Lecanemab over a two-year duration: Key insights from a regional specialty medical center
Lisa B.E. Shields, Hust Hannah, Gregory E. Cooper, Theresa Kluthe, Rachel N. Hart, Andrew P. Thaliath, Brandon C. Dennis, Stephanie W. Freeman, Jessica F. Cain, Whoy Y. Shang, Kendall M. Wasz, Adam T. Orr, Christopher B. Shields, Shirish S. Barve, Kenneth G. Pugh

TL;DR
This study examines the safety and outcomes of lecanemab treatment for Alzheimer's disease over two years, focusing on amyloid-related imaging abnormalities and patient characteristics.
Contribution
The study provides real-world data on lecanemab safety, particularly the risk of ARIA in APOE ε4 homozygous patients.
Findings
ARIA occurred in 22.3% of patients, with ε4 homozygotes having higher rates of ARIA compared to non-carriers.
Infusion-related adverse events decreased after introducing a pre-infusion medication cocktail.
Cognitive decline and ARIA progression were the main reasons for discontinuing lecanemab.
Abstract
The anti-amyloid monoclonal antibody lecanemab (Leqembi®) treats patients with mild cognitive impairment (MCI) or mild dementia due to Alzheimer’s disease (AD). We sought to evaluate the incidence of amyloid-related imaging abnormalities) ARIA and other adverse events associated with lecanemab. This retrospective and observational study features 187 patients who received at least one lecanemab infusion at our multidisciplinary Norton Neuroscience Institute Memory Center over a two-year duration (August 25, 2023-August 24, 2025). A total of 109 (58.3 %) patients were diagnosed with MCI, and 78 (41.7 %) had mild dementia prior to starting lecanemab. The mean age at the initial infusion was 73 years (Range: 49-90 years). Most (127 [67.9 %]) patients were female, and the majority (181 [96.8 %]) were Caucasian. Of the 175 patients who underwent at least one surveillance brain MRI following…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
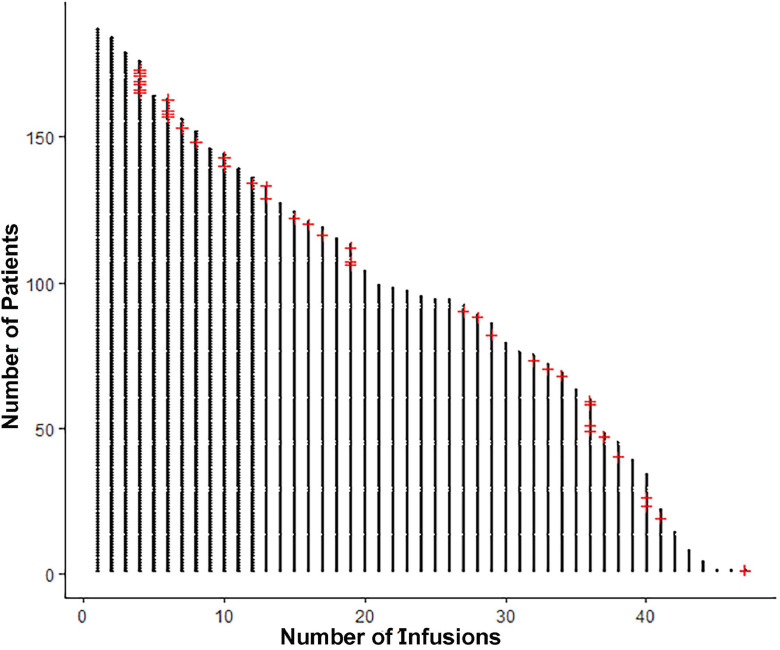 Figure 1
Figure 1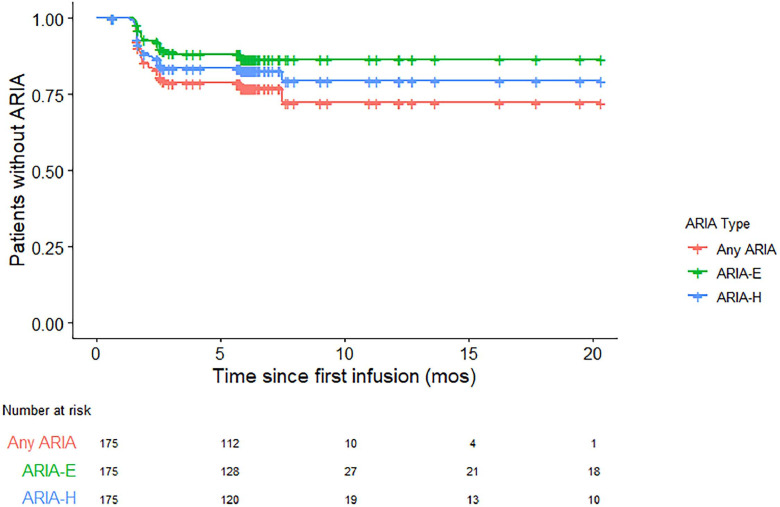 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer Immunotherapy and Biomarkers · Vasculitis and related conditions · Heparin-Induced Thrombocytopenia and Thrombosis
Introduction
1
In 2025 over 7 million Americans are living with Alzheimer’s disease (AD) which is projected to rise to approximately 13 million by 2050 [1]. Health and long-term care costs for individuals with dementia are estimated to be 1 trillion in 2050. The anti-amyloid monoclonal antibody lecanemab (Leqembi®) was approved by the U.S. Food and Drug Administration on July 6, 2023 to treat patients with mild cognitive impairment (MCI) or mild dementia due to AD [2,3]. Lecanemab decreased amyloid markers in mild dementia which led to a moderately slower rate of decline in measures of cognition and activities of daily living compared to placebo at 18 months in the phase 3 Clarity AD trial of lecanemab [4]. However, patients may develop amyloid-related imaging abnormalities (ARIA) with microhemorrhages (ARIA-H) or edema (ARIA-E) which may lead to either temporary suspension or permanent discontinuation of lecanemab. Other studies have confirmed that lecanemab may be well-tolerated, reduces the rate of clinical deterioration, and decreases brain amyloid-beta plaques, though infusion-related side effects and/or ARIA may arise [[5], [6], [7], [8], [9], [10], [11]]. Appropriate use recommendations have been published to address the challenges that providers may face when prescribing this drug and provide guidance regarding the surveillance and management of ARIA [2]. Clinicians, patients, and caregivers should be cognizant of the associated risks of lecanemab and closely monitor patients for adverse events throughout the duration of treatment [12].
Our Memory Center previously reported our initial experience treating patients with lecanemab over a six-month period (August 25, 2023 to March 1, 2024) [13]. Almost 25 % of the patients who completed one or more safety monitoring brain MRIs had ARIA detected. Most of these patients were asymptomatic and were either ε4 homozygous or ε4 heterozygous. Through our early use of lecanemab, we described several lessons learned from an organizational, clinical, and payment and insurance coverage standpoint [13].
Herein, we have expanded our previous lecanemab study and now report our experience with patients treated with lecanemab for MCI and mild dementia due to AD over a two-year period. The occurrence of ARIA on surveillance brain MRIs following lecanemab initiation is discussed. We also present the number of patients who have discontinued lecanemab and their reasons for doing so. Key insights through our ongoing use of lecanemab as well as future directions of lecanemab are described.
