Psoriasis flare confused with drug allergy: A collaborative effort is required to treat tuberculosis in the setting of severe psoriasis
Quratulain Kizilbash, Adriana Vasquez, Barbara Seaworth, Lynn Horvath

TL;DR
Treating tuberculosis in patients with severe psoriasis requires collaboration between specialists to avoid misdiagnosing psoriasis flares as drug allergies.
Contribution
The paper highlights the importance of a multidisciplinary approach to manage TB and psoriasis simultaneously.
Findings
Two patients experienced psoriasis flares mistaken for TB drug reactions after stopping immunosuppressive therapy.
A combined treatment plan using acitretin, cyclosporine, and TB medications successfully managed both conditions.
Collaboration between TB and dermatology teams improved clinical and bacteriologic outcomes.
Abstract
Psoriasis is a chronic autoimmune disorder. Severe psoriasis is treated with systemic immunosuppressive agents. Systemic immunosuppression increases the risk of tuberculosis (TB) disease. Sudden cessation of immunosuppression seems logical in a TB patient but can lead to psoriasis flares. And when a new rash occurs during TB therapy, drug reaction is usually suspected. This can result in untreated TB disease or intermittent therapy, thus increasing the risk for acquired drug resistance. We describe two patients who developed TB disease during immunosuppressive therapy for psoriasis. When the immunosuppressive therapy was stopped, due to TB disease, both patients experienced significant worsening of psoriasis. The skin changes were confused with drug reaction to TB medications. Significant treatment interruptions resulted. A single team of TB physicians and one dermatologist, worked in…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2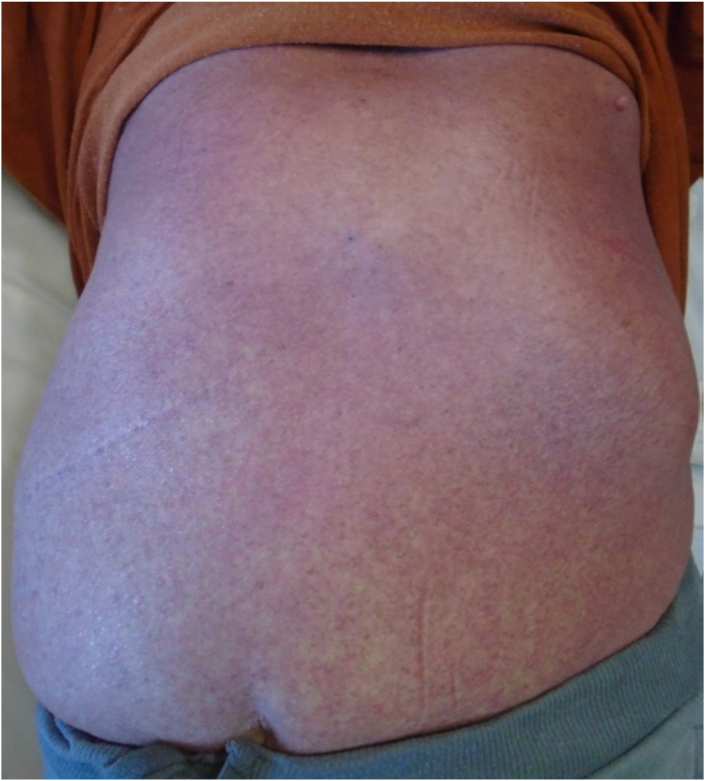 Figure 3
Figure 3 Figure 4
Figure 4 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPsoriasis: Treatment and Pathogenesis · Infectious Diseases and Tuberculosis · Tuberculosis Research and Epidemiology
Introduction
1
Psoriasis is a chronic autoimmune disorder that frequently affects the skin and joints. Psoriasis therapy has traditionally consisted of topical and systemic steroid therapy. However, psoriasis therapy has been revolutionized over the last two decades with development of tumor necrosis factor (TNF)–α–antagonist therapy. TNF–α–antagonist therapy results in dramatic improvement of psoriasis, but the immunosuppressive characteristics result in an increased risk of tuberculosis (TB) disease, as well as other infections [1]. Janus kinase (JAK) inhibitors result in a reduction of a variety of cytokines including TNF–α and are also used to treat a variety of immune mediated diseases including psoriasis [2]. Interleukin (IL) inhibitors including the IL-12/IL-23 inhibitor ustekinumab have emerged as safe and effective options for the treatment of psoriasis and although there is no clear evidence of increased risk of reactivation of TB, routine annual monitoring for TB is still recommended [3,4]. A review of the literature shows an abundance of articles published in the last decade on the topics of psoriasis and TB. However, most of these articles focus on identification and treatment of latent tuberculosis infection (LTBI) prior to initiation of TNF–α–antagonist therapy [[5], [6], [7]]. When TB disease is diagnosed, the recommendation by most experts is to discontinue biologic therapy for psoriasis and initiate TB therapy [8,9]. There is limited information on when to re-introduce TNF–α–antagonist therapy and JAK inhibitors [10].
