Non-autoimmune Familial Hyperthyroidism in Children: The Importance of Genetic Testing
Mariana Sa Pinto, Tomás Ferrão, Andreia Dias Preda, Margarida Moreno Fernandes, Maria Adriana Rangel

TL;DR
A 16-year-old with non-autoimmune hyperthyroidism and family history was found to have a TSHR gene variant, showing the importance of genetic testing in such cases.
Contribution
Highlights the role of genetic testing in diagnosing non-autoimmune familial hyperthyroidism in children.
Findings
A TSHR gene variant c.2009A>G p.(Asn670Ser) was identified in a patient with non-autoimmune hyperthyroidism.
The patient's condition improved with methimazole treatment and clinical monitoring.
The case emphasizes the need to consider genetic causes in hyperthyroidism without autoimmune markers.
Abstract
Hyperthyroidism of non-autoimmune etiology is an uncommon occurrence, and its etiology may be the result of germline variants capable of activating the thyroid-stimulating hormone receptor (TSHR). The case of a 16-year-old adolescent with a family history of hyperthyroidism and negative antithyroid antibodies is presented. Imaging revealed bilateral subcentimeter nodules, and thyroid scintigraphy showed normal, heterogeneous uptake, with no hyperfunctioning areas. Genetic testing identified the likely pathogenic variant c.2009A>G p.(Asn670Ser) in the TSHR gene, which has been previously described in families with non-autoimmune hyperthyroidism. The patient is undergoing treatment with methimazole, with normalization of thyroid function and clinical surveillance. This case highlights the need to consider alternative etiologies of hyperthyroidism, particularly in the absence of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
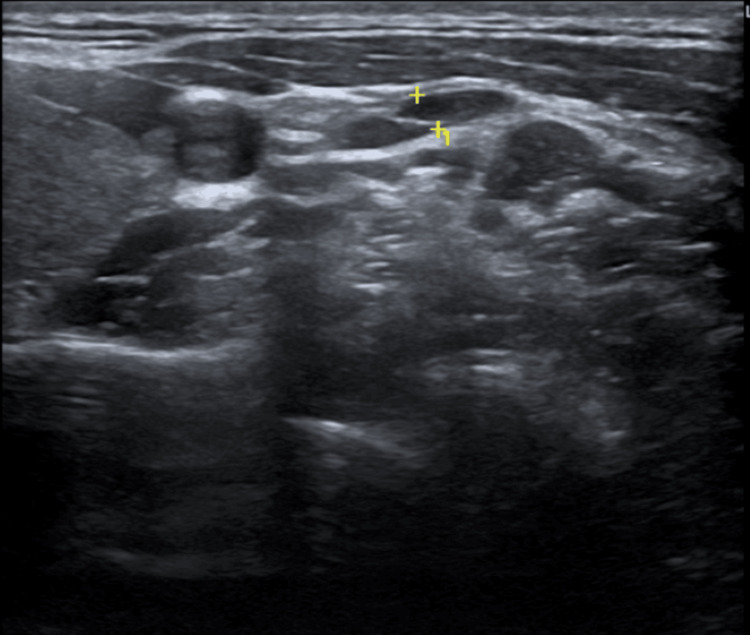 Figure 1
Figure 1| Laboratory parameter | Patient value | Reference range | Units |
| TSH | <0.005 | 0.4-4.0 | μIU/mL |
| Free T4 | 2.1 | 0.8-1.8 | ng/dL |
| TRAbs | Negative | Negative | - |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Disorders and Treatments · Ophthalmology and Eye Disorders · Diabetes and associated disorders
Introduction
The predominant etiology of hyperthyroidism in children is autoimmune disease, particularly Graves' disease, accounting for approximately 80%-95% of cases [1-3]; however, in rare instances, hyperthyroidism may have a genetic basis due to activating germline variants of the thyroid-stimulating hormone receptor (TSHR) gene. This form of hyperthyroidism lacks autoimmune features and is transmitted in an autosomal dominant pattern, resulting in familial clustering [1,2]. It is characterized by persistent thyrotoxicosis, negative TSHR antibodies (TRAbs), a positive family history, and may be associated with nodular hyperplasia [1,3-5]. Recognizing these hereditary forms is essential for accurate diagnosis in pediatric patients, as well as for individualized therapeutic planning and appropriate genetic counseling [1,3-5].
Case presentation
A 16-year-old male adolescent, without siblings, was referred to the pediatric endocrinology outpatient clinic due to palpitations and suspected hyperthyroidism. Family history was significant for hyperthyroidism in the father, paternal grandfather, and paternal uncle, all of whom had undergone thyroidectomy. The father’s disease course was difficult to control with antithyroid drugs, requiring frequent dose adjustments and intermittent use of a block-and-replace strategy.
