Histological and Immunohistochemical Biomarkers for Wound Age Estimation in Human Skin: A Systematic Review
Anas E Ahmed, Wassal F Aljohani, Akram K Moafa, Faisal A Hattan, Yaser A Altalhi, Nawaf S Alsulamy, Zayad M Albalawi, Feras M Aldhubayi, Abdulwhab A Alatawi, Nawaf K Alqahtani

TL;DR
This paper reviews biomarkers in human skin that help estimate wound age, focusing on how different markers are useful at different healing stages.
Contribution
The study systematically identifies and categorizes histological and immunohistochemical markers for wound age estimation across post-traumatic intervals.
Findings
Very early wounds show markers like fibronectin, CD62p, and TNF-α within minutes to one hour.
Intermediate wounds (1-10 days) are marked by immune cell phenotyping and chemokines like CD14 and MCP-1.
Late wounds (7+ days) involve hypoxia and matrix remodeling indicators such as ORP150 and VEGF.
Abstract
Accurate estimation of wound age is a critical challenge in forensic pathology, particularly for determining wound vitality and the interval between injury and death. Conventional histology often lacks sensitivity in the early post-traumatic stages, prompting investigation into molecular and immunohistochemical biomarkers. This review synthesizes evidence on histological and immunohistochemical markers used for wound age estimation in human skin, with attention to their applicability across different post-traumatic intervals. Very early wounds, from minutes up to one hour, are best characterized by markers related to haemostasis, mast cell activation, and early cytokine release, including fibronectin, CD62p (P-selectin), factor VIII-related antigen, tumor necrosis factor-alpha (TNF-α), and tryptase. Early wound stages, spanning hours, show transient mast cell accumulation and cytokine…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
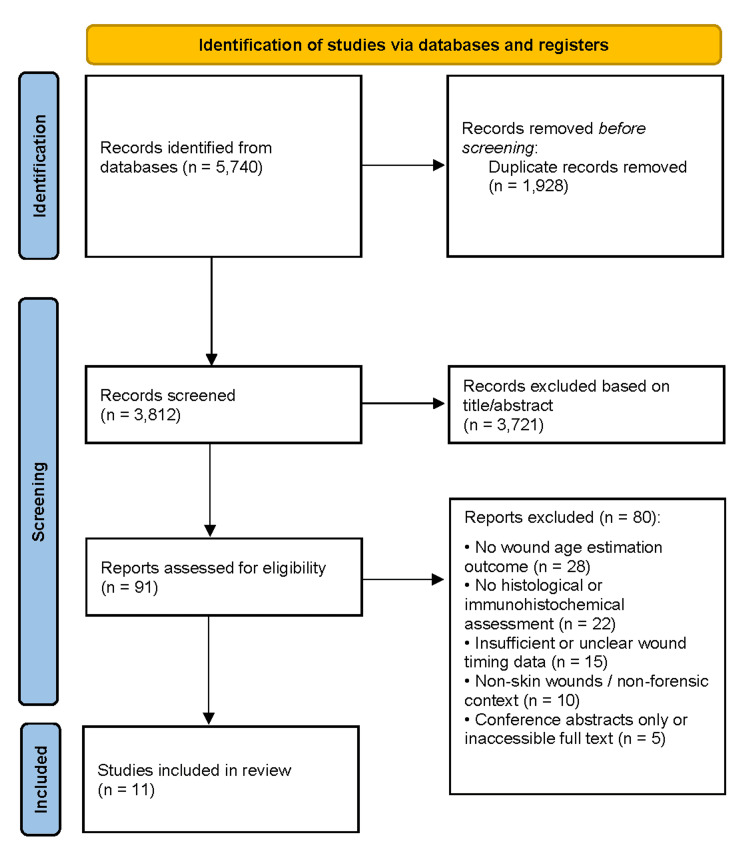 Figure 1
Figure 1| Study (author) | Study design and population | Sample size and wound type | Wound age range and groups | Marker(s) and category | Method and quantification | Time-dependent expression | Diagnostic performance | Forensic application | Key findings and limitations |
| van de Goot et al. [ | Human autopsy observational study | 807 samples; blunt-force; paired controls | Early wounds only; controls, few minutes, 15–30 min | Fibronectin, CD62p, Factor VIII | IHC; 4-grade scoring; probability model | ↑within minutes; peak 15–30 min; ↓not assessed | Probability: 0→non-vital 87–90%; 1–2→few min 72–93%; 3→15–30 min 55–76% | Very early wound age (minutes–30 min) | Coagulation markers allow early estimation; limitations: relies on reported wound timing |
| Bonelli et al. [ | Human autopsy study with surgical controls | 105 skin samples; 75 vital, 15 post-mortem, 15 surgical controls | ≤24 h; ≤1, 1–3, 3–6, 6–12, 12–24 h | Mast cells (tryptase/chymase) | Affinity cytochemistry + IHC; quantitative counts | ↑detectable ≤1 h; peak 1–3 h; ↓after 3 h | Statistically significant (p<0.01); no ROC | Early wound age (hours), vitality assessment | Transient dermal mast cell increase; limitation: group-based inference, no ROC metrics, reduced utility >24 h |
| Fronczek et al. [ | Human study, living subjects | 101 wound biopsies; mixed traumatic injuries | 0.2–25 d; 0.2–2, 2–4, 4–10, 10–25 d | MPO, CD45, CD68 (cells); IL-8, MIP-1 (chemokines); CML, vitronectin | IHC; cell counts, probability scoring | peak 0.2–2 d; ↓4–10 d; mild secondary ↑10–25 d | >10 IL-8/MIP-1 cells/mm²→<10 d; probability model; no ROC | Early–intermediate wound age (hours–days) | Combined markers improve estimation; limitations: living subjects, overlap, no ROC metrics |