Methods
2
Study population and Memory Center team
2.1
Under an Institutional Review Board-approved protocol and according to the Declaration of Helsinki, we conducted a retrospective review of 187 patients treated with at least one lecanemab infusion at the Norton Neuroscience Institute Memory Center (NNI-MC) over a two-year duration (August 25, 2023-August 24, 2025). The inclusion and exclusion criteria as well as detailed descriptions of pre-lecanemab testing (CSF biomarkers, amyloid PET scans, baseline brain MRIs, ApoE genotyping, and cognitive testing [Mini-Mental State Examination [MMSE] or Montreal Cognitive Assessment [MoCA]) were previously described in our initial lecanemab publication [13]. Amyloid status was determined by one of the three options depending on individual clinical circumstances: CSF testing, an amyloid PET scan, or PrecivityAD2® (C_2_N Diagnostics; St. Louis, MO) blood test.
Patients were treated with intravenous (IV) lecanemab 10 mg/kg per infusion with an IV infusion administered every 2 weeks. After observing numerous side effects following the lecanemab infusions within the first several months of initiating this drug, every patient was pretreated with an oral cocktail of acetaminophen 650 mg, loratadine 10 mg, and famotidine 20 mg starting on December 31, 2023. After completing 18 months of lecanemab therapy, patients were given the option of receiving the infusion on a monthly basis instead of every 2 weeks [14]. Baseline brain MRIs were performed prior to the initial lecanemab administration, and surveillance MRIs were subsequently obtained before the 5^th^, 7^th^, and 14^th^ infusions [4]. If ARIA-H and/or ARIA-E was detected on surveillance MRIs, the patient required monthly MRIs until ARIA-E resolved or ARIA-H stabilized.
The NNI-MC is associated with Norton Healthcare which serves the regional, metropolitan community of Louisville, Kentucky. The Memory Center clinical capacity has increased exponentially over the past 4 years, from 928 new patients evaluated in 2021 to 2,573 in 2025 annualized. As of September 2025, our NNI-MC team consists of 2 neurologists, 2 geriatricians, 2 physician assistants, 1 neuropsychologist, 1 neuropsychometrist, 1 nurse practitioner, 1 full-time nurse navigator, 4 medical assistants, 1 MRI scheduler, 1 pharmacist, and the authorization team. In addition to the NNI-MC team, several other resources are valuable to effectively and safely treat patients, including the task force administration, infusion members, an MRI scheduler just for the surveillance brain MRIs, and the billing and coding team.
Several metrics were collected including the patient’s age, gender, race, Body Mass Index (BMI), highest level of education, medical specialty of the referring physician, comorbidities, payer of lecanemab, MMSE/MoCA scores, ApoE genotype, medications for MCI/AD (donepezil, memantine, galantamine, rivastigmine), ARIA-H and/or ARIA-E on surveillance brain MRIs, and infusion-related side effects. The severity of ARIA-H and ARIA-E was also determined [2,15,16]. Management of ARIA was based on the phase III Clarity AD trial [4] and the lecanemab appropriate use recommendations [2]. At the 2-year mark of infusing lecanemab, we assessed how many patients continued to be administered lecanemab and the reasons that patients discontinued this drug. A comparison of MMSE scores at baseline and between 1-2 years post-lecanemab was also performed. We initially analyzed these metrics in all 187 patients who received at least one lecanemab infusion. We subsequently performed an evaluation of a subset of patients who had undergone at least one surveillance brain MRI following the start of lecanemab, specifically, patients who were treated with at least 4 lecanemab infusions.
Statistical analysis
2.2
Patient demographics, comorbidities, and baseline brain MRI findings were compared between those who had no evidence of ARIA on surveillance brain MRI scans and those who had any ARIA, solitary ARIA-H, and solitary ARIA-E using Kruskal-Wallis tests for the continuous variables and Chi-squared tests or Fisher’s exact test for categorical variables as appropriate depending on the number of subjects per category. ARIA rates and patients who were symptomatic with ARIA were compared between patients with the lowest quartile baseline MMSE scores (≤ 23) and those with the highest quartile baseline MMSE scores (≥ 27) by the same tests described above. A multivariate binomial regression was performed, predicting symptomatic ARIA by the diagnosis (MCI versus mild dementia) and MMSE scores. These tests were performed on R version 4.2.3 (2023-03-15 ucrt).
Ethical approval and informed consent
2.3
The WCG Institutional Review Board (IRB) determined that this retrospective study was exempt under 45 CFR 46.104(d)(4). The IRB number is 2024-0001, and the IRB approval was dated January 3, 2024. According to federal regulations, the IRB of record determined that this study was exempt Category 4 with a complete waiver of consent and authorization.
Results
3
Clinical characteristics
3.1
A total of 109 (58.3 %) patients were diagnosed with MCI, and 78 (41.7 %) had mild dementia due to AD prior to starting lecanemab (Table 1). The mean age at the initial infusion was 73 years (Range: 49-90 years). Most (127 [67.9%]) patients were female, and the majority (181 [96.8%]) were Caucasian. Most (141 [75.4%]) patients had pursued higher education (education beyond high school). Most patients (177 [94.6%]) had been treated with medications for MCI/AD, with donezepil as the most common (164 [87.l7%]).Table 1. Characteristics of patients treated with lecanemab at our Memory Center.Table 1 dummy alt textFeaturesNumber of patients (n=187)Diagnosis MCI109 (58.3 %) Mild dementia78 (41.7 %)**Age at 1^st^ lecanemab infusion (years)**Mean: 73 years (Range: 49-90 years) < 6520 (10.7 %) 66-7486 (46.0 %) 75-8476 (40.6 %) > 855 (2.7 %)Gender Female127 (67.9 %) Male60 (32.1 %)Race Non-Hispanic White181 (96.8 %) African-American5 (2.7 %) Asian1 (0.5 %)Body Mass Index at 1^st^ lecanemab infusionMean: 26.0 (Range: 17.6-45.0) < 19.912 (6.4 %) 20.0-24.968 (36.4 %) 25.0-29.979 (42.2 %) 30.0-34.922 (11.8 %) 35.0-39.93 (1.6 %) > 40.03 (1.6 %)Highest level of education Did not complete high school5 (2.7 %) High school graduate41 (21.9 %) Some college24 (12.8 %) Technical school after high school5 (2.7 %) Associate’s degree11 (5.9 %) College graduate49 (26.2 %) Post-college degree *47 (25.1 %) Unknown5 (2.7 %)Medical specialty of referring physician Primary Care Provider151 (80.7 %) Self-referral17 (9.1 %) Neurologist15 (8.0 %) Other4 (2.1 %)Comorbidities Dyslipidemia141 (75.4 %) Hypertension86 (46.0 %) Cardiovascular disease (other than hypertension)60 (32.1 %) Diabetes mellitus35 (18.7 %)Payer of lecanemab Medicare143 (76.5 %) Medicare A and B (“traditional” Medicare) 87 (60.8 %) Medicare Advantage/Replacement 56 (39.2 %) Patient Assistance Program31 (16.6 %) Commercial insurance13 (6.9 %)Medications for mild cognitive impairment/AD Donepezil164 (87.7 %) Memantine103 (55.1 %) Galantanime10 (5.3 %) Rivastigmine12 (6.4 %) None10 (5.3 %)Testing for AD CSF165 (88.2 %) PET scan (amyloid)18 (9.6 %) Blood test to detect status of amyoid pathology13 (7.0 %)APOE ε4 status ε4 Heterozygote102 (54.5 %) ε4 Homozygote27 (14.4 %) ε4 Non-carrier58 (31.0 %)Findings on baseline brain MRI Subcortical hyperintensities165 (88.2 %) Mild 137 (83.0 %) Moderate 28 (17.0 %) Microbleeds20 (11.4 %)Baseline MMSE/MoCA Scores MMSE (n=148 [79.1 %])Mean: 25 (Range: 19-30) MoCA (n=39 [20.9 %])Mean: 21 (Range: 14-28)MCI: Mild cognitive impairmentAD: Alzheimer’s disease⁎Post-college degree: Master’s, PhD, MD, JD
Testing prior to lecanemab infusion
3.2
Patients who received lecanemab had either positive CSF biomarkers (165 [88.2 %]), a positive amyloid PET scan (18 [9.6 %]), and/or positive plasma based biomarkers for AD (PrecivityAD2®) (13 [7.0 %]) (Table 1). Nine (4.8 %) patients underwent testing for plasma based biomarkers for AD without undergoing CSF or amyloid PET scan testing.
