Seizures After Lumbar Laminectomy: A Clinical Case
Neuza Machado, Elisabete Monteiro, Juliana Branquinho, Mafalda Neves, Sofia Mendes

TL;DR
A patient developed seizures after spine surgery due to cerebrospinal fluid hypotension from a dural tear, highlighting the need for prompt repair.
Contribution
This case report highlights a rare complication of incidental durotomy during spine surgery leading to generalized seizures.
Findings
A 71-year-old female developed generalized seizures post-lumbar surgery due to CSF hypotension from an iatrogenic dural tear.
Imaging confirmed a pseudohypoxic cerebral pattern consistent with CSF hypotension.
Early repair of incidental durotomy is recommended to prevent complications from CSF leakage.
Abstract
Incidental durotomy can occur as a complication of spine surgery, potentially resulting in serious intracranial complications. We report a case of a 71-year-old female with significant spinal stenosis from L3-L5 who underwent a posterior lumbar decompression and fusion. In the immediate post-operative period, she developed generalized tonic-clonic seizures. A brain computed tomography scan was urgently performed, showing a slight decrease in the amplitude of the supratentorial ventricular system, associated with engorgement of the venous sinuses, interpeduncular hyperdensity, and thalamic hypodensities (evoking a pseudohypoxic pattern). These changes, taken together, were consistent with the suspicion of cerebrospinal fluid (CSF) hypotension. A brain magnetic resonance image was done, confirming a pseudohypoxic cerebral pattern. This case illustrates CSF hypotension after iatrogenic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1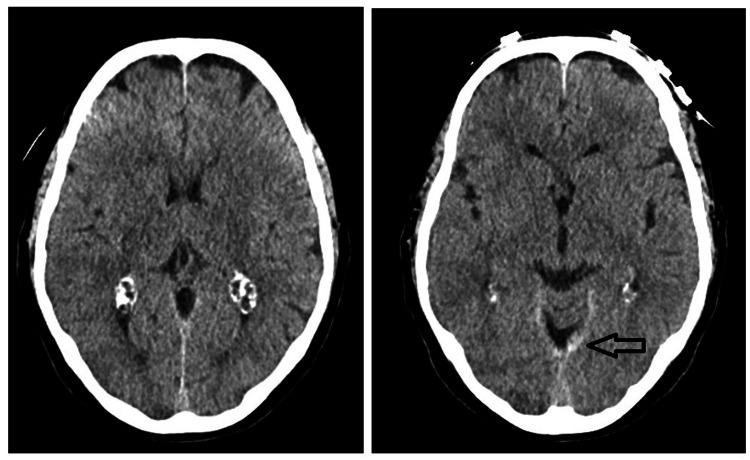 Figure 2
Figure 2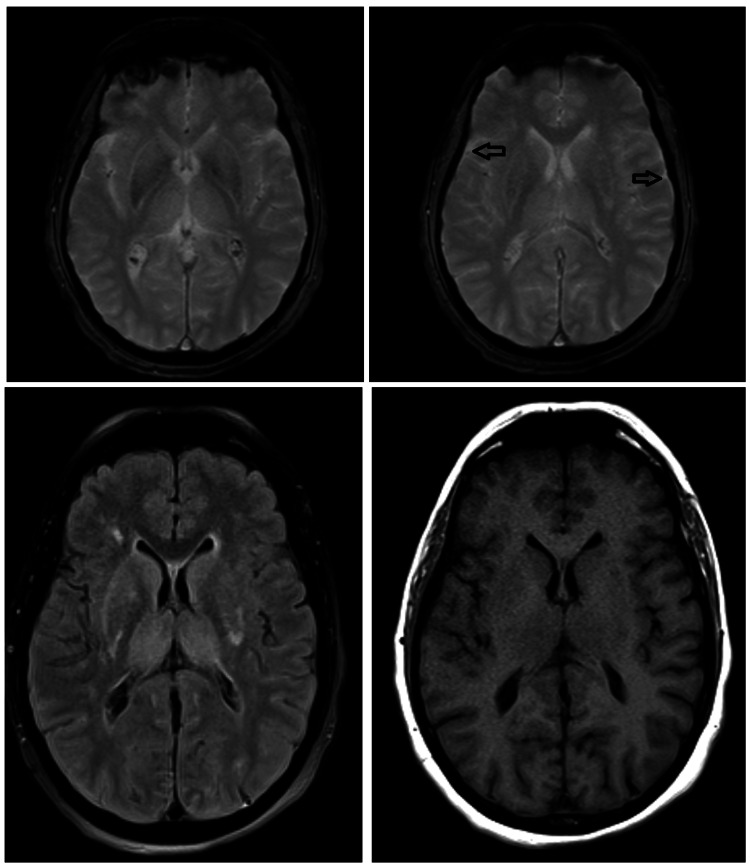 Figure 3
Figure 3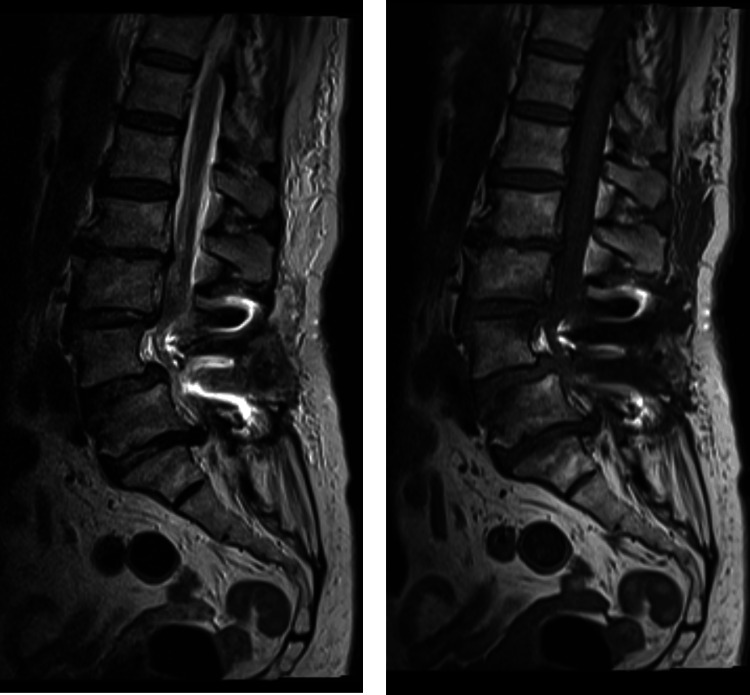 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurosurgical Procedures and Complications · Head and Neck Surgical Oncology · Cerebrospinal fluid and hydrocephalus
Introduction
