Genital tuberculosis initially presenting as pyometra and progressing to miliary tuberculosis: A case report
Kentaro Kasuga, Miyako Kitazono, Masaomi Maeda, Taro Koba, Shuichi Matsuda, Mikio Takamori

TL;DR
A rare case of genital tuberculosis misdiagnosed as pyometra eventually led to miliary tuberculosis, highlighting the importance of considering tuberculosis in unusual infections.
Contribution
This case report highlights genital tuberculosis as a potential cause of pyometra and emphasizes the need for early diagnosis to prevent severe disease.
Findings
Genital tuberculosis can present as pyometra and progress to miliary tuberculosis if undiagnosed.
Tuberculosis should be considered in the differential diagnosis of pyometra, especially in immunosuppressed patients.
Anti-tuberculosis treatment successfully improved both pyometra and miliary tuberculosis in this case.
Abstract
Female genital tuberculosis is a rare and often asymptomatic condition, which makes its diagnosis challenging. Early recognition of uncommon clinical presentation of tuberculosis is crucial for the better management of it. We report herein a case of genital tuberculosis that initially presented as pyometra and subsequently progressed to miliary tuberculosis. An 86-year-old woman with a history of immunosuppressive therapy for bullous pemphigoid presented with fever and septic shock and was diagnosed with pyelonephritis. Computed tomography (CT) incidentally revealed pyometra, from which Escherichia coli was isolated, and showed no abnormal findings in the lung fields. At the time, an acid-fast bacillus and histopathological examination had not been conducted. Although she improved with antibiotics, her fever recurred one month later. Repeat CT demonstrated diffuse, granular opacities in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
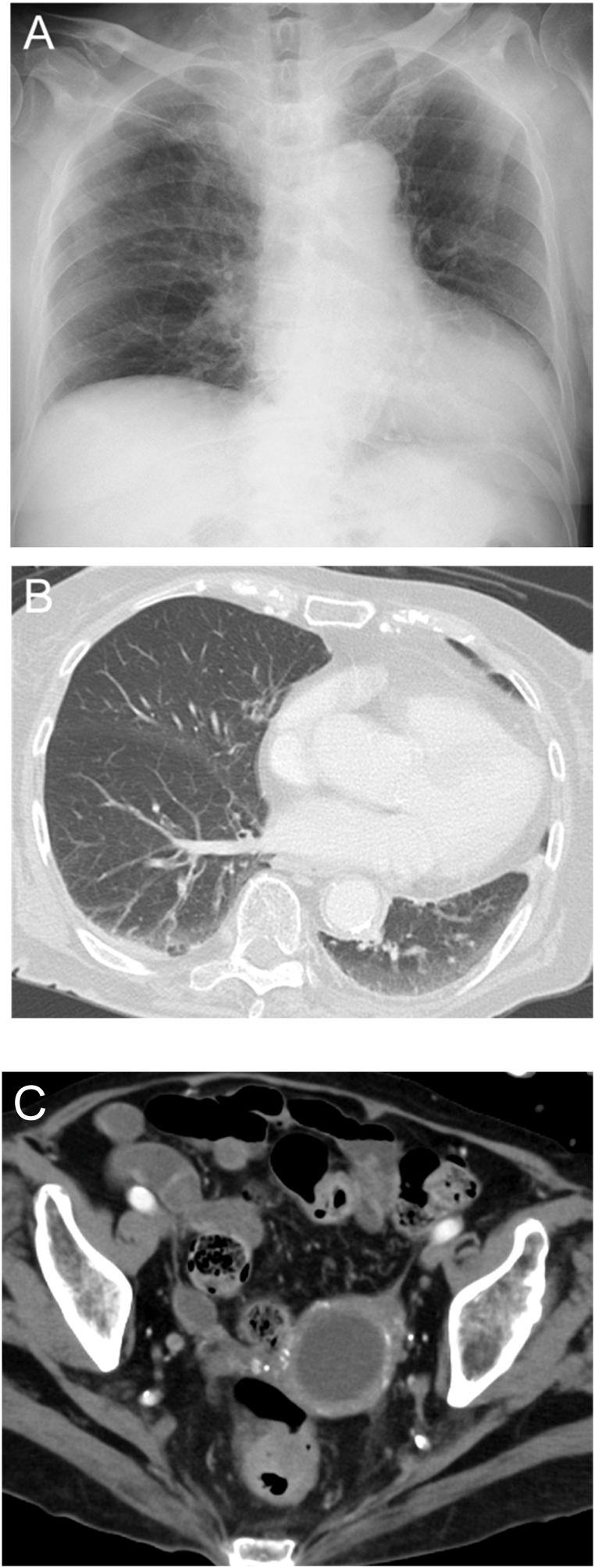 Figure 1
Figure 1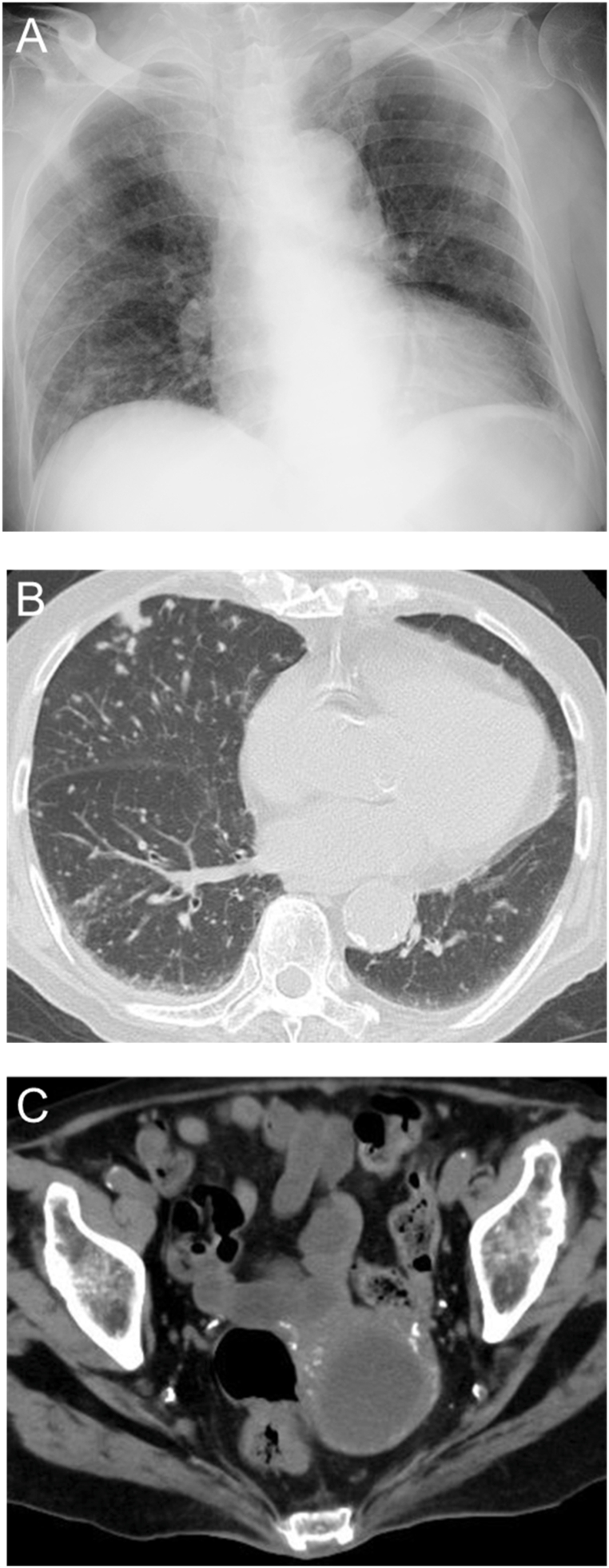 Figure 2