| Fouad et al. [ | Human autopsy observational study | 40 autopsy cases; stab 55%, laceration 20%, incised 10%, abrasion 10%, contusion 5% | <12 h–10 d; <12 h, 12–24 h, 1–3 d, >3–10 d | CD14 (inflammatory cell surface receptor) | IHC (avidin–biotin); semi-quantitative % CD14+ cells | ↑<12 h; peak 1–3 d; ↓>3 d | ROC >90%: 1–3 d (Se/Sp 100%, AUC 1.0); 70% cut-off poor | Intermediate wound age (1–3 d), vitality assessment | Strong correlation with wound age; limitation: small sample in older wounds, limited wound types |
| Bacci et al. [ | Human autopsy study with surgical controls | 50 vital wounds, 10 post-mortem lesions, 10 surgical controls | ≤60 min; ≤5, 6–15, 16–30, 31–60 min | TNF-α–positive mast cells (cytokine) | Affinity cytochemistry + IHC; morphometric counts (cells/mm²) | ↑TNF-α >15 min; peak 31–60 min; ↓post-mortem lesions | Statistically significant differences; no sensitivity/specificity | Very early wound age (minutes–1 h), vitality assessment | TNF-α mast cells increase earlier than total mast cells; limitation: short time window, no diagnostic metrics |
| Ishida et al. [ | Human autopsy observational study | 58 wounds; paired controls | Few minutes–21 d; 0–12 h, 1–5, 7–14, 17–21 d | ORP150 (hypoxia/angiogenesis) | IHC; double-color fluorescence; morphometry | ↑≤12 h minimal; peak 7–14 d (~59%); ↓17–21 d (~28%) | Cut-off >50%→7–14 d; no ROC | Intermediate–late wound age (days–weeks) | Reflects hypoxia-driven granulation; limitations: overlap 1–5 and 17–21 d, semi-quantitative |
| Gauchotte et al. [ | Human autopsy/surgical study; ex vivo model | 12 stab wounds, 58 surgical, 8 controls, 24 early post-mortem | 1–44 min; <10, 10–20, >20–44 min | FVIIIra, CD15, mast cell tryptase | IHC on paraffin; quantitative/qualitative | Tryptase degranulation 1 min; CD15 9 min; peak first hour; ↓putrefied tissue | FVIIIra: Se 100%, Sp 47%; CD15: Se 47%, Sp 100%; tryptase: Se 60%, Sp 100% | Very early wound age (minutes), vitality | CD15 and tryptase are reliable early markers; limitations: putrefied tissue, moderate inter-observer agreement |
| Kondo et al. [ | Experimental animal study; human validation | 55 human wounds; paired controls | Few minutes–21 d; 0–12 h, 1–5, 7–14, 17–21 d | Ubiquitin (Ub, stress/heat-shock) | IHC; semi-quantitative morphometry; blinded observers | ↑4 h–1 d; peak 7–14 d (~31–45%); ↓17–21 d, shift to fibroblasts | <10%→<1 d; >10%→≥1 d; >20%→7–14 d; >30%→7–14 d; no ROC | Intermediate to late wound age | Clear cell-type pattern; limitations: overlap 1–5 and 17–21 d, semi-quantitative |
| Grellner et al. [ | Human autopsy/surgical study | 105 sharp-force wounds; paired controls | Minutes–6 weeks; early: 15–20, 30–60, 60–90 min | IL-1β, IL-6, TNF-α | IHC (APAAP); semi-quantitative | Earliest 15–20 min; peak 30–90 min; ↓several hours | Not reported | Very early wound age (minutes–hours), vitality | Rapid cytokine up-regulation precedes leukocytes; limitations: baseline expression, semi-quantitative |
| Grellner et al. [ | Human autopsy/surgical study | 74 wounds TGF-α, 51 TGF-β1; paired controls | Minutes–6 weeks; early 5 min–5 h | TGF-α, TGF-β1 (growth factors) | IHC (LSAB); semi-quantitative epidermis/dermis | TGF-α ↑~10 min; TGF-β1 minutes; peak 30–60 min; ↓TGF-α 1–1.5 h; TGF-β1 persists hours–weeks | Not reported | Very early to intermediate/late wound age | Rapid up-regulation precedes inflammation; limitations: baseline expression, semi-quantitative |
