Infection and risk of psoriasis and atopic dermatitis: A systematic review and meta-analysis
Zhiru Zhou, Xu Yao, Juan Su, Minxue Shen, Hervé Bachelez, Xiang Chen, Yi Xiao

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
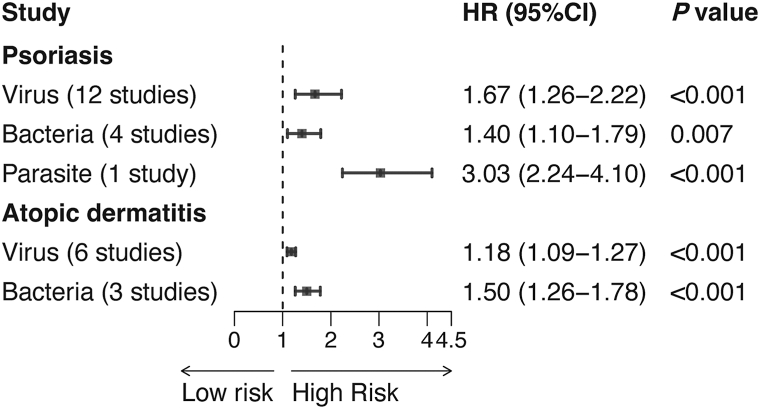 Figure 1
Figure 1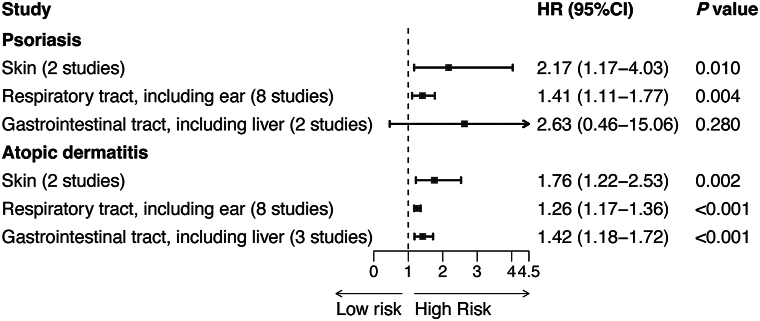 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDermatology and Skin Diseases · Psoriasis: Treatment and Pathogenesis · Dermatological diseases and infestations
To the Editor: Psoriasis and atopic dermatitis (AD) are common inflammatory diseases, characterized by chronic course and no known cure, highlighting the need to identify underlying etiology.1 Streptococcal pharyngitis is a well-established trigger of guttate psoriasis, and Staphylococcus aureus colonization contributes to AD progression.2^,^3 Moreover, the SARS-CoV-2 pandemic highlighted previously overlooked infectious triggers of immune dysregulation potentially linked to dermatological diseases.4 However, the impact of broader infections on the incidence of these diseases remains inconclusive. Therefore, we conducted a systematic review and meta-analysis to assess the relationship between infections and psoriasis or AD incidence.
Our review was registered in PROSPERO (CRD42023478691) following PRISMA and MOOSE guidelines (Supplementary Tables I and II, Appendix 1, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1). We searched PubMed, Web of Science, and Embase from inception to September 2025 for cohort studies examining infections and disease onset. Subgroup analysis stratified infections by type and site, while sensitivity analysis included studies using Cox proportional hazards model.