Figure 2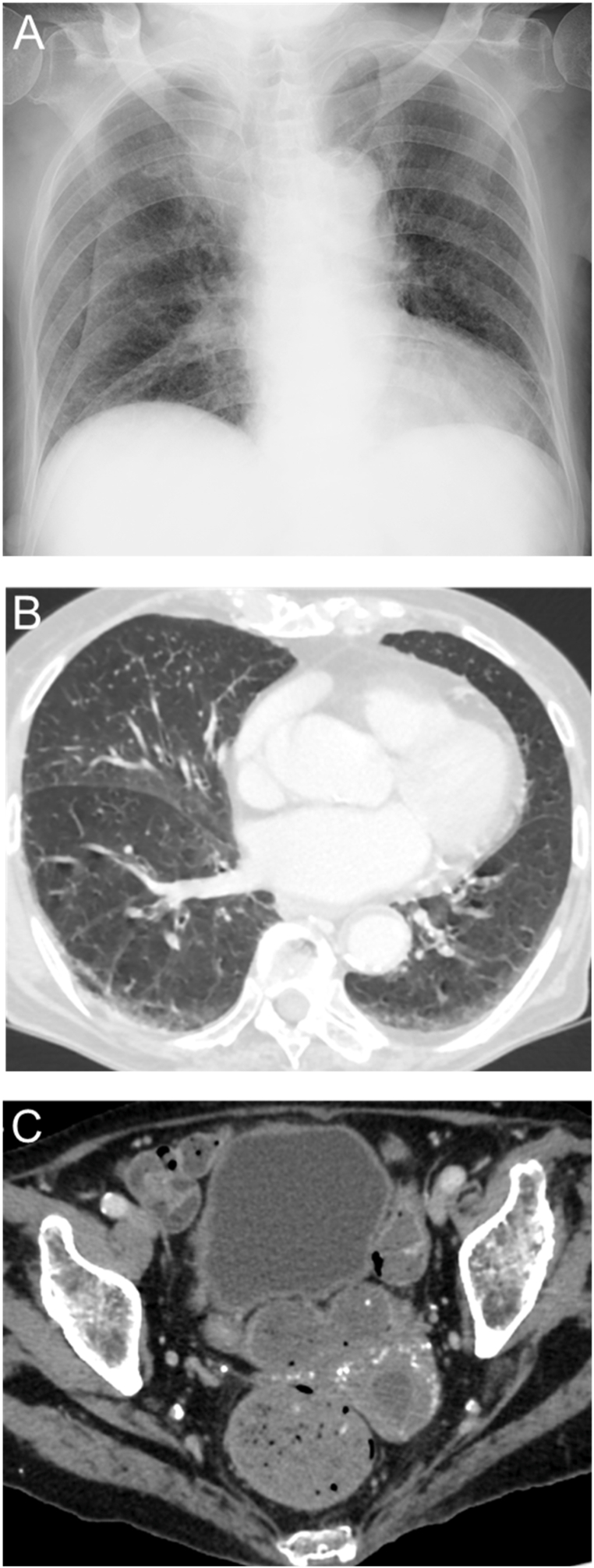 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDiagnosis and treatment of tuberculosis · Gynecological conditions and treatments · Infectious Diseases and Tuberculosis
Introduction
1
Genital tuberculosis is rare and often asymptomatic, and its diagnosis is challenging [[1], [2], [3], [4]]. Female genital tuberculosis reportedly occurs in 0.002–0.56 % of hospitalized women and in 0.2–21 % of infertile women, although the prevalence varies significantly by country and region due to differences in tuberculosis burden [3,[5], [6], [7], [8]]. The patients with genital tuberculosis have been reported to be approximately 0.1 % in all female patients with active tuberculosis in Japan, a low tuberculosis prevalence country [9]. In genital tuberculosis, M. tuberculosis is thought to be primarily transmitted hematogenously from the lungs to the fallopian tubes and endometrium during the primary infection [[10], [11], [12], [13]]. Most cases of genital tuberculosis are relapses stemming from a latent site years or even decades after the initial infection [4,13].