| Kondo et al. [ | Human autopsy observational study | 50 wounds; paired controls | Few minutes–21 d; 0–12 h, 1–4, 7–14, 17–21 d | IL-8, MCP-1, MIP-1α (chemokines) | IHC; semi-quantitative morphometry; two observers | ↑4–12 h; peak 1–4 d; ↓7–21 d, but higher than baseline | Cut-offs: IL-8 >50%, MCP-1 >30%, MIP-1α >40%→≥1 d; no ROC | Early–intermediate wound age (≥1 d) | Chemokine shift from neutrophils → macrophages/fibroblasts; limitations: baseline expression, overlap, semi-quantitative |
| Study (author) | Case selection | Index test | Reference standard | Flow and timing | Overall risk of bias |
| van de Goot et al. [ | Low: Large autopsy series (n=322) with clear grouping of controls, very early, and early vital wounds. | Low: IHC scoring system defined; consensus scoring by two assessors. | Low: Wound age based on forensic investigation and witness statements. | Unclear: Reliance on witness statements may introduce timing uncertainty. | Moderate |
| Bonelli et al. [ | Low: Clearly defined groups including vital lesions with documented survival times, post-mortem lesions, and healthy surgical controls; no inappropriate exclusions. | Unclear: Affinity cytochemistry and immunofluorescence methods for mast cells are described, but blinding and pre-specified diagnostic cut-offs are not reported. | Low: Wound age established independently from medical, police, and circumstantial records. | Low: All samples processed uniformly, PMI reported, all predefined groups included. | Moderate |
| Fronczek et al. [ | Low: Living subjects with known wound age prospectively included; exclusions justified; wound ages documented by victims and forensic physicians. | Low: IHC protocols, antibodies, scoring, and statistical modelling pre-specified; standardized assessment across markers. | Low: Wound age determined independently from patient history and forensic documentation. | Low: Biopsies processed uniformly; wound-age groups predefined; all cases analyzed. | Low |
| Fouad et al. [ | Low: Randomly selected autopsy cases with clearly defined inclusion/exclusion criteria; wounds of known infliction time included; paired non-injured skin controls. | Low: IHC staining, antibody details, semi-quantitative assessment, and ROC-based cut-offs are clearly described, reducing interpretation bias. | Low: Wound age independently established from police reports and documented infliction times. | Low: Samples processed uniformly; putrefied cases excluded; PMI ≤3 days; all cases analyzed. | Low |
| Bacci et al. [ | Low: Vital wounds, post-mortem lesions, and healthy skin controls are clearly defined; selected based on documented survival times with no inappropriate exclusions. | Unclear: IHC methods and quantification of TNF-α-positive mast cells are described, but blinding and pre-specified cut-offs are not reported. | Low: Wound age independently determined using police, witness, and medical records. | Low: All samples processed uniformly, post-mortem intervals reported, no unexplained exclusions. | Moderate |
| Ishida et al. [ | Low: Autopsy skin wounds with defined wound-age groups (0–12 h to 17–21 d); paired uninjured skin controls; confounding conditions excluded. | Low: IHC and morphometric quantification described; two investigators blinded; cut-offs biologically/statistically supported. | Low: Wound age determined independently from forensic documentation; not inferred from ORP150. | Low: Samples processed uniformly; PMI <3 days; predefined groups fully analyzed; no unexplained exclusions. | Low |