A total of 102 (54.5 %) patients were ε4 heterozygous, 27 (14.4 %) were ε4 homozygous, and 58 (31.0 %) were ε4 non-carriers. The number of patients with the following findings on baseline brain MRI included: four or fewer microbleeds (17 [9.1 %]) and subcortical hyperintensities (165 [88.2 %]), the latter of which were mild in 137 (83.0 %) patients and moderate in 28 (17.0 %) patients. Of the 148 (79.1 %) patients who underwent MMSE testing and 39 (20.9 %) patients who had MoCA testing, the mean baseline scores were 25 and 21, respectively.
ARIA-H and ARIA-E detected on surveillance brain MRI
3.3
Fig. 1 depicts when ARIA was detected on surveillance brain MRIs among all patients treated with lecanemab. Of the 175 patients who underwent at least one surveillance brain MRI scan following lecanemab initiation, 39 (22.3 %) had evidence of ARIA (Table 2, Table 3). Both ARIA-H and ARIA-E were present in 13 [33.3 %], solitary ARIA-H was observed in 17 [43.6 %], and solitary ARIA-E was detected in 9 [23.1 %]). Of the 39 patients with ARIA, 20 (51.3 %) were ε4 heterozygous, 12 (30.8 %) were ε4 homozygous, and 7 (17.9 %) were ε4 non-carriers. Patients who were ε4 homozygous more frequently had evidence of any ARIA (ARIA-H and ARIA-E) (p-value = 0.002), solitary ARIA-E (p = 0.041), and solitary ARIA-H (p = 0.004) (Table 4). Of the 25 patients who underwent at least one surveillance brain MRI and were ε4 homozygous, 12 (48.0 %) had ARIA detected. Of the 95 patients who underwent at least one surveillance brain MRI and were ε4 heterozygous, 20 (21.0 %) had ARIA detected. Of the 55 patients who underwent at least one surveillance brain MRI and were ε4 non-carriers, 7 (12.7 %) had ARIA detected. Patients with more baseline microbleeds more frequently developed any ARIA (ARIA-H and ARIA-E) (p = 0.041) and solitary ARIA-H (p = 0.022), as determined by the Kruskal-Wallis Test and operationalized as a continuous variable. The presence of baseline microbleeds was associated with a higher frequency of solitary ARIA-H, though was only marginally statistically significant (p = 0.051).Fig. 1. The detection of ARIA-H and ARIA-E on surveillance brain MRIs in relation to the number of lecanemab infusions. Each dot represents one infusion. Each red plus sign indicates the detection of ARIA (n=39).Fig 1 dummy alt textTable 2Status of patients treated with lecanemab at our Memory Center at the two-year mark.Table 2 dummy alt textFeaturesNumber of patients (n=187)ARIA-H/ARIA-E detected on surveillance brain MRI (n=175) Yes39 (20.8 %) Solitary ARIA-H 17 (43.6 %) Solitary ARIA-E 9 (23.1 %) Both ARIA-H and ARIA-E 13 (33.3 %)ARIA-H/ARIA-E detected on surveillance brain MRI (n=39) ε4 Homozygote12 (30.8 %) ε4 Heterozygote20 (51.3 %) ε4 Non-carrier7 (17.9 %)APOE ε4 status and detection of ARIA-H/ARIA-E on surveillance brain MRI ε4 Homozygote (n=25)12 (48.0 %) ε4 Heterozygote (n=95)20 (21.0 %) ε4 Non-carrier (n=55)7 (12.7 %)ARIA-H/ARIA-E first detected on surveillance brain MRI (n=39) Before 5^th^ infusion29 (74.4 %) Before 7^th^ infusion7 (17.9 %) Before 14^th^ infusion3 (7.7 %)Infusion-related adverse effects Yes60 (32.1 %) No127 (67.9 %)Infusion-related adverse effects following 1^st^ lecanemab infusion and when they started Yes54 (28.9 %) At Infusion Center (0–3 h) 14 (25.9 %) 3–24 h post-infusion 36 (66.7 %) 24–48 h post-infusion 2 (3.7 %) > 48 h post-infusion 2 (3.7 %) No133 (71.1 %)Infusion-related adverse effects before and after pre-infusion cocktail (December 31, 2023) Before pre-infusion cocktail (n=42)19 (45.2 %) After pre-infusion cocktail (n=145)41 (28.3 %)Status of lecanemab infusions Ongoing155 (82.9 %) Discontinued32 (17.1 %) Progressive cognitive decline/delusions/agitation 10 (31.2 %) ARIA progression 9 (28.1 %) Moved to different city/state 3 (9.4 %) Focus on other medical conditions 3 (9.4 %) Need for continued anticoagulation 3 (9.4 %) Surveillance brain MRI detected bilateral SDH 1 (3.1 %) Pursue conservative treatment (not lecanemab) 1 (3.1 %) Non-compliant with infusions 1 (3.1 %) Died after 1^st^ infusion (most likely cardiac-related) 1 (3.1 %)Number of lecanemab infusionsMean: 24 (Range: 1-47) 1-311 (5.9 %) 4-1037 (19.8 %) 11-2040 (21.4 %) 21-3022 (12.3 %) 31-4056 (29.9 %) > 4021 (11.2 %)Comparison of MMSE scores at baseline and after 1 year post-lecanemab (n=73) Increased13 (17.8 %) Decreased51 (69.9 %) Same9 (12.3 %)Table 3ARIA-H and ARIA-E in patients treated with lecanemab at our Memory Center.Table 3 dummy alt textPatient #Age/ GenderCo-morbiditiesAPOE4 GenotypeBrain MRI Prior to Lecanemab InfusionSurveillance Brain MRIsMRIs Following ARIA DetectionSymptomatic/ Lecanemab Permanently Suspended167/MHTN, HC, DMε4/ε42 foci cerebral microbleedsBefore 5^th^ infusion: 3 new foci ARIA-H for total of 5 [Moderate]; lecanemab held1^st^ MRI following ARIA: negative for new ARIA- H and ARIA-E; lecanemab resumedNo280/MHTN, HC, DM, CVD *ε3/ε42 foci superficial siderosis each less than 1 cm in diameterBefore 5^th^ infusion: 9 new foci ARIA-H [Moderate], unchanged appearance of superficial siderosis (less than 1 cm in diameter); lecanemab held1^st^ MRI following ARIA: 1 new focus ARIA-H [Severe], unchanged appearance of superficial siderosis (less than 1 cm in diameter); 2^nd^ MRI following ARIA: 1 new focus ARIA-H [Severe]; lecanemab not resumedNo/Yes after the 4^th^ infusion372/MHC, DM, CVD ; Aspirin 81 mgε3/ε4No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 1 focus ARIA-E (8.0 mm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA: negative for new ARIA-H and ARIA-E, previous focus of ARIA-E resolvedNo477/FHTNε3/ε3No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 4 new foci ARIA-H [Mild] and 1 new focus ARIA-E (4.0 cm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA negative for new ARIA-H, decreased size of ARIA-E (3.7 cm in diameter), and 1 new infarct (7.0 mm in diameter) in the left cerebellar hemisphereNo574/MHCε3/ε3No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 1 focus ARIA-E (4.2 cm in