The patient denied weight loss, gastrointestinal disturbances, insomnia, decline in school performance, or ocular symptoms, such as exophthalmos. Laboratory evaluation demonstrated persistently suppressed TSH levels, with elevated free thyroxine (free T4) and negative TRAbs. A detailed summary of laboratory findings is presented in Table 1.
Thyroid ultrasound revealed a mildly enlarged gland with bilateral nodules measuring up to 8 mm, classified as TI-RADS 3 and 4, without suspicious malignant features or significant interval growth (Figure 1). Thyroid scintigraphy demonstrated normal global uptake (2.4%), with no hyperfunctioning nodules.
Thyroid ultrasound imaging
Treatment with methimazole (0.15 mg/kg/day) was initiated, leading to progressive normalization of thyroid function. The patient is currently maintained on a low dose (2.5 mg/day), remains asymptomatic, and reports no adverse effects. Genetic testing identified a likely pathogenic heterozygous TSHR variant, c.2009A>G p.(Asn670Ser), previously associated with familial non-autoimmune hyperthyroidism and nodular hyperplasia. The father is awaiting genetic testing.
Discussion
This case illustrates persistent hyperthyroidism with negative thyroid autoantibodies and a positive family history, a clinical profile that is highly suggestive of familial non-autoimmune hyperthyroidism [1,2,5]. The p.Asn670Ser variant in the TSHR gene is a constitutively activating variant, previously associated with early-onset thyrotoxicosis and, in some cases, thyroid nodules [1,2,4]. Distinguishing this condition from Graves' disease is essential, as prognosis, risk of recurrence, and long-term management differ substantially [2,3,6]. Antithyroid drugs may achieve initial biochemical control; however, in genetically mediated hyperthyroidism, they are generally considered a temporizing measure rather than a curative option, with definitive therapies, such as radioactive iodine or thyroidectomy, often required [2,3,5].
This case highlights the importance of early recognition and thorough evaluation of family history, as well as the role of genetic testing in enabling timely diagnosis and preventive genetic counseling in affected families, particularly given the autosomal dominant pattern of transmission and the associated risk to relatives [1,3,5].
Conclusions
Familial non-autoimmune hyperthyroidism represents a rare but clinically significant cause of persistent thyrotoxicosis in pediatric patients, particularly in the presence of negative thyroid autoantibodies and a suggestive family history, where early identification of an activating germline TSHR variant enables accurate diagnosis, individualized therapeutic planning, and appropriate genetic counseling. Early genetic diagnosis also influences long-term management decisions, including the timing of definitive therapy. Identification of a pathogenic TSHR variant supports a family-centered approach, including cascade genetic screening of at-risk relatives, as a preventive strategy to optimize long-term follow-up and management.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Familial nonautoimmune hyperthyroidism caused by a germline TSHR pathogenic variant JCEM Case Rep Takahashi S Taniyama M Fukuda T Kobayashi T 02202410.1210/jcemcr/luae 167PMC 1140892939301178 · doi ↗ · pubmed ↗
- 2Familial non-autoimmune hyperthyroidism in four generations caused by a novel disease-causing variant in the TSHR gene Balkan J Med Genet Malej A Avbelj Stefanija M BrataničN Trebušak Podkrajšek K 87922320213381607710.2478/bjmg-2020-0022 PMC 8009563 · doi ↗ · pubmed ↗
- 3Hyperthyroidism in children Pediatr Rev Srinivasan S Misra M 2392483620152603425410.1542/pir.36-6-239 · doi ↗ · pubmed ↗
- 4Thyroid gene expression in familial nonautoimmune hyperthyroidism shows common characteristics with hyperfunctioning autonomous adenomas J Clin Endocrinol Metab Hébrant A Van Sande J Roger PP 260226099420091938378110.1210/jc.2008-2191 · doi ↗ · pubmed ↗
- 5Central TSH dysregulation in a patient with familial non-autoimmune autosomal dominant hyperthyroidism due to a novel thyroid-stimulating hormone receptor disease-causing variant Medicina (Kaunas) Suput Omladic J Pajek M Groselj U 3019657202110.3390/medicina 57030196 PMC 799654633669123 · doi ↗ · pubmed ↗
- 6Extrathyroidal manifestations of persistent sporadic non-autoimmune hyperthyroidism in a 6-year-old boy: a case report Life Ahn MB 713112021 https://doi.org/10.3390/life 110707133435708410.3390/life 11070713 PMC 8305946 · doi ↗ · pubmed ↗