The impact of expanded access to antiretroviral treatment on engagement in HIV care and viral suppression among pregnant women living with HIV in South Africa
Cornelius Nattey, Mhairi Maskew, Nelly Jinga, Laura Rossouw, Amy Wise, Nicola van Dongen, Thalia Ferreira Brizido, Maanda Mudau, Karl-Günter Technau, Kate Clouse

TL;DR
This study examines how expanded access to HIV treatment in South Africa affected care engagement and virus control in pregnant women with HIV.
Contribution
The study evaluates the impact of Option B+ and Universal Test and Treat policies on HIV care engagement and viral suppression in pregnant women.
Findings
Engagement in HIV care before pregnancy increased during the Option B+ and UTT eras compared to earlier periods.
Younger women and those with low CD4 counts were less likely to engage in HIV care prior to pregnancy.
Viral suppression was higher among women who used ART before pregnancy compared to those without prior care.
Abstract
Timing of engagement in HIV care in relation to pregnancy impacts maternal outcomes and the risk of vertical transmission of HIV. Option B+, a policy that mandates offering all pregnant women living with HIV (PWLH) lifelong antiretroviral therapy (ART) irrespective of their CD4 count, has been adopted across sub-Saharan Africa, including South Africa since 2015. This study aimed to assess the impact of expanded access to ART on engagement in HIV care and viral suppression among pregnant women in South Africa. This observational study used data from pregnant women living with HIV who delivered at Rahima Moosa Mother and Child Hospital in Johannesburg, South Africa from 2013−2017. Linkage to a national HIV laboratory cohort (the NHLS National HIV cohort) was used to ascertain engagement in HIV care prior to antenatal care (ANC) entry and viral load outcomes. Analyses were stratified by…
Click any figure to enlarge with its caption.
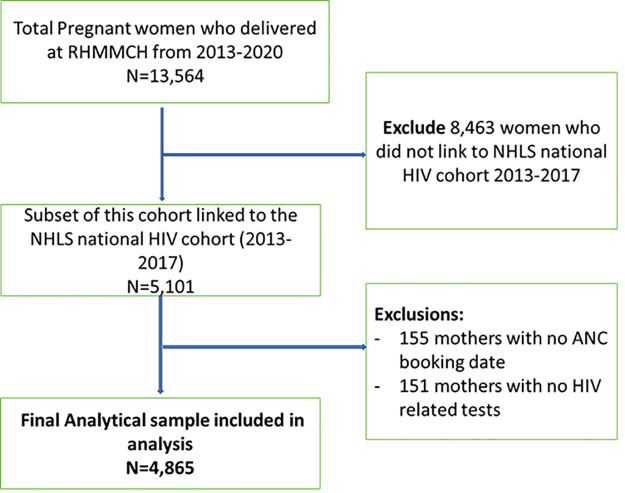 Fig 1
Fig 1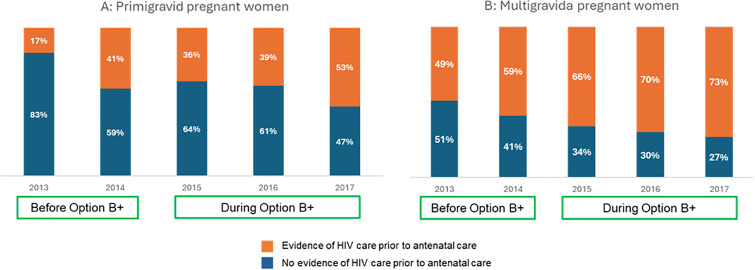 Fig 2
Fig 2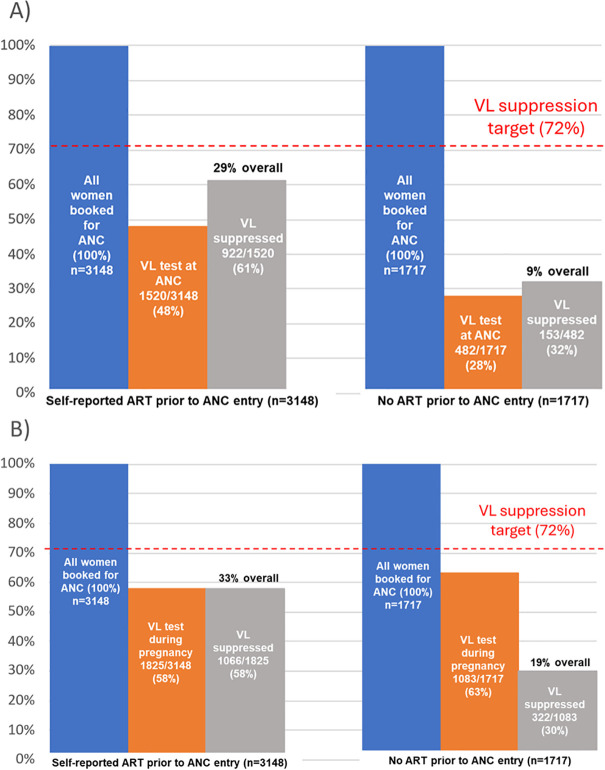 Fig 3