| Gauchotte [ | Low: Autopsy wounds, surgical intravital wounds, and post-mortem controls included; criteria clearly reported; no inappropriate enrichment. | Low: IHC assessment predefined with explicit thresholds (CD15 ≥4 cells/10 HPF; tryptase degranulation ≥20% + gradient); observers blinded; reproducibility assessed. | Low: Vitality defined using clear histological criteria; ex vivo post-mortem model strengthens reference validity. | Low: All samples underwent the same index tests; timing between injury, devascularization, and sampling documented. | Low |
| Kondo et al. [ | Low: 55 human skin wounds across defined age groups (0–12 h to 17–21 d) with paired controls; confounders excluded. | Low: IHC protocol and morphometric quantification clearly described; two blinded investigators; intranuclear Ub positivity assessed. | Low: Wound age independently established using forensic documentation and surgical/autopsy timing. | Low: Samples processed uniformly; PMI controlled; predefined groups fully analyzed; no unexplained exclusions. | Low |
| Grellner et al. [ | Low: Large series of human skin wounds with clearly defined wound-age groups; paired uninjured skin controls; no inappropriate exclusions. | Unclear: IHC (APAAP) and semi-quantitative scoring described; blinding and pre-specified cut-offs not reported. | Low: Wound age determined independently from surgical timing and forensic documentation. | Low: Samples processed uniformly; early/late intervals predefined; PMI reported; no unexplained exclusions. | Moderate |
| Grellner et al. [ | Low: Skin wounds from operations and autopsies chronologically dated; clear inclusion/exclusion; paired uninjured skin controls. | Low: IHC methods clearly described; assessors blinded; scoring criteria predefined; positive/negative controls used. | Low: Wound age determined independently from surgical records and forensic documentation. | Low: Samples processed uniformly; early/late intervals predefined; PMI reported; no unexplained exclusions. | Low |
| Kondo et al. [ | Low: 50 human autopsy skin wounds across defined age groups (0–12 h; 1–4 d; 7–14 d; 17–21 d) with paired controls; confounders excluded. | Low: IHC protocols and morphometric quantification described; two independent investigators; biologically meaningful cut-offs proposed. | Low: Wound age independently established using forensic documentation and autopsy timing. | Low: Uniform processing; PMI <3 days; predefined groups fully analyzed; no unexplained exclusions. | Low |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsWound Healing and Treatments · Pressure Ulcer Prevention and Management · Forensic Entomology and Diptera Studies
Introduction and background
Accurate estimation of wound age is a fundamental yet challenging task in forensic pathology, as it is crucial for reconstructing injury events, determining vitality, and establishing timelines relevant to investigations and judicial proceedings [1]. Distinguishing antemortem from postmortem injuries and estimating the time since wounding can influence interpretations of cause and manner of death and support or refute investigative hypotheses [2,3]. However, wound age estimation is complicated by the dynamic and multifactorial nature of tissue responses, interindividual variability, and postmortem changes [4].