Pyometra occurs in 0.5–2.5 % of uterine tuberculosis cases [14]. The development of pyometra is attributed to impaired uterine clearance in elderly post-menopausal women with functional decline, and the symptoms are often non-specific [15]. Aerobic and anaerobic organisms account for almost all the causative pathogens in pyometra [15], while cases due to Mycobacterium tuberculosis (M. tuberculosis) are rare. Diagnosis of tuberculous pyometra requires microbiologic and histopathologic evaluation of specimens collected from endometrium, including nucleic acid amplification tests [16]. Low incidence rate and insidious disease progression reduce the opportunity of clinical suspicion and delay the diagnosis of tuberculous pyometra.
We report herein a case of genital tuberculosis that initially presented as pyometra, then progressed to miliary tuberculosis.
This case report has been reported in line with the 2025 SCARE criteria.
Case presentation
2
Four months before referred to our hospital, an 86-year-old woman with diabetes mellitus was diagnosed with bullous pemphigoid, began immunosuppressive therapy with prednisolone 20 mg/day, cyclosporine 50 mg/day, and intravenous immunoglobulin 20,000 mg/day (400 mg/kg/day). Three months later, she was admitted to a previous hospital with a fever and septic shock, with diagnosis of pyelonephritis. Computed tomography (CT) incidentally revealed pyometra, but no evident abnormalities in the lung fields (Fig. 1). Endometrial aspiration was performed, and Escherichia coli (E. coli) was isolated from a general bacterial culture of the uterine contents, while an acid-fast bacillus (AFB) culture was not obtained and a histopathological examination was not performed due to a negative cytology result. Ampicillin/sulbactam was administered, with cessation of cyclosporin. She recovered from septic shock by glucocorticoid replacement therapy considering relative adrenal insufficiency. However, one month later, her fever recurred. Chest X-ray and CT revealed diffuse, granular opacities in the bilateral lungs and an enlargement of the pyometra (Fig. 2). Although both the AFB smear and nucleic acid amplification test (NAAT) for M. tuberculosis were negative in the sputum, the uterine contents tested positive on both tests. She was transferred to our hospital for quarantine, further evaluation, and treatment.Fig. 1CT findings at one month before admission. A. Chest CT demonstrated no evident abnormalities in the lung fields. B. Abdominal and pelvic CT demonstrated the uterine pyometra.Fig. 1. Fig. 2CT findings on admission to our hospital. A. Chest CT demonstrated diffuse, bilateral, granular opacities. B. Abdominal and pelvic CT demonstrated an enlargement of the uterine pyometra.Fig. 2
She was diagnosed with progressive supranuclear palsy during the previous hospitalization, and was bedridden and fully dependent in all activities of daily living. Her medication included prednisolone 15 mg/day, trimethoprim 40 mg/day, sulfamethoxazole 200 mg/day, rabeprazole 10 mg/day, levodopa 300 mg/day, and carbidopa 30 mg/day on admission. She had no history of infertility (gravida 4, para 4) and no family history of tuberculosis. Physical examination revealed a Glasgow Coma Scale score of 14 (E4V4M6), body temperature of 37.2 °C, blood pressure of 102/80 mmHg, heart rate of 86 beats/min, and SpO_2_ of 94 % on room air. Chest and abdominal examinations were unremarkable. Blood tests revealed elevated white blood cell count and C-reactive protein level, and positive result in the T-SPOT test (Table 1). The AFB smears of the sputum and uterine contents were ± and 2+, respectively, and NAATs for M. tuberculosis were positive in both specimens. AFB cultures identified M. tuberculosis in the sputum and uterine contents, but not in the blood or urine. General bacterial culture of the uterine contents yielded E. coli and Klebsiella oxytoca (K. oxytoca). Cytological examination of the uterine contents revealed no malignant cells. She was diagnosed with genital tuberculosis and miliary tuberculosis. Anti-tuberculosis therapy was initiated