diameter) [Mild] and 1 focus of ARIA-H [Mild]; lecanemab continued1^st^ MRI following ARIA: 1 new focus ARIA-E (less than 1 cm in diameter) and increased size of previous focus of ARIA-E (5.8 cm in diameter) [Moderate]; lecanemab suspended; 3^rd^ MRI following ARIA: resolution of ARIA-E and ARIA-H; lecanemab resumedNo671/FNone; Aspirin 81 mgε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 6 foci ARIA-H [Moderate] and 1 new focus ARIA-E (6.0 cm in diameter) [Moderate]; lecanemab suspended1^st^ MRI following ARIA: 5 new ARIA-H [Severe] and decrease in size of previous ARIA-E (3.0 cm) [Mild]Yes (headaches)/Yes after the 4^th^ infusion771/FHCε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-E (less than 1 cm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA: ARIA-E resolved; 4^th^ MRI following ARIA: 1 focus ARIA-E (less than 5 cm in diameter) [Mild]; 5^th^ MRI after ARIA: increased size of ARIA-E (3.2 cm in diameter) [Mild]; 6^th^ MRI after ARIA: 2 new foci ARIA-E (0.5 cm and 2.2 cm in diameter) [Moderate]; lecanemab suspended after 17^th^ infusion due to headaches and persistent ARIA-EYes (headaches)/Yes after the 17^th^ infusion875/FHTN, HCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-H [Mild]; lecanemab continued1^st^ MRI following ARIA negative for new ARIA-H and ARIA-ENo974/FHTN, HCε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-E (1.8 cm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA: increased size of ARIA-E (2.2 cm in diameter) and 1 new focus ARIA-E (3.0 cm) [Moderate]; lecanemab suspendedNo/Yes after the 36^th^ infusion1073/FHCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-E (3.0 cm in diameter) [Mild] and 4 new ARIA-H [Mild]; lecanemab suspended due to ARIA and symptoms1^st^ MRI following ARIA: increased size of ARIA-E (3.4 cm) and 4 new foci of ARIA-H [Moderate]; 2^nd^ MRI following ARIA: ARIA-H stable [Mild] and ARIA-E decreased in size [Mild]; 3^rd^ and 4^th^ MRIs following ARIA: resolution of ARIA-H and ARIA-E; lecanemab resumed; 5^th^ MRI following ARIA: 3 new foci ARIA-H [mild]; lecanemab continued; 6^th^ MRI following ARIA: stable ARIA-H [mild]; lecanemab continuedYes (fatigue/disorientation for several days after 4^th^ infusion)1171/FHCε2/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion, 2 new foci ARIA-H [Mild]; lecanemab continuedNo1274/FNoneε2/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion, 2 new foci ARIA-H [Mild]; lecanemab continuedNo1363/MNoneε2/ε3No evidence of microbleeds or vasogenic edemaBefore 14^th^ infusion: 1 new focus ARIA-E (5.0 mm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA: ARIA-E resolvedNo1464/MHCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 4 foci ARIA-H [Mild] and 1 new focus ARIA-E (2.0 cm in diameter) [Mild]; lecanemab continued1^st^ MRI following ARIA: 11 new foci ARIA-H for total of 15 [severe] and increased size of ARIA-E (5.5 cm in diameter) [moderate]; lecanemab discontinued after 6^th^ infusionNo/Yes after the 6^th^ infusion1570/FNoneε3/ε3No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 3 new foci ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: 1 new focus ARIA-H for total of 4 [mild] and 1 new focus ARIA-E (2.0 cm in diameter) [mild]; lecanemab discontinued after 6^th^ infusionNo/Yes after the 6^th^ infusion1680/FHTN, HCε3/ε41 focus cerebral microbleedBefore 5^th^ infusion: 1 new focus ARIA-H [mild] and 1 focus ARIA-E (3.0 cm in diameter) [mild]; lecanemab continued1^st^ MRI following ARIA: 2 new foci ARIA-H for total of 3 [mild] and increased size of ARIA-E (4.5 cm in diameter) [mild]No1772/MNoneε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no new ARIA-H [mild]No1877/FHTNε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 new focus ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: 1 new focus ARIA-H for total of 2 [mild]; lecanemab held and discontinued after 8^th^ infusion; 4^th^ surveillance MRI: 7 new foci ARIA-H [moderate]No/Yes after the 8^th^ infusion1976/FHCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-E (sulcal effusion) [mild]; lecanemab continued1^st^ MRI following ARIA: ARIA-E resolvedNo2069/FHC, CVε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No2170/MHTN, HC, CVε3/ε3No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No2272/FNoneε3/ε41 focus cerebral microbleedBefore 5^th^ infusion: 2 foci ARIA-E (5.5 cm and 4.2 cm in diameter) [moderate]; lecanemab held1^st^ MRI following ARIA: decreased size in ARIA-E (3.9 cm and 4.2 cm) [mild]; lecanemab resumed after 4^th^ surveillance MRI; 6^th^ surveillance MRI: 4 new ARIA-E (all with diameter less than 1.0 cm) [moderate]; lecanemab discontinued after 15^th^ infusionNo/Yes after the 15^th^ infusion2376/MHC, CVε3/ε42 foci cerebral microbleedsBefore 5^th^ infusion: 1 new focus ARIA-H for total of 3 [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No2471/FHTNε3/ε42 foci cerebral microbleedsBefore 5^th^ infusion: 1 new focus ARIA-H for total of 3 [mild]; lecanemab continued1^st^ MRI following ARIA: 1 new ARIA-H for total of 4 [mild]No2566/MNoneε3/ε4No evidence of microbleeds or vasogenic edemaBefore 14^th^ infusion: 3 new foci ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No2680/FHC, DMε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 new focus ARIA-H [mild] and 1 new focus ARIA-E (2.4 cm in diameter) [mild]; lecanemab held1^st^ MRI following ARIA: no change in ARIA-H [mild] and decreased size of ARIA-E (1.3 cm in diameter) [mild]; lecanemab discontinued after 4^th^ infusionNo/Yes after the 4^th^ infusion2769/MHC/DMε4/ε4No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 5 new foci ARIA-H [moderate] and 1 new focus ARIA-E (1.4 cm in diameter) [mild]; lecanemab held1^st^ MRI following ARIA: 1 new focus ARIA-H for total of 6 [moderate] and resolution of ARIA-E; lecanemab still suspended; 4^th^ surveillance MRI: no change in ARIA-H [moderate]; lecanemab resumed after 4^th^ surveillance MRINo2886/FHTN, HC, CVε3/ε3No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 