Fig 3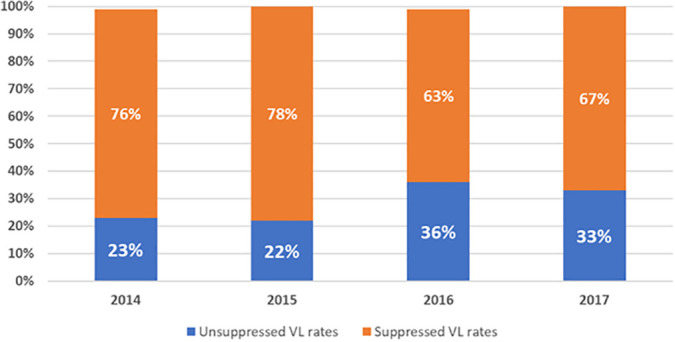 Fig 4
Fig 4- —http://dx.doi.org/10.13039/100000071National Institute of Child Health and Human Development
- —http://dx.doi.org/10.13039/100000071National Institute of Child Health and Human Development
- —http://dx.doi.org/10.13039/100000071National Institute of Child Health and Human Development
- —http://dx.doi.org/10.13039/100006492Division of Intramural Research, National Institute of Allergy and Infectious Diseases
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHIV/AIDS Research and Interventions · HIV/AIDS drug development and treatment · Adolescent Sexual and Reproductive Health
Introduction
Option B+, a policy that mandated offering all pregnant women living with HIV (PWLH) initiate lifelong antiretroviral therapy (ART) irrespective of their CD4 count, has been adopted by most treatment programmes in sub-Saharan Africa [1], including South Africa in 2015 [2]. This policy aimed to reduce the risk of vertical transmission of HIV through suppression of HIV viral load (VL) during pregnancy, while also improving uptake and continuity of HIV care among women [3]. Option B+ adoption has dramatically increased the number of pregnant women initiating ART [4] and led to a substantial reduction in vertical transmission of HIV [5].
Though the implementation of Option B+ has also yielded high coverage of HIV testing at entry to antenatal care (ANC) [6], it is unclear whether it has affected the timing of engagement in HIV care in relation to ANC initiation. Engagement in HIV care prior to the start of ANC is critical to efforts to eliminate vertical transmission, as early engagement can ensure complete ART coverage and sustained suppression of HIV viral load throughout pregnancy, delivery and the postpartum period [7–9]. Data from South Africa’s National Antenatal HIV Sentinel Survey indicate that, compared to women initiating ART before pregnancy, women who initiated ART during pregnancy achieved lower rates of viral load testing (73% vs. 83%) and viral suppression (57% vs. 76%) [10].