Spine surgery carries the risk of various complications, such as damage to blood vessels, injury to nerve roots, formation of a hematoma in the epidural space after surgery, infections at the surgical site, spinal cord damage, and tears in the dura mater [1]. Unintentional durotomy with cerebrospinal fluid (CSF) leakage has also been observed following procedures such as lumbar puncture, spinal anesthesia, myelography, and the placement of a lumbar drain [2,3]. Various treatment approaches are available for managing durotomies, including direct primary closure during surgery and the use of fibrin glue, fat grafts, or muscle grafts to aid in sealing the tear [4]. The precise pathophysiology remains unclear, but it is believed that a CSF leak can lead to reduced intracranial pressure and enlargement of the subdural spaces. This may result in downward displacement of the brain, causing stretching of neural structures [5]. We present a case of CSF hypotension following an incidental dural tear during posterior lumbar spinal surgery.
Case presentation
A 71-year-old female presented with lumbar pain, numbness and weakness of both legs. Her past medical history was only remarkable for type 2 diabetes mellitus. No history of hypertension or coagulation disorders was documented. Pre-operative imaging lumbar spine scan showed significant stenosis at the level of L3-L5 (Figure 1). Laboratory blood tests were all within normal limits.
Pre-operative lumbar magnetic resonance imaging
She underwent a posterior lumbar decompression and fusion L3-L5. The anesthetic technique was total intravenous anesthesia. The intra-operative analgesia was paracetamol 1g, metamizole 1g, ketorolac 30mg and morphine 2mg. The procedure was performed in a prone position. The neurosurgeons did not see any signs of intraoperative CSF leak. The surgery was completed and the patient was awoken and extubated. After a few minutes, generalized tonic-clonic seizures occurred. As a result, she was promptly re-intubated and transferred to the Neurocritical Care Unit (NCCU). An urgent brain computed tomography (CT) scan was ordered. It showed a decrease in the amplitude of the supratentorial ventricular system, associated with engorgement of the venous sinuses, interpeduncular hyperdensity and hypodensity in the thalami (evoking a pseudohypoxic pattern) (Figure 2).