A total of 29 cohort studies (17 on psoriasis, 12 on AD) were included, encompassing 31,766,971 participants (Supplementary Fig 1, Table III, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1). Included studies were generally of high quality based on the Newcastle-Ottawa scale (Supplementary Table IV, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1). Infection was associated with a 64% increased risk of psoriasis (HR = 1.64, 95% CI: 1.32-2.04, P < .001), and a 23% increased risk of AD (HR = 1.23, 95% CI: 1.17-1.31, P < .001) (Supplementary Figs 2 and 3, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1). Subgroup analysis by infection type (Fig 1, Supplementary Figs 4 and 5, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1) revealed that viral (HR = 1.67), bacterial (HR = 1.40), and parasitic infection (HR = 3.03) were associated with psoriasis, while viral (HR = 1.18) and bacterial infection (HR = 1.50) were linked to AD. For infection site (Fig 2, Supplementary Figs 6 and 7, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1), psoriasis risk was elevated with skin (HR = 2.17) and respiratory tract infection (HR = 1.41), while AD incidence was linked to skin (HR = 1.76), respiratory tract (HR = 1.26), and gastrointestinal tract infection (HR = 1.42). Sensitivity analysis confirmed stable results (Supplementary Figs 8 and 9, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1), and the Egger test showed no evidence of publication bias.Fig 1. Psoriasis and atopic dermatitis. Summary of different types of infection and the incidence of psoriasis and atopic dermatitis. Data are presented as pooled hazard ratios (HRs) with 95% confidence intervals, calculated using random-effects models. Odds ratios and risk ratios from original studies were converted to HRs. Heterogeneity was assessed using I^2^ statistics and Cochran's Q-test. Detailed forest plots are shown in Supplementary Figs 4 and 5, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1. CI, Confidence interval; HR, hazard ratio.Fig 2. Psoriasis and atopic dermatitis. Summary of different sites of infection and the incidence of psoriasis and atopic dermatitis. Data are presented as pooled hazard ratios (HRs) with 95% confidence intervals. Statistical methods are as described in Fig 1. Detailed forest plots are shown in Supplementary Figs 6 and 7, available via Mendeley at https://data.mendeley.com/datasets/b5fvbd9djz/1.
Several limitations should be noted. First, although a random-effects model was applied to address heterogeneity, substantial variability remained, which may be explained by differences in infection definitions, study periods, or unknown disease etiology. Moreover, the observational design cannot establish causality, warranting further studies including Mendelian randomization or cytological experiments to strengthen causal inference. Additionally, the absence of cohort data for fungal infections in either psoriasis or AD limits generalizability and calls for high-quality cohort studies.
Despite limitations, our study provides epidemiological evidence that infection history should be considered a risk factor for both diseases. Broad infections extending beyond specific pathogens may act as a hit for chronic inflammation and immune stress in disease progression.5 Current clinical guidelines fail to adequately address infection-related risks, indicating the need for more comprehensive risk stratification strategies. Clinically, for individuals at high risk or with family history of disease, assessing infection history, controlling infections promptly, and modulating excessive immune response are essential. In patients with psoriasis or AD, especially on biological therapy, close infection monitoring is crucial to prevent disease flares. Further research should explore mechanistic links between systemic infections and immune dysregulation for targeted prevention strategies.
Conflicts of interest
Xiao serves as Councilor of the International Psoriasis Council (IPC), member of the International Society of Atopic Dermatitis (ISAD), Associate Editor of the Journal of Investigative Dermatology (JID), and member of the Large Database Workgroup of the Journal of the American Academy of Dermatology (JAAD).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chen Y.Peng C.Zhu L.Atopic dermatitis and psoriasis: similarities and differences in metabolism and microbiome Clin Rev Allergy Immunol 66202429431510.1007/s 12016-024-08995-338954264 · doi ↗ · pubmed ↗
- 2Leung D.Y.Travers J.B.Giorno R.Evidence for a streptococcal superantigen-driven process in acute guttate psoriasis J Clin Invest 9619952106211210.1172/JCI 1182637593594 PMC 185858 · doi ↗ · pubmed ↗
- 3Demessant-Flavigny A.L.Connetable S.Kerob D.Moreau M.Aguilar L.Wollenberg A.Skin microbiome dysbiosis and the role of Staphylococcus aureus in atopic dermatitis in adults and children: a narrative review J Eur Acad Dermatol Venereol 37Suppl 5202331710.1111/jdv.1912537232427 · doi ↗ · pubmed ↗
- 4Syed U.Subramanian A.Wraith D.C.Incidence of immune-mediated inflammatory diseases following COVID-19: a matched cohort study in UK primary care BMC Med 21202336310.1186/s 12916-023-03049-537735654 PMC 10512476 · doi ↗ · pubmed ↗
- 5Hwee J.Tait C.Sung L.Kwong J.C.Sutradhar R.Pole J.D.A systematic review and meta-analysis of the association between childhood infections and the risk of childhood acute lymphoblastic leukaemia Br J Cancer 118201812713710.1038/bjc.2017.36029065105 PMC 5765221 · doi ↗ · pubmed ↗