We describe two patients with severe psoriasis that subsequently developed TB disease. Their treatment courses were complicated by suspected drug reactions, that were ultimately determined to be psoriasis flares. A team of physicians, including a team of infectious diseases physicians and a dermatologist, developed a treatment plan that first targeted the psoriasis and then the TB. Clear skin at the time of rechallenge of TB medications facilitated the provider's ability to identify subsequent drug reactions.
Case discussion
2
Patient #1
2.1
Patient is a 42-year-old Asian female with a 13-year history of severe psoriasis complicated by psoriatic arthritis. Her psoriasis had been treated with numerous therapies in the past, including topical agents, phototherapy, acitretin, prednisone, methotrexate, cyclosporine, ustekinumab, adalimumab, etanercept, and infliximab. She was diagnosed with cavitary pulmonary TB disease. At that time, her psoriasis was being successfully treated with etanercept. The patient was started on TB treatment with rifampin, moxifloxacin, pyrazinamide and ethambutol. Isoniazid was not prescribed initially due to concern of possible resistance due to prior isoniazid therapy for 6 months for LTBI. Etanercept was discontinued at the time of TB diagnosis. She was told that she should receive no systemic psoriasis therapy while being treated for TB. Two weeks after starting TB treatment she developed a diffuse rash requiring hospitalization. The rash was thought to be secondary to a TB drug reaction and all TB therapy was stopped. Over the next 6 months she underwent 7 outpatient attempts to restart TB therapy. All resulted in “new” rashes, thought to be drug reactions and led to treatment interruptions. Rifampin and rifabutin were reported as causing the most severe reactions. She was admitted to Texas Center for Infectious Disease (TCID) to be challenged with TB medications in a controlled, hospital setting. Patient had diffuse erythroderma and thick scale at the time of TCID admission (Fig. 1, Fig. 2). It was questioned how any physician could differentiate psoriasis from a drug reaction clinically in this patient. Dermatology evaluated the patient and suggested short term aggressive psoriasis therapy before initiation of TB therapy with acitretin and cyclosporine in conjunction with topical triamcinolone 0.1 % ointment nightly with a sauna suit. Patient's skin dramatically improved and cyclosporine was discontinued two weeks after its initiation. Psoriasis treatment was continued with acitretin, triamcinolone ointment and the sauna suit. TB was treated with sequential introduction of INH, moxifloxacin and linezolid. She then was challenged with rifampin, and she tolerated all drugs without development of rash. Ultimately, she was transitioned to INH and Rifampin therapy and successfully finished a 9-month course of TB therapy.Fig. 1. Back with diffuse erythroderma and thick scaleFig. 1Fig. 2Extremities with diffuse erythroderma and thick scale
Patient #2
2.2
Patient is a 71-year-old Caucasian male with a 40-year history of psoriasis and diabetes. Treatment for psoriasis included use of tanning beds and ustekinumab which was given 6 months and then again 2 months prior to his presentation to a rheumatologist with fatigue and musculoskeletal discomfort. The psoriasis was well controlled at that time. A screening Chest Xray and subsequent CT chest revealed right hilar lymphadenopathy. He was diagnosed with small cell lung cancer on a right hilar lymph node biopsy and pan-susceptible Mycobacterium tuberculosis grew from the same specimen 6 weeks later. He was diagnosed with disseminated TB involving the lungs, liver and spleen and was started on treatment with rifampin, isoniazid, pyrazinamide, and ethambutol and one week later started on chemotherapy for lung cancer with carboplatin and etoposide along with radiation. Two weeks after the initiation of TB therapy, he developed a diffuse, exfoliating rash requiring hospitalization. Drug