Post-operative brain computed tomographyThere is a slight decrease in the amplitude of the supratentorial ventricular system, associated with engorgement of the venous sinuses, interpeduncular hyperdensity, and hypodensity in the thalami (evoking a pseudohypoxic pattern). There is also the appearance of "pseudo-subarachnoid hemorrhage" (arrow).
Different aetiologies were considered, including a dural tear with CSF leak or an anaesthetic complication.
Seizures were managed with sedation (propofol) and antiepileptics (levetiracetam). An electroencephalogram (EEG), performed without sedation, revealed diffuse slowing of brain electrical activity, consistent with moderate encephalopathy, and no apparent epileptic activity.
A wake-up test showed a persistent Glasgow Coma Scale (GCS) of 3 (E1V1M1) [6], and a brain magnetic resonance imaging (MRI) revealed a pseudohypoxic cerebral pattern (Figure 3).
Post-operative brain magnetic resonance imagingChanges consistent with a pseudohypoxic pattern are described in the context of spinal surgical intervention. There was a diffuse thickening and pachymeningeal enhancement (arrows); these findings are compatible with a context of cerebrospinal fluid hypotension.
A lumbar MRI was not able to document liquor leak points (Figure 4).
Post-operative lumbar imagesThe MRI was unable to document liquor leak points.
Intracranial pressure (ICP) was sustained at 2-4 mmHg with the head up to 30º. After several observations, on the sixth day of hospitalization, clear fluid drainages were observed through the lumbar surgical wound. With these drainages, ICP dropped to negative values. She initiated meropenem and vancomycin due to suspected central nervous system infection.
In a multidisciplinary discussion between neurosurgeons and neurointensivists, it was decided to perform a surgical review of the wound. A surgical exploration was performed in the operating room, with identification of one dural laceration and exteriorization of the rootlets adjacent to the right L5 screw. This dural tear was repaired with a dural substitute and biological glue.
On the twelfth day of hospitalization, four days after the second surgery, she was extubated and she presented with a GCS of 14 (E4V4M6) [6]. Her wound healed without signs of infection. A follow-up brain CT scan postoperatively demonstrated no alterations. At NCCU discharge, she was GCS 15 (E4V5M6). Her neurological examination showed improvement of her bilateral leg numbness compared to her pre-operative status, but mild cognitive and motor impairment (global strength 3+) was noted. She underwent physiotherapy and rehabilitation with posterior improvement (global strength 4+).
Discussion
Dural injuries are a relatively uncommon complication of spine surgery, occurring in approximately 4% to 9% of cases [7]. Several causes of CSF leakage due to dural tears during surgery have been identified, including direct trauma to the dura, excessive traction on nerve roots, and improperly placed surgical instruments [8]. Risk factors that may contribute to this complication include advanced age, female sex, previous surgeries leading to scar tissue formation, corrective vertebral osteotomy procedures, degenerative spondylolisthesis, and earlier radiotherapy, which can hinder proper tissue healing [9,10]. In the majority of cases, patients experience a persistent headache caused by the downward shift of the brain, which places tension on the pain-sensitive dural sinuses [11]. In our case, the patient did not present with any preceding symptoms. Instead, she presented with a new-onset, sudden generalized tonic-clonic seizure that occurred immediately after the surgery. Our patient was healthy and had no history of hypertension or previous head, thoracic or lumbar trauma.
Although the exact mechanism is not fully understood, it is believed that a continuous loss of CSF leads to a sustained decrease in ICP. This reduction in pressure causes the brain, which typically floats in CSF, to descend or sag within the skull. As a result, sensitive structures such as the meninges and bridging veins are stretched, which is thought to be the source of symptoms like headache and discomfort [12]. Some researchers also propose that a decrease in CSF pressure can lead to downward displacement of the brain. Under normal conditions, CSF provides buoyancy that helps support the brain’s weight. When CSF pressure drops, this support is reduced, allowing the brain to sag or shift downward, which may result in a range of neurological symptoms. We believe that the cause of our patient was the sudden loss of a significant volume of CSF through the dural tear.
