Diagnostic Utility of Laparoscopy in Breast Cancer-Associated Carcinomatous Peritonitis With Suspected Advanced Ovarian Cancer
Toshiya Nishimura, Hideaki Tsuyoshi, Fumikata Hara, Makoto Orisaka, Sayaka Fujiwara

TL;DR
This case study shows how laparoscopy helped diagnose breast cancer in a patient suspected of having ovarian cancer, emphasizing its value in challenging diagnostic scenarios.
Contribution
Demonstrates the diagnostic utility of laparoscopy in identifying breast cancer as the source of carcinomatous peritonitis when imaging is inconclusive.
Findings
Diagnostic laparoscopy revealed peritoneal dissemination in a patient suspected of ovarian cancer.
Histopathology confirmed metastatic breast cancer despite no detectable primary lesion.
Laparoscopy is a minimally invasive and effective tool for diagnosing carcinomatous peritonitis.
Abstract
Carcinomatous peritonitis (CP) secondary to breast cancer is an uncommon metastatic manifestation that presents considerable diagnostic challenges, particularly when the primary lesion is not detectable through imaging modalities. This report examines the case of a 54-year-old female patient who presented with abdominal pain and constipation. Initial preoperative imaging and tumor marker analysis suggested gynecological malignancy, with a strong suspicion of ovarian cancer; however, no definitive primary tumors were identified. Subsequent diagnostic laparoscopy revealed peritoneal dissemination, and histopathological examination confirmed metastatic breast cancer via immunohistochemical staining. This case highlights the essential role of laparoscopy in obtaining a pathological diagnosis even when gynecological cancer is suspected. Laparoscopy is a minimally invasive and highly…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
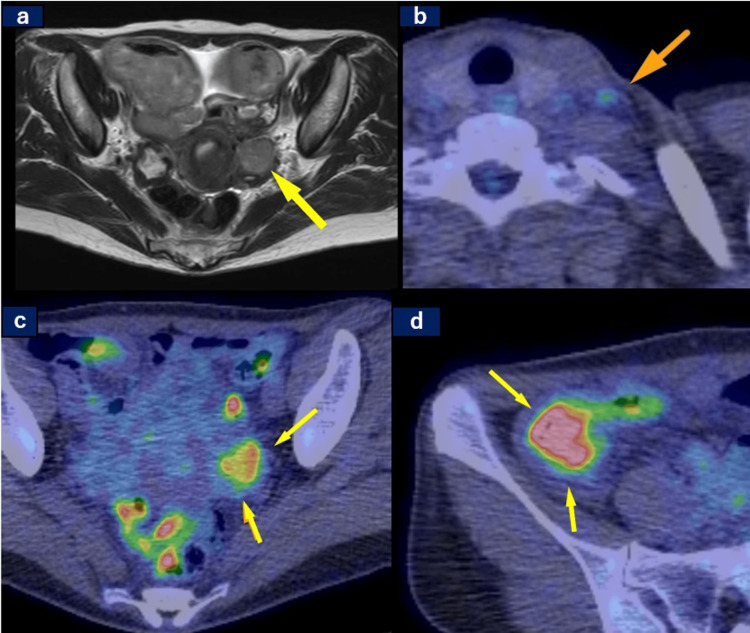 Figure 1
Figure 1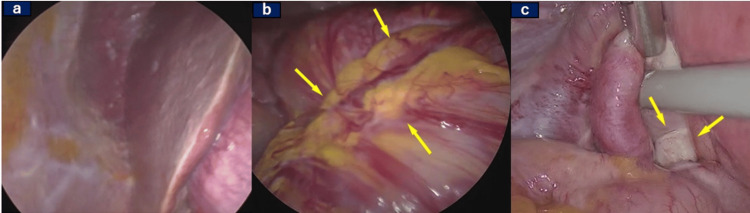 Figure 2
Figure 2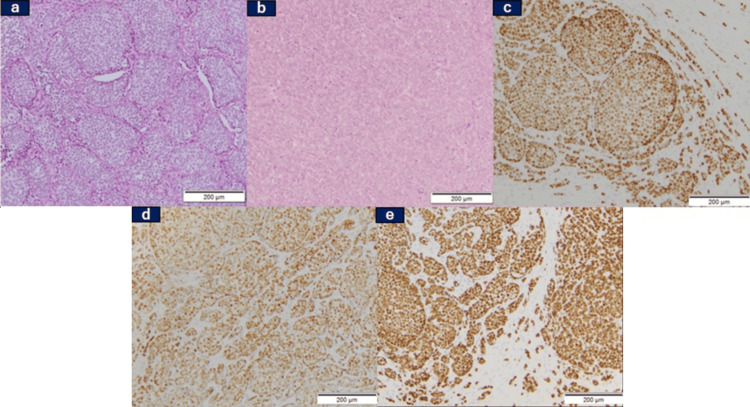 Figure 3
Figure 3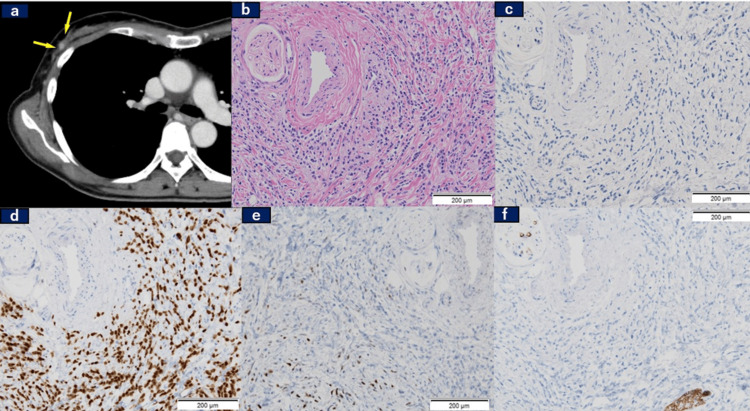 Figure 4
Figure 4| Items | Result | Under limit | Upper limit | Unit |
| WBC | 8340 | 3500 | 9000 | /μL |
| CRP | 0.47 | 0.00 | 0.50 | mg/dL |
| Hb | 13.0 | 12.0 | 16.0 | g/dL |
| PLT | 30.3 | 10.0 | 40.0 | x 104/μL |
| Na | 136.4 | 136.0 | 145.0 | mEq/L |
| K | 4.2 | 3.2 | 5.1 | mEq/L |
| Cl | 102.4 | 98.0 | 108.0 | mEq/L |
| BUN | 12.6 | 8.0 | 22.0 | mg/dL |
| Cre | 0.65 | 0.40 | 0.80 | mg/dL |
| AST | 14 | 8 | 38 | IU/L |
| ALT | 12 | 4 | 35 | IU/L |
| LDH | 174 | 119 | 229 | IU/L |
| CEA | 3.1 | 0.0 | 5.0 | ng/mL |
| CA19-9 | 10 | 0.0 | 37.0 | U/mL |
| CA125 | 25.4 | 0.0 | 35.0 | U/mL |