with isoniazid 250 mg/day, rifampicin 450 mg/day, ethambutol 750 mg/day, and pyrazinamide 1100 mg/day. Drug susceptibility testing confirmed sensitivity to all anti-tuberculosis drugs.Table 1. Laboratory findings performed on admission to our hospital.Table 1. HematologyBiochemistry and serologyWhite blood cells8000/μLTotal protein6.1g/dL Neutrophils82%Albumin2.5g/dL Lymphocytes11%Total bilirubin1.1mg/dL Monocytes5%AST16IU/L Eosinophils1%ALT10IU/LHemoglobin9.1g/dLLDH232IU/LPlatelet21.7x10^4^ μLCreatine kinase18IU/LESR (1h)97mmBlood urea nitrogen13.7mg/dLCreatinine0.55mg/dLGlucose221mg/dLHemoglobin A1c7.5%C-reactive protein5.06mg/dLIGRA(T-SPOT®)positivePanel A35Panel B: 4646Nil Control0Positive Control501Abbreviations: ESR, erythrocyte sedimentation rate; AST, aspartate transaminase; ALT, alanine aminotransferase; LDH, lactate dehydrogenase; IGRA, Interferon-γ release assay.
One month after the initiation of this treatment, follow-up chest X-ray and CT demonstrated improvement in the bilateral, granular opacities and a significant reduction in the size of the pyometra (Fig. 3). After confirming that three consecutive sputum AFB smears were negative, she was transferred back to the previous hospital on the 35th day of hospitalization.Fig. 3CT findings at one month after anti-tuberculosis treatment. A. Chest CT demonstrated an improvement in the diffuse, bilateral, granular opacities. B. Abdominal and pelvic CT demonstrated a reduction in the size of the pyometra.Fig. 3
Discussion
3
This case report highlights the difficulty in diagnosing tuberculous pyometra. The progression to miliary tuberculosis provided the opportunity to diagnose the tuberculous pyometra, suggesting that delay in diagnosis of tuberculous pyometra has potential for deterioration. Previous reports of postmenopausal tuberculous pyometra showed favorable outcomes without progression to miliary tuberculosis [2,14,17,18], while our patient fortunately followed an uneventful course after stating anti-tuberculous treatment. Reactivation of tuberculosis in the elderly or immunocompromised hosts resulting from latent infection have become more common in low tuberculosis burden countries [19]. Although tuberculosis is a rare cause of pyometra, understanding atypical presentations of tuberculosis is vital for early detection, timely treatment, and infection control. Our case demonstrates that early suspicion of tuberculosis in the patient with pyometra warrants investigation for active infection through AFB and histopathological examination.
In our case, the patient was diagnosed with tuberculosis following immunosuppressive therapy for bullous pemphigoid and sepsis. Corticosteroid treatment has been associated with an increased risk of tuberculosis [20], and the prior use of other immunosuppressive agents may have contributed to the development of the disease. In addition, it has been reported that immunosuppression during sepsis and prolonged sepsis-induced immunoparalysis can occur, particularly in elderly individuals [21]. Based on these reports, uterine tuberculosis in this patient was most likely a reactivation of latent infection triggered by immunosuppression, resulting from both the initiation of immunosuppressive therapy and the onset of septic shock. We assume that miliary tuberculosis developed secondary to genital tuberculosis, as pyometra preceded the detection of abnormal findings in the lung fields. Previous reports have also described cases in which genital tuberculosis preceded miliary tuberculosis [22,23], supporting the possibility that genital tuberculosis in our patient progressed to miliary tuberculosis. E. coli and K. oxytoca were also isolated from the uterine contents, and co-infections involving M. tuberculosis and other bacteria are not uncommon [24,25]. Although such co-infection may have contributed to the formation of an abscess or localized tissue damage, in our case, the size of the pyometra decreased with anti-tuberculosis treatment alone, without additional antibacterial agents, which implies that the co-infection may not have played a major role.
