with an extremely large mitral annulus because the LCX falls outside the visible range of TEE.
CONCLUSIONS
MPR of intraoperative TEE images is a less invasive and useful tool to detect patients with a short ML distance. The area of the closest distance from the mitral annulus to the LCX is at P1 near the anterolateral commissure, especially in patients with MAD.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Grande AM , Fiore A, Massetti M, ViganòM. Iatrogenic circumflex coronary lesion in mitral valve surgery. Tex Heart Inst J. 2008;35:179-183.18612492 PMC 2435437 · pubmed ↗
- 2Miura K , Komiya T, Shimamoto T, Matsuo T. How far is the left circumflex coronary artery from the mitral annulus? Gen Thorac Cardiovasc Surg. 2020;68:1447-1452.33029760 10.1007/s 11748-020-01493-1 · doi ↗ · pubmed ↗
- 3Kishimoto N , Takahashi Y, Fujii H, et al Computed tomography to identify risk factors for left circumflex artery injury during mitral surgery. Eur J Cardiothorac Surg. 2022;61:675-683.34652422 10.1093/ejcts/ezab 409 · doi ↗ · pubmed ↗
- 4Van der Bijl P , Stassen J, Haugaa KH, et al Mitral annular disjunction in the context of mitral valve prolapse. JACC. 2024;17:1229-1245.38703174 10.1016/j.jcmg.2024.03.006 · doi ↗ · pubmed ↗
- 5Hutchins GM , Moore GW, Skoog DK. The association of floppy mitral valve with disjunction of the mitral annulus fibrosus. N Engl J Med. 1986;314:535-540.3945291 10.1056/NEJM 198602273140902 · doi ↗ · pubmed ↗
- 6Carmo P , Andrade MJ, Aguiar C, Rodrigues R, Gouveia R, Silva JA. Mitral annular disjunction in myxomatous mitral valve disease: a relevant abnormality recognizable by transthoracic echocardiography. Cardiovasc Ultrasound. 2010;8:53.21143934 10.1186/1476-7120-8-53PMC 3014886 · doi ↗ · pubmed ↗
- 7Aybek T , Risteski P, Miskovic A, et al Seven years’ experience with suture annuloplasty for mitral valve repair. J Thorac Cardiovasc Surg. 2006;131:99-106.16399300 10.1016/j.jtcvs.2005.07.060 · doi ↗ · pubmed ↗
- 8Ender J , Selbach M, Borger MA, et al Echocardiographic identification of iatrogenic injury of the circumflex artery during minimally invasive mitral valve repair. Ann Thorac Surg. 2010;89:1866-1872.20494041 10.1016/j.athoracsur.2010.02.059 · doi ↗ · pubmed ↗