reaction was considered, but skin biopsy was consistent with a psoriasis flare. One month after re-starting TB therapy, he developed transaminitis (AST 238 and ALT 249), requiring discontinuation of TB therapy. Treatment was changed to a liver friendly regimen with rifabutin, ethambutol and levofloxacin. Due to skin and liver issues, he had numerous treatment interruptions, and had only received 6 weeks of effective TB therapy over a period of 4 months. He was admitted to TCID to be challenged with TB medications in a controlled, hospital setting. Dermatology evaluated the patient and determined he had erythrodermic psoriasis (Fig. 3, Fig. 4, Fig. 5) and recommended systemic psoriasis therapy with acitretin 25mg daily and cyclosporine 100mg three times a day. The patient's pruritus and erythroderma significantly improved. Treatment for TB disease was started 4 days after initiation of psoriasis therapy with an escalating rifabutin dose for two days and then levofloxacin. Patient tolerated these medications well and was discharged on daily levofloxacin and rifabutin for a total of 9 months, to be given by directly observed therapy as an outpatient. Cyclosporine was discontinued two weeks after its initiation. Psoriasis treatment was continued with acitretin, triamcinolone 0.1 % ointment and use of a sauna suit and he was to follow up with dermatology one month after discharge from TCID. He completed radiation and 4 cycles of chemotherapy for lung cancer and was to follow up with oncology for a PET scan and further management.Fig. 3. Erythroderma of the backFig. 4Erythroderma and scaling of the palmsFig. 5Erythroderma and scaling of the feet with pitting and discoloration of toenails
Two patients were referred to TCID for admission and treatment of TB disease in the setting of severe psoriasis. Both patients were previously unable to tolerate TB therapy due to presumed drug reactions. We utilized a collaborative approach to care with a team of infectious disease physicians and a dermatologist. In both patients, we first aggressively treated the psoriasis. Our goal was to improve the psoriasis before re-challenge with TB medications. In both cases we used a combination of a short term (2 weeks) immunosuppressive agent, cyclosporine, and long-term use of a non-immunosuppressive agent, acitretin, with topical steroid therapy. Both patients demonstrated dramatically improved skin. The patients were then, sequentially challenged with TB medications at TCID while being closely monitored. Both tolerated TB therapy without any skin reaction, their TB disease improved clinically, bacteriologically, and radiographically and they were subsequently discharged to outpatient TB treatment.
Severe psoriasis is often treated with immunosuppressive agents. The diagnosis of TB disease frequently leads to sudden discontinuation of psoriasis therapy. However, an abrupt discontinuation of psoriasis therapy will likely result in a flare of the psoriasis as an immune reconstitution inflammatory syndrome (IRIS) type reaction. Both patients had clear skin prior to the initiation of TB treatment, and they subsequently had a psoriasis flare which was confused with a TB drug reaction. We would recommend continuation of psoriasis treatment if their disease is well controlled. Even in a seriously ill patient with well controlled psoriasis on a TNF–α–antagonist, the best option may be to continue it and start aggressive and adequate TB therapy. If the psoriasis is not controlled at the time of TB diagnosis this may need to be done first if the patient can tolerate waiting several weeks prior to the initiation of TB treatment. If TB treatment is delayed it would be recommended to continue airborne isolation during this time. A collaborative approach, including a TB clinician and a dermatologist, can provide balanced treatment of both TB disease and psoriasis which will allow for TB therapy without interruptions, prevent the development of drug resistance and improve patient satisfaction.