3 foci ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: 1 new focus ARIA-H for total of 5 [moderate]; lecanemab held; 3^rd^ surveillance MRI: no change in ARIA-H [moderate] and 1 new focus ARIA-E (0.5 cm in diameter) [mild]; lecanemab still held; 4^th^ surveillance MRI: no change in ARIA-H [moderate] and resolution of ARIA-E; lecanemab resumed after 4^th^ surveillance MRINo2966/MHTN, HCε2/ε4No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 1 new focus ARIA-E (3.7 cm in diameter) [mild]; lecanemab held since symptomatic1^st^ MRI following ARIA: resolution of ARIA-E; lecanemab resumed after 3^rd^ surveillance MRIYes (headaches)3085/FHCε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 3 new ARIA-H [mild] and 2 foci ARIA-E (3.2 cm and 1.7 cm in diameter) [moderate]; lecanemab held1^st^ MRI following ARIA: 2 new foci ARIA-H for total of 5 [moderate] and decreased size of ARIA-E [moderate]; lecanemab held; lecanemab discontinued after 4^th^ infusionNo/Yes after 4^th^ infusion3174/FHTN, HCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 new focus ARIA-H [mild] and 1 focus ARIA-E (3.4 cm in diameter) [mild]; lecanemab continued1^st^ MRI following ARIA: 1 new focus ARIA-H for total of 2 [mild] and increased size of ARIA-E (4.1 cm in diameter) [mild]; lecanemab continued; 5^th^ surveillance MRI: 8 new ARIA-H for total of 10 [moderate] and resolution of ARIA-E; 7^th^ surveillance MRI: no change in ARIA-H [moderate]; lecanemab resumed after 7^th^ surveillance MRINo3279/FHC, DMε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 new focus ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No331 focus cerebral microbleedBefore 7^th^ infusion: 2 new foci ARIA-H for total of 3 [mild]; lecanemab continued1^st^ MRI following ARIA: 2 new foci ARIA-H for total of 5 [moderate]; lecanemab held; 3^rd^ surveillance MRI: no change in ARIA-H [moderate]; lecanemab discontinued after 6^th^ infusionNo/Yes after 6^th^ infusion3469/FHCε3/ε4No evidence of microbleeds or vasogenic edemaBefore 14^th^ infusion: 7 new ARIA-H [moderate] and 1 new ARIA-E (sulcal effusion) [mild]; lecanemab heldNo3563/MHCε4/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 focus ARIA-E (less than 1 cm in diameter) [mild]; lecanemab held since symptomatic1^st^ MRI following ARIA: resolution of ARIA-E; lecanemab discontinued after 4^th^ infusionYes (smelling gas odor, weak, clammy, fatigue)/Yes after 4^th^ infusion3684/FHTN, HC, CVε2/ε4No evidence of microbleeds or vasogenic edemaBefore 7^th^ infusion: 1 new ARIA-H [mild]; lecanemab continued1^st^ MRI following ARIA: no change in ARIA-H [mild]No3779/FHTNε3/ε3No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 2 foci of ARIA-H (superficial siderosis) [moderate]; lecanemab held1^st^ MRI following ARIA: no change in ARIA-H [moderate]; lecanamab resumedNo3878/FHCε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 2 new foci ARIA-H [mild] and 4 new foci ARIA-E (3.0 cm, 1.8 cm, 1.5 cm, and 1.0 cm in diameter) [moderate]; lecanemab heldNo/Yes after 4^th^ infusion39ε3/ε4No evidence of microbleeds or vasogenic edemaBefore 5^th^ infusion: 1 new focus ARIA-H (superficial siderosis) [mild]; lecanemab continued1^st^ MRI following ARIA: resolution of ARIA-H; lecanemab discontinued after 6^th^ infusionNo/Yes after 6^th^ infusionARIA-H: amyloid-related imaging abnormalities-hemorrhage.ARIA-E: amyloid-related imaging abnormalities-edema.HTN: hypertension.HC: hypercholesterolemia.DM: diabetes mellitus.CV: cardiovascular disease excluding hypertension.Table 4. Baseline characteristics of patients with and without amyloid-related imaging abnormalities (ARIA).Table 4 dummy alt textOVERALLNO ARIAANY ARIAP-VALUESOLITARY ARIA-EP-VALUESOLITARY ARIA-HP-VALUEN175136392230AGE (MEAN (SD))73.18 (6.19)72.99 (6.24)73.87 (6.02)0.432172.50 [69.50, 76.75]0.725174.00 [71.00, 79.00]0.2021SEX (%)0.6272>0.99920.9752 MALE55 (31.4)41 (30.1)14 (35.9)7 (31.8)10 (33.3) FEMALE120 (68.6)95 (69.9)25 (64.1)15 (68.2)20 (66.7)RACE (%)0.25430.55930.1623 CAUCASIAN169 (96.6)132 (97.1)37 (94.9)21 (95.5)28 (93.3) AA4 (2.3)2 (1.5)2 (5.1)1 (4.5)2 (6.7) ASIAN2 (1.1)2 (1.5)0 (0.0)0 (0.0)0 (0.0)MMSE SCORE (MEDIAN [IQR])25.00 [23.00, 27.00]25.00 [23.00, 27.00]24.00 [23.75, 26.00]0.155124.00 [24.00, 26.00]0.543124.00 [24.00, 25.00]0.1871APOE ε4 STATUS (%)****0.00220.04120.004**2 HOMOZYGOTE25 (14.3)13 (9.6)12 (30.8)7 (31.8)10 (33.3) HETEROZYGOTE95 (54.3)75 (55.1)20 (51.3)10(45.5)14 (46.7) NON-CARRIER55 (31.4)48 (35.3)7 (17.9)5 (22.7)6 (20.0)**BASELINE MICROBLEEDS (%)**0.08220.72120.0512 NO155 (88.6)124 (91.2)31 (79.5)19 (86.4)23 (76.7) YES20 (11.4)12 (8.8)8 (20.5)3 (13.6)7 (23.3)**BASELINE # OF MICROBLEEDS (MEDIAN [IQR])0.00 [0.00, 0.00]0.00 [0.00, 0.00]0.00 [0.00, 0.00]0.04110.00 [0.00, 0.00]0.74710.00 [0.00, 0.00]0.0221BASELINE INFARCTS (%)**0.51730.6930.7113 NO161 (92.0)126 (92.6)35 (89.7)20 (90.9)27 (90.0) YES14 (8.0)10 (7.4)4 (10.3)2 (9.1)3 (10.0)**HIGHER EDUCATION (%)**0.31820.47620.8342 NO40 (23.5)28 (21.4)12 (30.8)7 (31.8)8 (26.7) YES130 (76.5)103 (78.6)27 (69.2)15 (68.2)22 (73.3)**HYPERTENSION (%)**0.39620.10320.9312 NO95 (54.3)71 (52.2)24 (61.5)16 (72.7)17 (56.7) YES80 (45.7)65 (47.8)15 (38.5)6 (27.3)13 (43.3)**DYSLIPIDEMIA (%)**0.6992>0.99920.5992 NO43 (24.6)32 (23.5)11 (28.2)5 (22.7)9 (30.0) YES132 (75.4)104 (76.5)28 (71.8)17 (77.3)21 (70.0)CARDIOVASCULAR (%)0.10320.02320.3312 NO118 (67.4)87 (64.0)31 (79.5)20 (90.9)23 (76.7) YES57 (32.6)49 (36.0)8 (20.5)2 (9.1)7 (23.3)**DIABETES (%)**0.76720.7582>0.9992 NO143 (81.7)110 (80.9)33 (84.6)19 (86.4)25 (83.3) YES32 (18.3)26 (19.1)6 (15.4)3 (13.6)5 (16.7)DIAGNOSIS (%)>0.99920.792>0.9992 MCI104 (59.4)81 (59.6)23 (59.0)12 (54.5)18 (60.0) EARLY AD71 (40.6)55 (40.4)16 (41.0)10 (45.5)12 (40.0)**BMI (MEDIAN [IQR])**25.43 [22.68, 28.55]25.73 [23.04, 28.61]24.72 [22.20, 27.94]0.402123.74 [21.87, 28.06]0.329124.24 [22.17, 27.27]0.11111= Kruskal-Wallis Test2= Chi-Squared Test3= Fisher’s Exact TestAA: African AmericanMCI: mild cognitive impairmentAD: Alzheimer’s diseaseBMI: body mass index.