Traditionally, estimation has relied on macroscopic examination and routine histopathology [5]. Classical histological features, such as hemorrhage, edema, inflammatory cell infiltration, and fibroblast proliferation, provide a general framework for assessing wound progression but often lack sensitivity and specificity, particularly in the early post-traumatic period [6]. Overlapping patterns across time intervals and the influence of postmortem changes and comorbidities further limit the reliability of conventional histology [7].
Recent advances in molecular biology and immunohistochemistry (IHC) have expanded the tools available to forensic pathologists [8]. Temporal expression of cellular markers, cytokines, growth factors, and stress-response proteins can provide more objective indicators of wound vitality and age [9]. Immunohistochemical techniques allow visualization of specific molecules involved in inflammation, angiogenesis, and tissue repair, helping define early, intermediate, and late phases of healing [10-15].
Despite these advances, the forensic application of these markers remains heterogeneous. Variations in study design, sample selection, wound types, analytical methods, and scoring systems, combined with methodological limitations, hinder the establishment of standardized approaches. No single marker or panel has been universally adopted, highlighting the need for systematic evaluation of existing evidence.
This systematic review aims to critically synthesize current evidence on histological and immunohistochemical markers for wound age estimation, assess their methodological quality, and clarify their diagnostic value, temporal reliability, and practical applicability in forensic practice.
Review
Methodology
Literature Search Strategy
This systematic review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. A comprehensive search was conducted across PubMed, Scopus, Web of Science, and the Cochrane Library from inception to the final search date. The search combined keywords and controlled vocabulary related to wound healing, forensic context, histological and immunohistochemical markers, and wound age. Terms included cytokines, chemokines, mast cell markers, leukocyte antigens, growth factors, coagulation-related proteins, and stress-response proteins. Searches were limited to human studies and original research, excluding reviews, editorials, conference abstracts without data, and non-relevant publications. Database-specific strategies ensured conceptual consistency across platforms (see Appendix 1).
Eligibility Criteria
Studies were included if they examined human skin wounds in a forensic context and assessed histological or immunohistochemical markers to estimate wound age or vitality. Included studies required known or reliably documented wound age and original data linking marker expression to post-traumatic intervals. Early, intermediate, and late wound phases were eligible. Excluded were animal-only studies, studies without forensic relevance, investigations not involving skin, studies limited to macroscopic or routine histology without marker analysis, and publications lacking sufficient methodological detail or outcomes. Non-English studies and case reports were also excluded. No restrictions were applied for geographic location or publication year.
Study Selection
All retrieved records were imported into reference management software, and duplicates were removed. Two reviewers independently screened titles and abstracts to exclude irrelevant studies, followed by full-text assessment against inclusion criteria. Discrepancies were resolved through discussion or consultation with a third reviewer. The selection process was documented using a PRISMA flow diagram, with reasons for exclusion recorded.
Data Extraction and Quality Appraisal
Two reviewers independently extracted data using a standardized form, including study design, forensic setting, sample characteristics, wound type and age, markers evaluated, analytical methods, scoring approaches, and key findings. Information on postmortem interval (PMI), control tissue use, and methodological limitations was also collected. Study quality and risk of bias were assessed using an adapted Quality Assessment of Diagnostic Accuracy Studies-2 (QUADAS-2) tool covering case selection, marker assessment, wound age determination, and flow/timing [17]. Each domain was rated as low, high, or unclear risk of bias, with justifications recorded. Discrepancies were resolved through discussion, and results informed the interpretation of the findings.
Results
Study Selection
A total of 5,740 records were identified, yielding 3,812 unique records after duplicate removal. Title and abstract screening excluded 3,721 records, primarily due to lack of forensic relevance, absence of wound age estimation, non-skin wounds, non-histological or non-immunohistochemical methods, animal-only studies, or non-original publication types. Ninety-one full-text articles were assessed, of which 80 were excluded for reasons including absence of a forensic context, lack of relevant markers, unclear wound timing, non-skin tissues, or unavailable data. Eleven studies [1-11] met all eligibility criteria and were included in the qualitative synthesis and risk-of-bias assessment (Figure 1).