CRediT authorship contribution statement
Quratulain Kizilbash: Writing – original draft, Conceptualization. Adriana Vasquez: Writing – review & editing. Barbara Seaworth: Writing – review & editing, Conceptualization. Lynn Horvath: Writing – review & editing.
Informed consent
Patients were discharged from the hospital years ago and therefore written consent cannot be obtained at this time however verbal informed consent was provided and poster was presented previously at National TB research meeting without objections from the patients. No patient identifying information has been used for this manuscript.
Funding sources
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cantini F.Nannini C.Niccoli L.Iannone F.Delogu G.Garlaschi G.Sanduzzi A.Matucci A.Prignano F.Conversano M.Goletti D.SAFEBIO (Italian multidisciplinary task force for screening of tuberculosis before and during biologic therapy). Guidance for the management of patients with latent tuberculosis infection requiring biologic therapy in rheumatology and dermatology clinical practice Autoimmun. Rev.1462015 Jun 50350910.1016/j.autrev.2015.01.011Epub 2015 Jan 21. PMID: 2561781625617816 · doi ↗ · pubmed ↗
- 2Miot H.A.Criado P.R.de Castro C.C.S.Ianhez M.Talhari C.Ramos P.M.JAK-STAT pathway inhibitors in dermatology An. Bras. Dermatol.9852023 Sep-Oct 65667710.1016/j.abd.2023.03.001Epub 2023 May 23. PMID: 37230920; PMCID: PMC 1040456137230920 PMC 10404561 · doi ↗ · pubmed ↗
- 3Yang K.Oak A.S.W.Elewski B.E.Use of IL-23 inhibitors for the treatment of plaque psoriasis and psoriatic arthritis: a comprehensive review Am. J. Clin. Dermatol.2222021 Mar 17319210.1007/s 40257-020-00578-0PMID: 33301128; PMCID: PMC 772745433301128 PMC 7727454 · doi ↗ · pubmed ↗
- 4Menter A.Strober B.E.Kaplan D.H.Kivelevitch D.Prater E.F.Stoff B.Armstrong A.W.Connor C.Cordoro K.M.Davis D.M.R.Elewski B.E.Gelfand J.M.Gordon K.B.Gottlieb A.B.Kavanaugh A.Kiselica M.Korman N.J.Kroshinsky D.Lebwohl M.Leonardi C.L.Lichten J.Lim H.W.Mehta N.N.Paller A.S.Parra S.L.Pathy A.L.Rupani R.N.Siegel M.Wong E.B.Wu J.J.Hariharan V.Elmets C.A.Joint AAD-NPF guidelines of care for the management and treatment of psoriasis with biologics J. Am. Acad. Dermatol.8042019 Apr 1029107210.1016/j.jaad.2018.11.057Epub 2019 Feb 13. PMID: · doi ↗ · pubmed ↗
- 5Haley C.A.Treatment of latent tuberculosis infection Microbiol. Spectr.522017 Apr 10.1128/microbiolspec.tnmi 7-0039-2016 PMID: 28409555; PMCID: PMC 11687480 PMC 1168748028409555 · doi ↗ · pubmed ↗
- 6Bassukas I.D.Gaitanis G.Constantopoulos S.H.Diagnosis of tuberculosis in patients with psoriasis: the need for a modified approach Eur. Respir. J.3812011 Jul 23123210.1183/09031936.00016611 PMID: 21719504; author reply 232-321719504 · doi ↗ · pubmed ↗
- 7Katsenos S.Nikolopoulou M.Tsiouri G.Bassukas I.D.Constantopoulos S.H.The challenging evaluation of patients with severe psoriasis for latent tuberculosis: an important indication for IGRA Open Respir. Med. J.52011596010.2174/1874306401105010059 Epub 2011 Jun 24. PMID: 21754976; PMCID: PMC 313286521754976 PMC 3132865 · doi ↗ · pubmed ↗
- 8Cantini F.Prignano F.Goletti D.Restarting biologics and management of patients with flares of inflammatory rheumatic disorders or psoriasis during active tuberculosis treatment J. Rheumatol. Suppl.912014 May 788210.3899/jrheum.140106 PMID: 2478900424789004 · doi ↗ · pubmed ↗