Arterial bleeding during endoscopic ultrasound-guided pancreatic pseudocyst drainage using a novel ultrasound processor
Junya Sato, Kazunari Nakahara, Yosuke Igarashi, Yusuke Satta, Akihiro Sekine, Yu Matsuda, Keisuke Tateishi

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
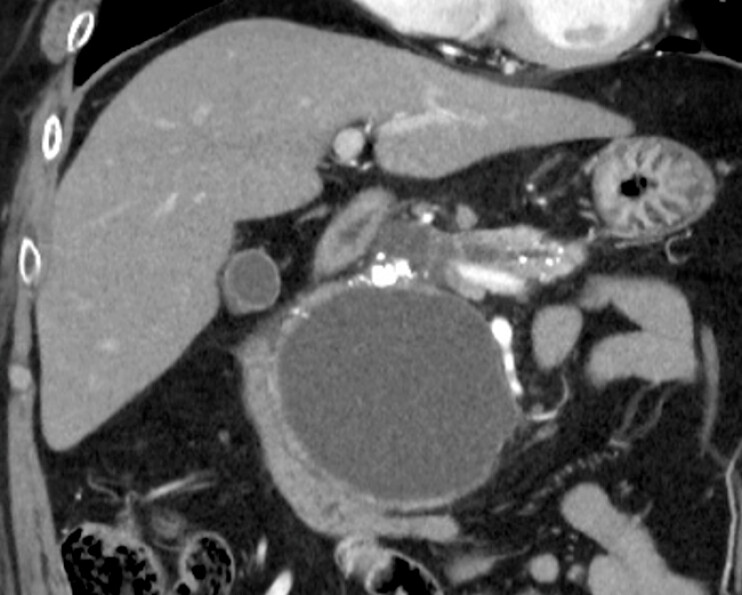 Fig. 1
Fig. 1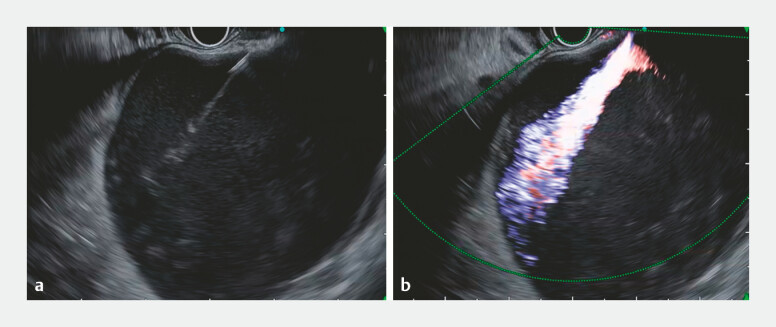 Fig. 2
Fig. 2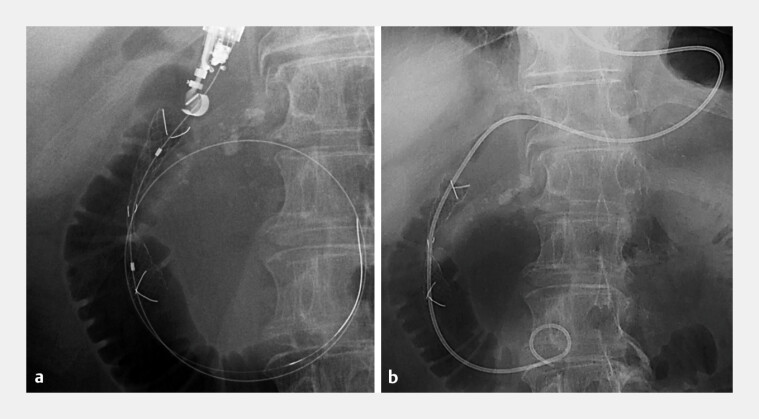 Fig. 3
Fig. 3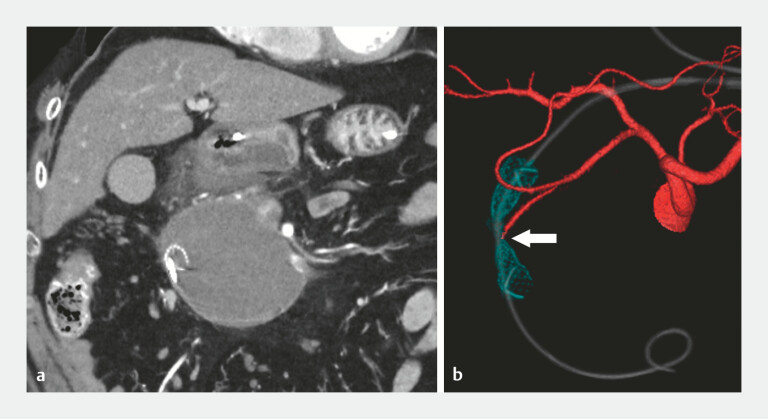 Fig. 4
Fig. 4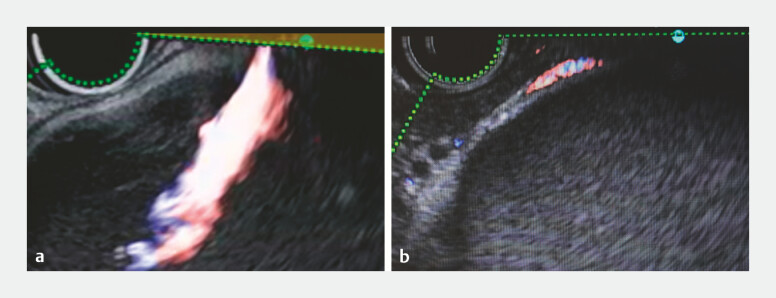 Fig. 5
Fig. 5- —JSPS KAKENHI
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPancreatitis Pathology and Treatment · Gallbladder and Bile Duct Disorders · Pancreatic and Hepatic Oncology Research
Bleeding during endoscopic ultrasound-guided pancreatic pseudocyst drainage (EUS-PPD) is most often associated with electrocautery puncture or tract dilation 1 2 3 4 5 . Conversely, bleeding caused solely by fine-needle puncture is rare. We report a case of arterial bleeding induced by fine-needle puncture performed using a novel ultrasound processor ( Video 1 ).