Five (12.8 %) patients with ARIA were symptomatic, necessitating lecanemab suspension (Table 3). Three of these symptomatic patients were ε4 homozygous, and two were ε4 heterozygous. Patient #6 had headaches when ARIA was detected on the surveillance brain MRI before the 5^th^ infusion. The lecanemab was permanently suspended, and the headaches resolved after the discontinuation of lecanemab. Patient #7 experienced headaches after the 17^th^ infusion. Due to persistent ARIA-E, the lecanemab was permanently suspended. The headaches subsequently resolved. Patient #10 had ARIA detected before the 5^th^ infusion at which time the patient was complaining of fatigue and disorientation. Due to her ε4 homozygous status, the lecanemab was temporarily suspended and the symptoms resolved. The patient resumed lecanemab after the 4^th^ MRI following ARIA, and no further symptoms occurred. Patient #29 had headaches when the surveillance brain MRI was performed before the 7^th^ infusion. The lecanemab was held, and the headaches resolved. The lecanemab was subsequently resumed after the third surveillance MRI, with no associated side effects. Patient #35 experienced numerous symptoms of smelling a gas odor, weakness, clamminess, and fatigue when ARIA was detected on the surveillance brain MRI was performed before the 5^th^ infusion. Due to these symptoms, the lecanemab was permanently suspended.
ARIA was most commonly detected on the surveillance brain MRI performed before the 5^th^ infusion (29 [74.4 %] patients) (Fig. 2). Of the patients who underwent at least one surveillance brain MRI and had baseline MMSE testing, there were no significant differences in the rates of any ARIA (both ARIA-H and ARIA-E) (p = 0.545), solitary ARIA-H (p = 0.43), or solitary ARIA-E (>0.999) or patients who were symptomatic with ARIA (p = 0.493) comparing patients with the lowest quartile (≤ 23; n = 38 [28 %]) to those with the highest quartile (≥ 27; n = 37 [27 %]) of MMSE scores. A multivariate regression revealed that diagnosis (MCI versus mild dementia) was not a significant predictor of symptomatic ARIA (OR = 2.034 [0.311–16.424], p-value = 0.457). Additionally, MMSE score was not a significant predictor of symptomatic ARIA (OR = 1.108 [0.762-1.63], p-value = 0.588).Fig. 2. The percentage of patients without evidence of ARIA over a two-year duration.Fig 2 dummy alt text
Infusion-related side effects
3.4
A total of 60 (32.1 %) patients experienced infusion-related adverse effects, 54 (90.0 %) of which occurred after the first lecanemab infusion (Table 2). Mild and transient headaches were most common, affecting 26 (48.1 %) of these patients after the first infusion. The side effects were reported either at the infusion center [0–3 h] (14 [25.9 %] patients) or between 3–24 h post-infusion (36 [66.7 %]). Of the 42 patients who received lecanemab before the pre-infusion cocktail was implemented, 19 (45.2 %) experienced an infusion-related adverse event (Table 2). Of the 145 patients who were treated with lecanemab after the pre-infusion cocktail was incorporated, 41 (28.3 %) had an infusion-related adverse event.
Status of lecanemab at the two-year mark of its use at our Memory Center
3.5
A total of 155 (82.9 %) patients continued to receive infusions at the two-year mark, while 32 (17.1 %) had discontinued lecanemab (Table 2). The mean number of lecanemab infusions per patient completed at the two-year mark was 24 (Range: 1-47). No patient elected to stop therapy after 18 months; all have continued infusions either every 2 or 4 weeks. Of the 32 patients who discontinued lecanemab, 10 (31.2 %) stopped lecanemab due to cognitive decline, delusions, and/or agititation associated with progression of the AD disease and 9 (28.1 %) discontinued lecanemab due to ARIA progression. Of these latter 9 patients, 4 were ε4 homozygous, 4 were ε4 heterozygous, and 1 was a ε4 non-carrier. Other reasons for suspending lecanemab are described in Table 2. Two patients died who were treated with lecanemab. One death occurred within several hours of the first infusion and was most likely cardiac-related. This case was described in detail within our initial lecanemab publication.^13^ The second patient, an 80-year-old female who was ε4 heterozygous with a history of dyslipidemia, had no evidence of ARIA on surveillance brain MRIs. After her 15^th^ and 16^th^ infusions, she was evaluated in the Emergency Department for aggression and hallucinations. These symptoms were most likely due to progressive dementia. The lecanemab was discontinued after her 19^th^ infusion. Two months later, the patient experienced a seizure and lost consciousness, was admitted to the hospital for 5 days, and was diagnosed with atrial fibrillation, a left bundle branch block, and a urinary tract infection. She died one month later.
Of the 73 patients who underwent MMSE testing prior to starting lecanemab and after the 1-year mark, 51 (69.9 %) had decreased MMSE scores, 13 (17.8 %) had increased MMSE scores, and 9 (12.3 %) had the same score (Table 2). Of the 13 patients whose MMSE scores increased from baseline to 1-year post-lecanemab, 7 had increased by one point, 3 by 2 points, 1 by 3 points, and 2 by 4 points. Of the 7 patients whose scores increased by more than one point, 4 were ε4 non-carriers, 2 were ε4 heterozygous, and 1 was ε4 homozygous. Comparing the 51 patients with a decreased MMSE score after 1-year post-infusion to the 22 patients with no decrease in MMSE scores (the MMSE score either stayed the same or improved), there was no significant association between any of the variables (patient age, sex, ApoE status, any ARIA, ARIA-H, and ARIA-E) and a decrease in MMSE scores (Supplemental Table 1). A multinomial binomial regression predicting the decrease in MMSE scorers controlling for age, gender, and ApoE status revealed that none of the variables were significant predictors for a decrease in MMSE scores (Supplemental Table 2) or a change in MMSE scores (Supplemental Table 3). Supplemental Figure 1 depicts a spaghetti plot for all 73 patients who had baseline MMSE testing and then after 1-year of lecanemab infusions. Supplemental Figure 2 highlights a spaghetti plot for the patients who developed ARIA and who had baseline MMSE testing and after 1-year of infusions.
Of the 21 patients who underwent more than 40 infusions (a minimum of 18 months), 16 had MMSE scores performed at baseline and after 1-year post-lecanemab (Supplemental Figure 3). Of these 16 patients, 12 had decreased MMSE scores, 3 had increased scores, and the score remained in the same in 1 patient. One patient’s MMSE score increased by 4 from a baseline score of 20 to a subsequent score of 24 after 16 months of lecanemab infusions. The patient was 59 years old when he initiated lecanemab, had undergone 41 infusions, was a ε4 non-carrier, and had no evidence of ARIA or other adverse side effects of the drug.