A brain CT scan is essential for diagnosis and should be conducted promptly after the onset of any worrisome symptoms [13]. The scan may reveal downward displacement of the brain and herniation of the cerebellar tonsils, reduced ventricular size, enhancement of the meninges, or enlarged epidural veins [13]. Intracranial hypotension is challenging to confirm definitively using axial head CT scans. Common findings may include narrowing of the basal cisterns that seems disproportionate to any extra-axial fluid collections, collapse of the third ventricle, and widespread brain swelling. However, CT scans rarely provide a conclusive diagnosis. As a result, diagnosing intracranial hypotension relies largely on the patient's clinical history, with additional imaging performed when there is strong clinical suspicion [14]. In our patient, the brain CT scan demonstrated a decrease in the amplitude of the supratentorial ventricular system, associated with engorgement of the venous sinuses, interpeduncular hyperdensity and hypodensity in the thalami (evoking a pseudohypoxic pattern).
Management of a CSF leak can involve conservative, multifaceted approaches such as bed rest, adequate hydration, and pain relief, particularly in cases of mild CSF hypotension without severe symptoms. However, surgical treatment is often necessary for patients experiencing significant CSF loss accompanied by severe neurological deficits [15]. Most reported cases generally follow a benign course and result in good neurological recovery. Although the overall incidence is relatively low, approximately 5 in 100000, it is believed that many cases go undiagnosed [16]. Intracranial hypotension leading to reversible coma has a low mortality rate, with some studies reporting death rates below 10% [17]. Although coma in this situation is a serious complication, it is frequently reversible when treated promptly and appropriately. In the present case, our patient was managed in the NCCU with surgical intervention. At discharge, she was GCS 15 (E4V5M6) [6] and her neurological examination showed mild cognitive and motor impairment (global strength 3+), so she was orientated to physiotherapy and rehabilitation.
Conclusions
CSF hypotension is an uncommon but potentially serious complication that can occur following a CSF leak caused by iatrogenic durotomy during spinal surgery. The appearance of seizures after spine surgery should raise suspicion for postoperative CSF hypotension.
Prompt surgical repair of an incidental durotomy is crucial to minimize CSF leakage. Additionally, a brain CT scan should be performed to confirm the diagnosis and rule out other possible structural causes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Classification and management of early complications in open lumbar microdiscectomy Eur Spine J Kraemer R Wild A Haak H Herdmann J Krauspe R Kraemer J 2392461220031279999810.1007/s 00586-002-0466-y PMC 3615492 · doi ↗ · pubmed ↗
- 2Subdural hematoma following lumbar puncture Arch Intern Med Gaucher DJ Jr Perez JA Jr 1904190516220021219609110.1001/archinte.162.16.1904 · doi ↗ · pubmed ↗
- 3Subdural hematoma after thoracoabdominal aortic aneurysm repair: an underreported complication of spinal fluid drainage?J Vasc Surg Dardik A Perler BA Roseborough GS Williams GM 47503620021209625610.1067/mva.2002.125022 · doi ↗ · pubmed ↗
- 4Collagen matrix (Dura Gen) in dural repair: analysis of a new modified technique Spine (Phila Pa 1976) Narotam PK JoséS Nathoo N Taylon C Vora Y 286128672920041559929110.1097/01.brs.0000148049.69541.ad · doi ↗ · pubmed ↗
- 5Acute intracranial subdural hematoma following a lumbar CSF leak caused by spine surgery Spine (Phila Pa 1976) Sciubba DM Kretzer RM Wang PP 030200510.1097/01.brs.0000192208.66360.2916371890 · doi ↗ · pubmed ↗
- 6Assessment of coma and impaired consciousness: a practical scale Lancet Teasdale G Jennett B 8184304197410.1016/s 0140-6736(74)91639-04136544 · doi ↗ · pubmed ↗
- 7Long-term results of lumbar spine surgery complicated by unintended incidental durotomy Spine (Phila Pa 1976) Jones AA Stambough JL Balderston RA Rothman RH Booth RE Jr 443446141989271804910.1097/00007632-198904000-00021 · doi ↗ · pubmed ↗
- 8Evaluation and treatment of dural tears in lumbar spine surgery: a review Clin Orthop Relat Res Bosacco SJ Gardner MJ Guille JT 238247389200110.1097/00003086-200108000-0003311501817 · doi ↗ · pubmed ↗