| Study (Citation) | Year | Age | Initial/Recurrence | Symptoms | Preoperative Imaging | Tumor Marker (U/mL) | Preoperative Diagnosis of Carcinomatous Peritonitis | Postoperative Diagnosis: Pathological Diagnosis and Subtype (Histological) | Detection of Tumor from the Primary Site (Breast) | Procedure to Confirm the Diagnosis of Peritoneal Dissemination | Outcomes |
|
Yoshino et al. [ | 2024 | 59 | Recurrence | Abdominal distension and ascites effusion | The CT scan showed significant ascites accumulation. There was a partial bowel obstruction. | Not specified | Breast cancer | Same diagnosed from the cell block, we only know it is adenocarcinoma. ER(+), PgR(+), and Her2(−). | Yes (performed total mastectomy before 23 years) | Ascites puncture | DOD (61 months) |
|
Franceschini et al. [ | 2006 | 67 | Recurrence | Abdominal pain associated with constipation, tenesmus, and rectal bleeding | The CT scan showed the pelvic cavity almost completely occupied by neoplastic tissue. | Not specified | Breast cancer | Same invasive lobular carcinoma ER(+), PgR(+), and Her2:NA | Yes | Biopsies taken during rectosigmoidoscopy | AWD (duration not reported) |
|
Nakagawa et al. [ | 2020 | 68 | Recurrence | No symptoms | FDG accumulation was found in the pelvic peritoneum. | CA15-3: 230 | Breast cancer | Same invasive ductal carcinoma (papillotubular carcinoma), ER(+), PgR(+), and Her2(−) | Yes | Diagnostic laparoscopy | AWD (duration not reported, chemotherapy was effective) |
|
Mitsuyoshi et al. [ | 2023 | 48 | Initial | A hard mass of 30 mm in size was palpated in area A of the right breast. | FDG accumulation was found in the right breast and pelvic peritoneum. | Not specified | Breast cancer and suspicion of umbilical metastasis | Same invasive ductal carcinoma (tubule forming type + scirrhous type), ER(+), PgR(+),and Her2 (-). | Yes | Diagnostic laparoscopy | AWD (5 months) |
|
Osaku et al. [ | 2015 | 69 | Initial | Constipation | CT and PET did not show any apparent masses in the breasts. | Slightly elevated CA15-3 and CA125 | Metastatic disease of any kind | Breast cancer, invasive lobular carcinoma, immunohistochemical findings are NA. | Yes | Diagnostic laparotomy | DOD (48 months) |
|
Saranovic et al. [ | 2011 | 47 | Initial | Abdominal distension, intermittent abdominal pain, and prolonged constipation | CT scan showed peritoneal and omental implants, ascites, and bilateral ovarian cysts. (The breasts are not detailed.) | CA15-3: 66 | Ovarian cancer | Breast cancer invasive lobular carcinoma ER(+), PgR(+), and Her2 (2+) | Yes | Diagnostic laparotomy | AWD(84 months), rectal metastasis diagnosed at 72 months |
|
Egami et al. [ | 2024 | 64 | Initial | Back pain | MRI showed 50 mm multicystic tumor on the right ovary. | CA125: 47.2, CA19-9: 1021, and CEA:29.8 | Ovarian cancer | Seromucinous borderline tumor. The nodule of the round ligament was adenocarcinoma, and immunohistochemical staining was consistent with breast cancer ER(-), PgR(+), and Her2 (2+) | No postoperative breast MRI exhibited any malignant findings | Diagnostic laparoscopy | AWD (17 months after operation, chemotherapy was performed) |