Discussion
4
Data presented
4.1
Recent studies have reported the benefits of lecanemab while warning of the potential risks of ARIA, especially in patients who are ε4 homozygous [17,18]. Paczynski and colleagues reported 234 patients treated with lecanemab in a specialty memory clinic over 14 months [18]. Of the 194 patients who underwent at least one surveillance brain MRI, 42 (22 %) developed ARIA, 11 (26.2 %) of whom were symptomatic. In Bregman and colleagues’ study of 86 patients treated with lecanemab in a Cognitive Neurology Unit in a tertiary hospital setting, 16 (18.6 %) patients developed ARIA, most of whom were asymptomatic [17]. Bregman et al. excluded patients homozygous for APOE ε4 and, therefore, rates of ARIA would be expected to be lower overall. Our study concurs with these studies, reflected by 20 % of patients who had ARIA detected on surveillance brain MRIs, half of whom were ε4 homozygous and 30 % of whom were ε4 heterozygous. Five patients were symptomatic when ARIA was identified, resulting in a suspension of lecanemab. Three of these symptomatic patients were ε4 homozygous, and two were ε4 heterozygous. ARIA was most commonly detected on the surveillance brain MRI performed before the 5^th^ infusion (29 [74.4 %] patients). These findings confirm the relatively high risk of ARIA in patients treated with lecanemab, especially in those who are ε4 homozygous or heterozygous. These particular APOE ε4 statuses also portend a higher likelihood of symptomatic ARIA and discontinuing lecanemab due to ARIA progression. It is important to discuss the risks and benefits of starting lecanemab with patients and their families, especially in those who are ε4 homozygous. Unlike Paczynski and colleagues’ study, our study did not demonstrate a relationship between the MCI/mild dementia diagnosis and the lowest quartile of baseline MMSE scores with the development of ARIA. However, both of our studies reported that isolated ARIA-H was more frequent in patients with higher numbers of microbleeds on baseline brain MRI. In our study, patients with more baseline microbleeds more frequently developed any ARIA (ARIA-H and ARIA-E) and solitary ARIA-H. The presence of baseline microbleeds was also associated with a higher frequency of solitary ARIA-H. Of the 73 patients who underwent MMSE testing prior to starting lecanemab and after the 1-year mark in our study, 51 (69.9 %) had decreased MMSE scores, 13 (17.8 %) had increased MMSE scores, and 9 (12.3 %) had the same score.
In Paczynski et al.’s study, 87 (37 %) patients experienced infusion-related reactions, with 92 % occurring following the first or second infusion [18]. These reactions were rated as mild (67 %) or moderate (28 %). Their treatment protocol was changed after observing the high number of infusion-related reactions. Patients were subsequently pre-treated with loratadine and acetaminophen before the initial infusion. In Bregman and colleagues’ study, 19 (22.1 %) patients experienced mild and transient infusion-related reactions [17]. The number, severity, and timing of infusion-related side effects in our study is comparable to these studies. Sixty (32.1 %) patients experienced infusion-related adverse effects, 54 (90.0 %) of which occurred after the first lecanemab infusion and half of which were mild and transient headaches. Over 90 % of the side effects were reported at the infusion center or within 24 h post-infusion.
In Paczynski et al.’s study, 23 (9.8 %) patients discontinued lecanemab, 10 [43.5 %] for ARIA [18]. Bregman et al. reported that 17 (19.8 %) patients withdrew from treatment, with 5 [29.4 %] attributing ARIA as the reason [17]. A total of 32 (17.1 %) patients had discontinued lecanemab at the 2-year mark in our study, with 9 [28.1 %] ending their treatment due to ARIA progression.
Continued challenges with lecanemab at our Memory Center
4.2
We previously described the numerous insurance coverage challenges [13], and these hurdles have persisted (Table 5). The main obstacles are the initial approval and re-authorization of lecanemab by insurance companies, with different requirements for various Medicare options and commercial insurance. Original Medicare approves lecanemab for one year, while Medicare Advantage and commercial insurance plans approve this drug for 6 months. The authorization team at our Memory Center automatically submits the lecanemab re-approval request to insurance companies. Several patients have missed their scheduled infusions since the re-authorizations have not been approved in a timely manner. Some insurance companies require documentation that a patient is tolerating lecanemab well and is benefiting from this medication. These companies also necessitate a statement that the patient has had no evidence of moderate or severe ARIA on surveillance brain MRIs and that the patient has no clinical presentations suggesting ARIA.Table 5. Key insights gained from our two-year experience with lecanemab.Table 5 dummy alt textChallenges with lecanemabKey insightsInitial approval and re-authorization of lecanemab by insurance companiesImportance of shared decision-making progress between patient, caregiver, and provider to initiate lecanemab infusionBrain MRI scheduling concerns due to many patients who require brain imagingProviders offer anti-amyloid therapy early in the evaluation processSome patients do not want to transition to lecanemab maintenance every 4 weeks instead of every 2 weeks after 18 months of lecanemab infusionsPre-infusion oral cocktail (acetaminophen 650 mg, loratadine 10 mg, and famotidine 20 mg) decreased infusion-related adverse eventsReduced post-infusion observation time is possible without safety concerns
We also continue to experience issues with MRI scheduling due to many patients who require brain imaging and challenges with MRI scan capacity. To overcome this obstacle, we instituted a new MRI software program Deep Resolve (Siemens Healthineers; Malvern, PA) in January 2025 that increased the speed of each brain MRI scan by 70 % [19]. Adopting this new program has lessened the MRI workload and has permitted a greater number of scans to be performed.
Key insights gained from our two-year experience with lecanemab
4.3
Through our 2-year experience with lecanemab, we emphasize the importance of a shared decision making process between the patient, caregiver, and provider to initiate lecanemab infusion (Table 5). Patients and their caregivers are thoughtful and well-informed in the decision-making process, as they weigh the risks of lecanemab versus the frequency of infusions. Our Memory Center’s comfort level with treating patients with lecanemab has increased over the 2-year duration. This enhanced confidence has allowed us to lighten the patient restrictions as set forth in the lecanemab Appropriate Use Recommendations [2]. Patients who were previously excluded from using lecanemab due to a lifetime history of seizures and using other monoclonal antibodies such as denosumab are now potentially able to receive lecanemab through a shared decision-making process between the individual treating clinician and patient.
This theme of individualized decisions has been reported in association with lecanemab [20,21]. Parks and colleagues performed a qualitative study of 22 patients with AD highlighting how patients balance the risks and benefits of lecanemab [21]. Numerous considerations were contemplated prior to initiating lecanemab, including individual characteristics, family factors, trust in the provider, insurance coverage, and corresponding with patients who are receiving lecanemab. In Parks et al.’s qualitative study of 27 clinicians who prescribe lecanemab across seven medical centers, the techniques of how clinicians describe the risks and benefits of lecanemab vary, with most focusing on patient comorbidities, eligibility criteria fit, and degree of social support or family involvement in making decisions [20]. Few clinicians use patients’ goals to guide the conversation, and some may not recommend lecanemab and even may advise against it [20].
Our Memory Center providers try to offer anti-amyloid therapy as a possible treatment option early in the evaluation process among appropriate candidates so that the patients and their caregivers have adequate time to make an informed decision. The patient’s first appointment consists of a detailed history, physical exam, cognitive testing (typically MMSE or MOCA), blood work (CBC, CMP, vitamin B12, and TSH), screening for additional nutritional deficiencies, and a brain MRI. Patients undergo formal neuropsychology testing on a case by case basis. CSF studies, blood-based biomarkers, or amyloid PET studies are then performed to confirm AD pathology. Patients subsequently undergo APOE genotyping and continue to discuss the possible benefits and risks of anti-amyloid medications to help them make an informed decision.