Arterial bleeding induced by fine-needle puncture performed using a novel ultrasound processor, followed by endoscopic hemostasis.Video 1
A 61-year-old man with a 9-cm pseudocyst in the pancreatic head underwent EUS-PPD ( Fig. 1 ). After Doppler evaluation confirmed no intervening vessels, the pseudocyst was punctured from the duodenum with a 22-gauge needle (EZ Shot 3 Plus, Olympus) under the guidance of a novel ultrasound processor (EU-ME3, Olympus, Japan) and an ultrasound endoscope (GF-UCT260, Olympus). We inserted a 0.018-inch guidewire and subsequently removed the needle. We then immediately observed marked arterial spurting into the cyst cavity on gray-scale imaging ( Fig. 2 a ). Color Doppler confirmed pulsatile flow from the puncture site into the cyst cavity ( Fig. 2 b ). Despite inserting a 7-Fr dilator (ES Dilator, Zeon Medical Co., Japan) for compression hemostasis, bleeding recurred upon its withdrawal. Therefore, a 10-mm fully covered self-expandable metal stent (FCSEMS; HILZO biliary stent, ABIS Inc., Japan) was deployed across the EUS-guided created route, resulting in complete hemostasis. Then, a nasal catheter was placed through the FCSEMS ( Fig. 3 ). Postprocedural computed tomography showed no extravasation; however, injury to the posterior superior pancreaticoduodenal artery was suspected ( Fig. 4 ). The patient experienced no further bleeding, and 1 month later, the FCSEMS was removed without complications.
Computed tomography showing a 9-cm pseudocyst in the pancreatic head.
a Gray-scale ultrasound showing marked arterial spurting from the puncture site into the cyst cavity immediately after the withdrawal of the needle. b Color Doppler imaging confirming the presence of pulsatile arterial flow.
a Placement of a fully covered self-expandable metal stent deployed across the bleeding site resulting in complete hemostasis. b A nasal catheter inserted through the stent.
a Postprocedural computed tomography (CT) showing no extravasation. b The reconstructed CT image suggesting injury to the posterior superior pancreaticoduodenal artery (arrow).
This case highlights the possibility of bleeding during EUS-PPD even when Doppler imaging reveals no visible vessels and a thin needle is used. Compared with its predecessor (EU-ME2 model), the EU-ME3 processor detected certain small areas near the gastrointestinal wall lacking blood-flow signals ( Fig. 5 ). Thus, caution must be exercised to avoid inadvertent vessel injury near the gastrointestinal wall.
Color Doppler imaging comparison between the ( a ) EU-ME3 and ( b ) EU-ME2 ultrasound processors. The EU-ME3 processor displays a slightly reduced color Doppler imaging area (yellow highlight) near the gastrointestinal wall compared with the EU-ME2.
Endoscopy_UCTN_Code_CPL_1AL_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Itoi T Itokawa F Sofuni A Late bleeding after EUS-guided transjejunal drainage of a pancreatic pseudocyst in a Roux-en-Y patient Dig Endosc 201123515310.1111/j.1443-1661.2011.01141.x 21535202 · doi ↗ · pubmed ↗
- 2Iwashita T Lee JG Nakai Y Successful management of arterial bleeding complicating endoscopic ultrasound-guided cystogastrostomy using a covered metallic stent Endoscopy 201244 E 370E 37110.1055/s-0032-131006723012027 · doi ↗ · pubmed ↗
- 3Săftoiu A Ciobanu L Seicean A Arterial bleeding during EUS-guided pseudocyst drainage stopped by placement of a covered self-expandable metal stent BMC Gastroenterol 2013139323706101 10.1186/1471-230X-13-93PMC 3665445 · doi ↗ · pubmed ↗
- 4Matsumori T Katanuma A Maguchi HA case of delayed bleeding 9 days after endoscopic ultrasound-guided pancreatic pseudocyst drainage Endoscopy 201446 E 245E 24610.1055/s-0034-136488124853440 · doi ↗ · pubmed ↗
- 5Li Y Zhang L Yu T Endoscopic management of bleeding after endoscopic ultrasound-guided drainage of a pancreatic pseudocyst Endoscopy 202355 E 310E 31110.1055/a-1981-225836513109 PMC 9833937 · doi ↗ · pubmed ↗