| Our case | 2024 | 54 | Initial | Abdominal pain, ileus of the intestine | CT and PET did not show any apparent masses in the breasts. | CA125: 25.4, CA19-9: 10 | Ovarian cancer | Breast cancer invasive lobular carcinoma ER(+), PgR(+), and Her2:(-) | Yes | Diagnostic laparoscopy | DOD (22months) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntraperitoneal and Appendiceal Malignancies · Ovarian cancer diagnosis and treatment · Multiple and Secondary Primary Cancers
Introduction
Breast cancer is the most prevalent malignant tumor among women worldwide, with approximately 2,300,000 cases reported by 2022. The age-adjusted incidence rate was approximately 46.8 cases per 100,000 people [1]. The most common sites of distant metastasis include the bone, lungs, liver, and brain, whereas carcinomatosis peritonitis (CP) due to peritoneal dissemination is a relatively rare form of metastasis [2,3].
The diagnosis of this condition is based on clinical symptoms, such as ascites and bowel obstruction, tumor markers (such as CA15-3 and CEA), and imaging studies (computed tomography (CT) and fluorodeoxyglucose F18 (FDG)-positron emission tomography (PET)); however, a definitive diagnosis requires pathological examination.
Laparoscopy has recently gained attention as a minimally invasive diagnostic method, contributing to the improved diagnostic accuracy of peritoneal dissemination in gynecological and gastrointestinal malignancies [4,5]. However, there are few reports on the utility of laparoscopy for breast cancer. In the present case, diagnostic laparoscopy was performed because imaging studies suggested CP of the ovarian cancer. Pathological examination of the resected ovary and peritoneum revealed metastasis from the breast cancer. Although CP due to ovarian cancer was initially suspected, diagnostic laparoscopy revealed ovarian and peritoneal metastases from the breast.
This is a rare reported case in which diagnostic laparoscopy led to the identification of breast cancer metastasis to the ovary and peritoneum, followed by subsequent detection of the primary breast lesion during follow-up.
Case presentation
A 54-year-old female patient (gravida 3, para 3) presented with abdominal pain and constipation. Her previous intestinal obstruction had initially raised suspicion of transverse colon cancer; however, colonoscopy revealed no abnormalities. Subsequent CT imaging suggested ovarian enlargement, and the patient was therefore referred to our hospital for further evaluation.