At 18 months of lecanemab infusions, patients have the option of transitioning to lecanemab maintenance every 4 weeks. In our Memory Center, five patients started the monthly lecanemab maintenance after 18 months of biweekly infusions and then requested to revert to every 2 week infusions. These patients and their families attributed subjective cognitive decline for their reason to resume the infusions every 2 weeks. Two additional patients did not want to switch to the monthly maintenance and continued on the every 2-week regimen. While we are unable to explain why patients experience subjective cognitive decline with lecanemab administered every 4 weeks compared to every 2 weeks, we posit that patients may thrive on the socialization by coming to the infusion center where they receive encouragement in a positive environment. In our experience, no insurance companies have denied covering the biweekly infusions after 18 months.
In our initial lecanemab publication, 26 (37 %) patients experienced infusion-related side effects after their first lecanemab infusion, primarily headaches and shaking/chills/rigors [13]. Twenty-three (88 %) of these 26 patients reported the side effects either at the infusion center [0–3 h] (10 patients) or between 3–24 h post-infusion (13 patients). The side effects following the first lecanemab infusion mainly occurred in the first 3 months of prescribing lecanemab at our Memory Center. Similar to Paczynski and colleagues, we implemented a pre-infusion cocktail on December 31, 2023 which subsequently plummeted the number of post-infusion side effects. The primary difference between our protocol and theirs is that they pre-treat patients only for the initial infusion, while we pre-treat patients prior to every lecanemab infusion. As we continued to observe a decline in side effects following lecanemab, we revised the duration of post-infusion observation in August 2025. We reduced the observation period after the 1^st^ infusion from 3 to 2 h, after the 2^nd^ infusion from 2 h to 1 h, and all subsequent monitoring periods to 30 min.
Strengths and limitations of the current study
4.4
The strength of the present study is the large number of patients with MCI or mild dementia who were treated with lecanemab in a regional community medical center over a 2-year duration. We have incorporated the lessons learned from our initial experience with lecanemab in the first 6 months and expanded upon our knowledge in the subsequent 18 months. We continue to face similar challenges with insurance and brain MRI scheduling, however, we have implemented measures to mitigate these obstacles. With the imminent implementation of subcutaneous lecanemab infusions at our Memory Center, the care of patients with MCI and mild dementia will be transformed.
The limitations of the current study are its retrospective nature and variability of the reports among the radiologists who reviewed the baseline and surveillance brain MRIs. Our Memory Center has recently employed the use of machine learning capabilities that assist the radiologists in detecting ARIA on the baseline and surveillance brain MRIs which will expedite and standardize methods of quantitatively determining the presence and extent of ARIA. Another limitation is that not all patients underwent MMSE testing prior to starting lecanemab to permit a comparison between scores at baseline and after treatment. It is interesting to note that 30 % of patients who underwent MMSE testing prior to starting lecanemab and between the 1 and 2 year mark had either increased MMSE scores or had the same score.
In conclusion, the main aim of the present study was to define our experience with lecanemab with key insights and to document the incidence of ARIA detected on surveillance brain MRIs over a two-year period. We also wanted to determine how many patients discontinued lecanemab and their particular reasons. Our findings suggest that ARIA is a significant concern especially in patients who are ε4 homozygous. Comprehensive discussions among the patient, caregiver, and provider are valuable in deciding whether lecanemab is an appropriate and beneficial drug.
Funding
The authors declare that there was no funding for their study.
Declaration of generative AI and AI-assisted technologies in the writing process
AI has not been used at all in the preparation of this manuscript.
Data statement
All data supporting the findings of this study are available within the paper.
CRediT authorship contribution statement
Lisa B.E. Shields: Writing – review & editing, Writing – original draft, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Hust Hannah: Writing – review & editing, Software, Resources, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Gregory E. Cooper: Writing – review & editing, Supervision, Project administration, Investigation, Formal analysis, Data curation, Conceptualization. Theresa Kluthe: Writing – review & editing, Visualization, Validation, Software, Resources, Methodology, Investigation, Formal analysis, Data curation. Rachel N. Hart: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Andrew P. Thaliath: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Brandon C. Dennis: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Stephanie W. Freeman: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Jessica F. Cain: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Whoy Y. Shang: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Kendall M. Wasz: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Adam T. Orr: Writing – review & editing, Visualization, Validation, Software, Resources, Investigation, Formal analysis, Data curation, Conceptualization. Christopher B. Shields: Writing – review & editing, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization. Shirish S. Barve: Writing – review & editing, Investigation, Formal analysis, Data curation, Conceptualization. Kenneth G. Pugh: Writing – review & editing, Visualization, Validation, Supervision, Software, Resources, Project administration, Methodology, Investigation, Formal analysis, Data curation, Conceptualization.
Declaration of competing interest
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Gregory E. Cooper, MD, PhD receives research funding from Eisai, Lilly, Novartis, and Davos Alzheimer’s Collaborative. Rachel N. Hart, DO is on the Speaker’s Bureau of Lilly. The rest of the authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Alzheimer's Association 2025 Alzheimer's disease facts and figures Accessed December 15https://www.alz.org 2025 Accessed December 15
- 2Cummings J.Apostolova L.Rabinovici G.D.Atri A.Aisen P.Greenberg S.Lecanemab: appropriate use recommendations J Prev Alzheimers Dis 1020233623773735727610.14283/jpad.2023.30PMC 10313141 · doi ↗ · pubmed ↗
- 3Stewart J.Leqembi FDA approval history Accessed December 15https://www.drugs.com/history/leqembi.html 2025 Accessed December 15
- 4van Dyck C.H.Swanson C.J.Aisen P.Bateman R.J.Chen C.Gee M.Lecanemab in early Alzheimer's disease N Engl J Med 38820239213644941310.1056/NEJ Moa 2212948 · doi ↗ · pubmed ↗
- 5Ashmawy R.E.Okesanya O.J.Ukoaka B.M.Daniel F.M.Ezedigwe S.G.Agboola A.O.Exploring the efficacy and safety of lecanemab in the management of early Alzheimer's disease: a systematic review of clinical evidence J Alzheimers Dis 10520257147284023225810.1177/13872877251331640 · doi ↗ · pubmed ↗
- 6Honig L.S.Sabbagh M.N.van Dyck C.H.Sperling R.A.Hersch S.Matta A.Updated safety results from phase 3 lecanemab study in early Alzheimer's disease Alzheimers Res Ther 1620241053873049610.1186/s 13195-024-01441-8PMC 11084061 · doi ↗ · pubmed ↗
- 7Hossain M.F.Husna A.U.Kharel M.Use of lecanemab for the treatment of Alzheimer's disease: a systematic review Brain Behav 142024 e 35923886746010.1002/brb 3.3592 PMC 11169267 · doi ↗ · pubmed ↗
- 8Mc Dade E.Cummings J.L.Dhadda S.Swanson C.J.Reyderman L.Kanekiyo M.Lecanemab in patients with early Alzheimer's disease: detailed results on biomarker, cognitive, and clinical effects from the randomized and open-label extension of the phase 2 proof-of-concept study Alzheimers Res Ther 1420221913654418410.1186/s 13195-022-01124-2PMC 9768996 · doi ↗ · pubmed ↗