Tuberculosis remains a major public health concern, particularly among elderly and immunocompromised individuals, who are at increased risk of both disease and death. In parts of the Western Pacific, where the aging population is growing rapidly, elderly individuals account for a large proportion of cases, and tuberculosis remains a leading cause of infectious morbidity and mortality [[26], [27], [28], [29]]. Given the global aging population and the increasing use of immunosuppressive therapies, it is quite possible that similar, clinical cases will be seen in the future. All medical professionals, including obstetricians and gynecologists, should consider M. tuberculosis a potential causative pathogen of pyometra and perform a thorough examination, including tests for genital tuberculosis, particularly in elderly or immunosuppressed patients, as well as in cases of antibiotic-resistant pyometra. Even if other bacteria are identified, as in our case, the possibility of M. tuberculosis should not be excluded.
All current reports of genital tuberculosis presenting as pyometra are descriptive studies, most of which are case reports of one or a few cases. Against this background, there is currently no established diagnosis or treatment protocol. Therefore, future analytical and observational studies on genital tuberculosis presenting as pyometra are warranted.
Conclusion
4
M. tuberculosis should be considered a potential causative pathogen of pyometra, particularly in elderly or immunosuppressed patients.
CRediT authorship contribution statement
Kentaro Kasuga: Writing – original draft, Data curation. Miyako Kitazono: Writing – review & editing. Masaomi Maeda: Writing – review & editing. Taro Koba: Writing – review & editing. Shuichi Matsuda: Writing – review & editing. Mikio Takamori: Writing – review & editing, Supervision.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Singh A.Yadav G.Gupta M.Sharma P.Kumari P.Elhence P.Tuberculosis and ovarian malignancy: sometimes mimics, sometimes coexists J. Obstet. Gynaecol. Res.46202094594910.1111/jog.1422332246574 · doi ↗ · pubmed ↗
- 2Balik G.Ustuner I.Ural U.M.Bayoglu Tekin Y.Kagitci M.Gucer H.Guvendag Guven E.S.Pelvic tuberculosis presenting with pyometra in a post-menopausal woman Ege J. Med.5320145355
- 3Figueiredo A.A.Lucon A.M.Srougi M.Urogenital tuberculosis Microbiol. Spectr.5201711610.1128/microbiolspec.tnmi 7-0015-2016 PMC 1168743528087922 · doi ↗ · pubmed ↗
- 4Muneer A.Macrae B.Krishnamoorthy S.Zumla A.Urogenital tuberculosis – epidemiology, pathogenesis and clinical features Nat. Rev. Urol.16201957359810.1038/s 41585-019-0228-931548730 · doi ↗ · pubmed ↗
- 5Sharma J.B.Sharma E.Sharma S.Singh D.Female genital tuberculosis: revisited Indian J. Med. Res.1482018 S 71S 8310.4103/ijmr.IJMR_648_1830964083 PMC 6469382 · doi ↗ · pubmed ↗
- 6Bicha M.M.Kebede T.Z.Arefeaynie A.L.Meressa E.W.Female genital tuberculosis presenting as a protruding anterior vaginal wall mass: a case report Front. Med.112025150296910.3389/fmed.2024.1502969 PMC 1179407939911663 · doi ↗ · pubmed ↗
- 7Kulchavenya E.Extrapulmonary tuberculosis: are statistical reports accurate?Ther. Adv. Infect. Dis.22014617010.1177/204993611452817325165556 PMC 4072044 · doi ↗ · pubmed ↗
- 8Neonakis I.K.Spandidos D.A.Petinaki E.Female genital tuberculosis: a review Scand. J. Infect. Dis.43201156457210.3109/00365548.2011.56852321438789 · doi ↗ · pubmed ↗