The patient measured 157.1 cm in height and weighed 43.2 kg. There was no family history of hereditary cancer. Upon examination following stent placement, the patient's abdominal pain subsided, and no tenderness was detected.
Laboratory investigations indicated a mildly elevated white blood cell count (WBC) of 8340/μL and a C-reactive protein (CRP) level of 0.47 mg/dL. Serum tumor markers, including carcinoembryonic antigen (CEA) at 3.1 ng/mL, carbohydrate antigen 19-9 (CA19-9) at 10 U/mL, and cancer antigen 125 (CA125) at 25.4 U/mL, were all within normal limits (Table 1).
Contrast-enhanced CT of the chest, abdomen, and pelvis revealed enlarged left supraclavicular lymph nodes, which raised suspicion of metastasis from an unknown primary malignancy. No evidence of pulmonary metastases or pleural effusion was observed, and no apparent masses were detected in the breast. Ascites was present in the abdomen, but no significant abnormalities were identified in the pelvic or abdominal organs. Dilatation and fluid retention were noted in the small intestine, suggesting stenosis due to peritoneal dissemination.
Pelvic magnetic resonance imaging (MRI) revealed enlargement of the left ovary (Figure 1, Panel a). FDG PET revealed FDG uptake in the left ovary (Figure 1, Panel b), cervical lymph nodes (Figure 1, Panel c), and around the transverse colon stent (Figure 1, Panel d). Based on these findings, ovarian cancer with peritoneal dissemination was considered to be the most probable diagnosis. Diagnostic laparoscopy and cervical lymph node biopsy were performed to obtain tissue samples for pathological confirmation.
MRI and PET findings: Initially suggested ovarian cancer and cervical lymph node metastasis(a) Magnetic resonance imaging with T2-weighted images showed a left ovarian tumor (arrow). Positron emission tomography (PET) showed the accumulation of fluorodeoxyglucose F18 (FDG) in (b) cervical lymph nodes (arrow), (c) left ovary (arrow), and (d) around the transverse colon stent (arrow).
Laparoscopic examination revealed miliary-sized peritoneal seeding extending from the subdiaphragm to the Douglas fossa accompanied by ascitic fluid accumulation. The transverse colon exhibited distension due to extensive omental seeding, and the peritoneum surrounding the left ovary was thickened, although no distinct ovarian mass was identified (Figure 2, Panel a). Surgical resection of the omental seeding near the transverse colon (Figure 2, Panel b) and the left adnexa was performed (Figure 2, Panel c).
Findings on laparoscopyLaparoscopy revealed (a) miliary-sized peritoneal seeding from the subdiaphragm, (b) the transverse colon was distended due to extensive omental seeding, and (c) no ovarian mass was detected on the left ovary.
Histopathological analysis identified a poorly differentiated carcinoma, with tumor cells proliferating within the mesenchyme of the left ovary and fallopian tube (Figure 3, Panel a). Cervical lymph node biopsy revealed a histological pattern consistent with peritoneal lesions, indicating metastasis rather than two separate malignant tumors (Figure 3, Panel b). Immunohistochemical (IHC) analysis revealed positivity for estrogen receptor (ER) (Figure 3, Panel c), progesterone receptor (PgR) (Figure 3, Panel d), and GATA-binding protein 3 (GATA3) (Figure 3, Panel e), suggesting metastatic breast cancer.
Pathological findings of specimens by laparoscopic examination(a) Hematoxylin and eosin staining revealed poorly differentiated carcinoma, with tumor cells growing within the mesenchyme of the left ovary and the fallopian tube. (b) Cervical lymph node biopsy showing a histological pattern consistent with the peritoneal lesions. Immunohistochemical staining demonstrated positivity for (c) ER(+), (d) PgR(+), and (e) GATA3(+).ER: Estrogen receptor; PgR: Progesterone receptor; GATA3: GATA-binding protein 3.
A follow-up CT scan conducted 50 days after the initial visit to our department revealed a newly detectable mass in region C of the right mammary gland (Figure 4, Panel a), prompting a biopsy from this site. Hematoxylin and eosin (H&E) staining (Figure 4, Panel b) and IHC staining were performed. HER2 staining yielded an IHC score of 0 according to the ASCO/CAP guideline [6], rendering further evaluation using FISH unnecessary (Figure 4, Panel c). Additionally, staining for ER (Figure 4, Panel d) and PgR (Figure 4, Panel e) was positive, and E-cadherin (Figure 4, Panel f) was negative, indicating invasive lobular carcinoma of the breast.