PRISMA flow diagram illustrating the study selection processPRISMA flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies in the systematic review, including records retrieved through database searching, duplicates removed, full-text articles assessed for eligibility, and studies included in the final qualitative synthesis [16].
Study Characteristics
Most included studies were human autopsy-based observational investigations, commonly using non-injured skin as internal controls; one study involved living subjects with known wound ages. Sample sizes ranged from several dozen to several hundred specimens. Wound types included stab and incised wounds, lacerations, abrasions, contusions, surgical incisions, and blunt-force injuries. The temporal scope spanned minutes to several weeks post-injury, with studies typically categorizing wounds into predefined time intervals. Immunohistochemistry on paraffin-embedded sections was the principal method, assessing a broad range of inflammatory mediators, mast cell-related proteins, growth factors, stress-response proteins, and coagulation or extracellular matrix components using semi-quantitative, morphometric, or probability-based analyses (Table 1).
Quality Assessment of Included Studies
Using a tailored QUADAS-2 approach, case selection and reference standards were judged as low risk of bias across all studies, supported by clear inclusion criteria and independent wound timing sources. Variability was observed in the index test domain, with some earlier studies rated as unclear due to limited reporting on blinding or diagnostic thresholds, whereas more recent studies employed standardized scoring and explicit cut-offs. Flow and timing were generally low risk, with one study showing uncertainty due to reliance on witness-reported timing. Overall, most studies were rated as low risk of bias, with a minority classified as moderate quality due to index test reporting limitations (Table 2).
Qualitative Synthesis of Results
Very early wound age assessment demonstrated that immunohistochemical markers detect molecular changes within minutes, preceding histological inflammation. TNF-α-positive mast cells increased as early as 15 minutes and rose with survival time, distinguishing vital from post-mortem lesions [5]. Mast cell degranulation and early granulocyte markers were detectable within minutes, while coagulation-related markers showed rapid up-regulation with peak expression at short survival intervals, favoring vitality in probability-based models [1,7].
Early wound age within hours was characterized by transient mast cell increases peaking within the first few hours, followed by a decline, with consistently lower counts in post-mortem lesions [2]. Pro-inflammatory cytokines, including IL-1β, IL-6, and TNF-α, were up-regulated within minutes and peaked within the first 1-2 hours, providing temporal resolution before cellular infiltration [9].
Intermediate wound age was marked by evolving inflammatory infiltrates and early remodeling. CD14 expression increased within hours, peaked at 1-3 days, and declined thereafter, showing excellent discrimination for wounds aged 1-3 days [4]. Neutrophils peaked earlier than macrophages, while chemokines declined progressively; combined-marker models improved estimation for wounds younger than 10 days [3].
Late wound age estimation relied on stress-response and remodeling markers. Hypoxia-regulated proteins and ubiquitin showed minimal early expression, increased after one day, and peaked at 7-14 days before declining, with cell-type shifts reflecting granulation tissue development. Chemokines followed phase-dependent patterns with reduced but persistent expression in later wounds [6,8].
Discussion
This systematic review synthesizes histological and immunohistochemical markers for wound age estimation using a time-oriented framework that reflects the biological progression of wound healing. The findings confirm that wound repair begins immediately after injury and evolves through overlapping phases characterized by distinct cellular and molecular responses. Conventional histology alone shows limited sensitivity in the earliest post-traumatic period, whereas immunohistochemical markers related to haemostasis, inflammation, and immune activation provide improved temporal resolution. In particular, early expression of coagulation-related proteins, inflammatory cytokines, and mast cell activation markers appears valuable for distinguishing vital from non-vital wounds shortly after injury. As healing progresses, phase-specific immune cell infiltration and mediator expression allow more reliable differentiation of intermediate wound ages, especially when multiple markers are evaluated together rather than in isolation.
For later stages of wound healing, markers associated with angiogenesis, extracellular matrix remodeling, hypoxic stress, and fibroblast activity show more consistent patterns, although increasing biological variability limits precise dating. Across all time intervals, the review highlights that no single marker can reliably estimate wound age, emphasizing the importance of a multimodal approach integrating morphology with panels of complementary immunohistochemical markers. Interpretation remains constrained by methodological heterogeneity, lack of standardized scoring systems, and variability related to individual healing capacity and post-mortem factors. Future research should focus on well-characterized human studies with standardized protocols and validated cut-offs to improve forensic reliability and facilitate routine application in medicolegal practice.
Limitations
This review is limited by substantial methodological heterogeneity among included studies, including differences in wound types, sampling protocols, antibodies, scoring systems, and post-mortem intervals, which prevented quantitative meta-analysis. Many studies relied on semi-quantitative or observer-dependent assessments with limited reporting of diagnostic accuracy. Confounding factors such as comorbidities and environmental conditions were inconsistently addressed. Emerging molecular techniques, while promising, lacked standardization, limiting their applicability. These factors underscore the need for future research using harmonized methodologies and larger, well-characterized human datasets.
Conclusions
Wound age estimation remains a complex forensic challenge, especially in the early post-traumatic period, where conventional histology has limited sensitivity. Wound healing follows reproducible, phase-dependent molecular and cellular patterns that can guide temporal assessment. Early markers of haemostasis, mast cell activation, and cytokine release are informative within minutes to hours; immune cell and chemokine profiles provide resolution during intermediate phases; and markers of hypoxia response, angiogenesis, and tissue remodeling support dating in later stages. No single biomarker is sufficient across all phases, highlighting the value of integrated marker panels combined with morphological evaluation. Standardized protocols, digital quantification, and validation in human forensic material are essential to enhance accuracy, reproducibility, and reliability in wound age determination.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1A new method to determine wound age in early vital skin injuries: a probability scoring system using expression levels of Fibronectin, CD 62p and Factor VIII in wound hemorrhage Forensic Sci Int van de Goot FR Korkmaz HI Fronczek J 12813524420142523302110.1016/j.forsciint.2014.08.015 · doi ↗ · pubmed ↗
- 2Affinity cytochemistry analysis of mast cells in skin lesions: a possible tool to assess the timing of lesions after death Int J Legal Med Bonelli A Bacci S Norelli GA 33133411720031451768110.1007/s 00414-003-0396-1 · doi ↗ · pubmed ↗
- 3Analysis of inflammatory cells and mediators in skin wound biopsies to determine wound age in living subjects in forensic medicine Forensic Sci Int Fronczek J Lulf R Korkmaz HI 71324720152550666910.1016/j.forsciint.2014.11.014 · doi ↗ · pubmed ↗
- 4Detection of the timing of human skin wounds by immunohistochemical analysis of CD 14Arab J Forensic Sci Forensic Med Fouad AA Badr El Dine MMF El Dine Menesy MKH Abdelatif AA Abdelatif AA Khedr IR 1346135712019
- 5Early increase in TNF-alpha-containing mast cells in skin lesions Int J Legal Med Bacci S Romagnoli P Norelli GA Forestieri AL Bonelli A 13814212020061616354610.1007/s 00414-005-0030-5 · doi ↗ · pubmed ↗
- 6Expression of oxygen-regulated protein 150 (ORP 150) in skin wound healing and its application for wound age determination Int J Legal Med Ishida Y Kimura A Takayasu T Eisenmenger W Kondo T 40941412220081856342810.1007/s 00414-008-0255-1 · doi ↗ · pubmed ↗
- 7FVII Ira, CD 15, and tryptase performance in the diagnosis of skin stab wound vitality in forensic pathology Int J Legal Med Gauchotte G Wissler MP Casse JM 95796512720132374925610.1007/s 00414-013-0880-1 · doi ↗ · pubmed ↗
- 8Immunohistochemical detection of chemokines in human skin wounds and its application to wound age determination Int J Legal Med Kondo T Ohshima T Mori R Guan DW Ohshima K Eisenmenger W 879111620021205652610.1007/s 004140100260 · doi ↗ · pubmed ↗