A mammary tumor finally detected 50 days after the initial visit and the associated pathological findings(a) A small nodule emerged. (b) Hematoxylin and eosin staining of the small nodule. Immunohistochemical staining of the small nodule revealed (c) HER2(-), (d) ER(++), (e) PgR (+), and (f) E-cadherin (-).HER2: Human epidermal growth factor receptor 2; ER: Estrogen receptor; PgR: Progesterone receptor.
This led to a diagnosis of stage IV breast cancer with peritoneal dissemination, ovarian metastasis, and cervical lymph node metastasis. Subsequently, the patient underwent systemic therapy for metastatic breast cancer. Letrozole was initiated three months after the initial visit, followed by combination therapy with letrozole and abemaciclib after four months. After approximately 13 months of stable disease, follow-up CT demonstrated thickening at the proximal lumen of the transverse colon stent and peritoneal thickening, which was judged to indicate worsening peritoneal seeding; therefore, endocrine therapy was considered no longer effective, and capecitabine was introduced 14 months after the initial presentation, taking into account standard chemotherapy options and the patient’s preference for an oral regimen. At 20 months, CT revealed worsening transverse colon wall thickening and peritoneal thickening with increased ascites accumulation, leading to a determination of progressive disease. As the patient declined further cytotoxic anticancer agents due to concerns about physical decline from side effects and the National Cancer Center (NCC) Oncopanel revealed a high tumor mutational burden (TMB-high), treatment was switched to pembrolizumab monotherapy; however, the patient died 22 months after the initial presentation. Informed consent was obtained for the publication of this case report, and patient anonymity was preserved.
Discussion
CP originating from breast cancer represents a relatively uncommon metastatic pattern. Bertozzi et al. reported that peritoneal metastases occurred in approximately 0.7% of all patients with invasive breast cancer, including both ductal and lobular subtypes. In their analysis, invasive lobular carcinoma was identified as an independent risk factor for peritoneal metastasis; however, the overall prevalence of breast cancer-related CP remains low, and its prognosis is generally unfavorable [3]. Distinguishing breast cancer with peritoneal dissemination from gynecological or gastrointestinal malignancies is challenging [7]. Pathological examination is crucial for diagnosing breast cancer-related CP alongside imaging findings and tumor marker evaluation, and the diagnostic challenge is exacerbated when the primary lesion is not identifiable.
Diagnostic laparoscopy is well established as an effective tool for assessing peritoneal dissemination in gastric and pancreatic cancers as well as for staging gynecological malignancies [4,5,7]. It has also been reported to be beneficial for confirming the diagnosis and determining treatment strategies in cases of CP in which the primary tumor cannot be clearly identified. However, reports on diagnostic laparoscopy specifically for breast cancer are exceedingly limited, and evidence of its diagnostic utility in this context remains scarce.
Table 1 summarizes previous reports of breast cancer-derived CP along with the present case. The three cases reported by Yoshino et al. [8], Franceschini et al. [9], and Nakagawa et al. [10] involved patients with a history of breast cancer, and CP was confirmed as a recurrence. The case reported by Mitsuyoshi et al. [11] had no prior history of breast cancer but was diagnosed preoperatively based on physical examination and imaging studies. Reports in which breast cancer was not diagnosed preoperatively were limited to cases by Osaku et al. [12] and Saranovic et al. [13]. Osaku et al. [12] described a case of suspected carcinoma of unknown primary origin, where exploratory laparotomy was performed after endoscopic biopsy of a rectal stricture yielded no abnormal findings, and CP due to breast cancer was confirmed through biopsy of the peritoneal implants. Saranovic et al. [13] reported a patient who presented with abdominal distension preoperatively diagnosed with ovarian cancer based on imaging and underwent laparotomy. Postoperative pathology confirmed peritoneal dissemination originating from the breast cancer. In both reports, the diagnosis of breast cancer was established by further breast examination after laparotomy. Egami et al. [14] similarly reported a case in which ovarian enlargement led to a suspicion of ovarian cancer, and peritoneal dissemination from breast cancer was diagnosed laparoscopically, consistent with our case. However, in their case, peritoneal dissemination was limited to the round ligament, and the ovary was diagnosed as a seromucinous borderline tumor. Moreover, no lesions were identified in the breast, which was considered the primary site, even on postoperative imaging; therefore, breast biopsy was not performed.
The patient was initially diagnosed with ovarian cancer due to FDG uptake in the left ovary and subsequently underwent diagnostic laparoscopy for staging purposes. However, intraoperative tissue analysis unexpectedly revealed the presence of metastatic breast cancer. To our knowledge, this is a rare report in which comprehensive preoperative imaging failed to identify the primary lesion, leading to a strong suspicion of ovarian cancer, and in which diagnostic laparoscopy alone resulted in the definitive diagnosis of ovarian metastasis of breast cancer and breast cancer-related CP. Several challenges are encountered during the diagnostic process. FDG-PET demonstrated significant uptake in the left ovary, consistent with ovarian cancer, yet minimal uptake was observed in the pelvic and para-aortic lymph nodes, while the cervical lymph nodes exhibited uptake first, indicating an atypical metastatic pattern for advanced ovarian cancer. Furthermore, the tumor markers CA125 and CA19-9 were within the normal limits, creating a discrepancy with the imaging findings.
As breast cancer was not considered in the preoperative differential diagnosis, the breast cancer-associated marker CA15-3 was not measured. However, as shown in Table 2, several previous reports have documented elevated CA15-3 levels, suggesting its utility as a supplementary diagnostic marker for breast cancer-related CP.
Conclusions
In cases presenting with atypical findings, such as discrepancies between imaging findings and tumor markers, it may be beneficial to include breast cancer in the differential diagnosis, even in the absence of clear breast lesions. Measuring CA15-3, along with a broader panel of tumor markers, may facilitate earlier consideration of breast cancer as a potential origin.
This case highlights the diagnostic challenges associated with occult primary breast cancers. Even when imaging strongly suggests ovarian cancer, clinicians should exercise caution and expand the differential diagnosis when atypical metastatic patterns or inconsistent test results are encountered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Global patterns and trends in breast cancer incidence and mortality across 185 countries Nat Med Kim J Harper A Mc Cormack V 115411623120253999447510.1038/s 41591-025-03502-3 · doi ↗ · pubmed ↗
- 2Metastatic behavior of breast cancer subtypes J Clin Oncol Kennecke H Yerushalmi R Woods R 327132772820102049839410.1200/JCO.2009.25.9820 · doi ↗ · pubmed ↗
- 3Prevalence, risk factors, and prognosis of peritoneal metastasis from breast cancer Springerplus Bertozzi S Londero AP Cedolini C 688420152657633110.1186/s 40064-015-1449-x PMC 4641144 · doi ↗ · pubmed ↗
- 4The role of staging laparoscopy for gastric cancer patients: current evidence and future perspectives Cancers (Basel) Schena CA Laterza V De Sio D 34251520233744453510.3390/cancers 15133425 PMC 10340245 · doi ↗ · pubmed ↗
- 5Laparoscopy for diagnosing resectability of disease in women with advanced ovarian cancer Cochrane Database Syst Rev van de Vrie R Rutten MJ Asseler JD Leeflang MM Kenter GG Mol BW Buist M 03201910.1002/14651858.CD 009786.pub 3PMC 643217430907434 · doi ↗ · pubmed ↗
- 6Human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists Clinical Practice Guideline focused update J Clin Oncol Wolff AC Hammond ME Allison KH 210521223620182984612210.1200/JCO.2018.77.8738 · doi ↗ · pubmed ↗
- 7Infiltrative pattern of metastatic invasive lobular breast carcinoma in the abdomen: a pictorial review Insights Imaging Wong YM Jagmohan P Goh YG Putti TC Ow SG Thian YL Pillay P 1811220213489429710.1186/s 13244-021-01120-4PMC 8665916 · doi ↗ · pubmed ↗
- 8Breast cancer with biomarker reversal during the course of treatment: a case report J Surg Case Rep Yoshino R Nakatsubo M Ujiie N Kitada M 02024202410.1093/jscr/rjae 432PMC 1121249738947869 · doi ↗ · pubmed ↗