Despite the important potential benefits of early engagement in HIV care, many women still only learn their HIV status through routine antenatal testing and commencement of ART occurs late in pregnancy [11]. The impact of the implementation of Option B+ on engagement in HIV care and viral suppression at entry to antenatal care is unclear. Here, we estimate proportions of women with evidence of engagement in HIV care and viral suppression at entry to antenatal care. We also assess factors associated with engagement in HIV care prior to pregnancy. We then estimate the effect of prior engagement in HIV care on subsequent VL suppression during pregnancy and finally, stratify all analyses by vertical transmission policy era (prior to and during Option B+ era).
Methods
Vertical transmission policies in South Africa
South Africa’s policy for providing antiretroviral therapy (ART) to PWLH has evolved over time, following World Health Organization (WHO) recommendations. In April 2008, a dual-therapy PMTCT programme was implemented through which women were offered Zidovudine starting at 28 weeks’ gestation or ART at a CD4 count of <200 cells/µL [12]. In 2010, Option A was introduced with Zidovudine starting at 14 weeks’ gestation for women with a CD4 count of >350 cells/µL or triple-drug ART for women with a CD4 count of ≤350 cells/µL [13]. The Option A regimen was replaced in 2013 by the WHO-recommended Option B approach, where women were offered triple-drug therapy throughout pregnancy, with postpartum withdrawal after cessation of breastfeeding for those ineligible for lifelong treatment [14]. The progression from Option B to Option B+ in 2015 was one of the key developments in the South African national HIV policy. Under Option B+, pregnant WLWH were offered lifetime ART regardless of CD4 count [2]. In September 2016, the Universal Test-and-Treat (UTT) policy expanded lifelong ART eligibility to all people living with HIV regardless of CD4 count [15].
Study population and data sources
This observational study uses two data sources. First, we used data from all adult (>18 years) pregnant women living with HIV who delivered at Rahima Moosa Mother and Child Hospital (RMMCH) in Johannesburg, South Africa, from 2013–2017. The RMMCH Cohort, supported by the Empilweni Services and Research Unit collects maternal and infant data including demographics, antenatal care, HIV treatment, delivery, early infant diagnosis of HIV, and maternal ART use [16].
Second, we used data from a national HIV cohort constructed using routine laboratory data from South Africa’s National Health Laboratory Service (NHLS), the sole provider of public sector laboratory services, serving 80–90% of the uninsured population. This cohort includes records of HIV-related tests used for treatment initiation and monitoring since 2004 [17]. Using an anonymized unique patient identifier previously developed and validated, individuals were followed longitudinally through their laboratory results as they progress through the HIV care and treatment cascade [18].
We used deterministic record linkage procedures using laboratory sample barcodes to link the RMMCH maternal cohort data to laboratory data from the NHLS National HIV Cohort. These alphanumeric barcodes are centrally allocated by NHLS and affixed to biological specimens by healthcare workers at the point of collection, usually clinics and hospitals. The barcode is the same across all the tests performed on the same person’s biological specimen and were captured in both NHLS and RMMCH databases. We manually validated a sample of linked data (1,200 records) comparing patient surname, first name and date of birth to ensure barcode linkages were correctly linking individuals across the two datasets. This process yielded exact matches for 87% of records and likely matches with minor typographical mismatches for an additional 9% [19].
Study variables
Primary exposure variable: For this analysis, our primary exposure was prior engagement in HIV care at entry to ANC. We used the two data sources described above to ascertain if a woman had accessed HIV care prior to entry to antenatal care: 1) self-reported ART use prior to entry to antenatal care in the RMMCH maternal records (the mother stated she was on treatment at the first antenatal visit for the current pregnancy); or 2) evidence of HIV-associated laboratory data (CD4 count and/or HIV viral load) observed in the NHLS national HIV cohort between three months prior to date of entry to antenatal care and known date of entry to antenatal care. We defined a engagement in HIV care prior to entry to ANC by either or both of these data sources indicating a woman had accessed HIV care prior to entry to antenatal care for the current pregnancy (i.e., either the woman self-reported ART use OR laboratory data indicated HIV care-associated laboratory test results). If neither data source indicated prior access to HIV care (i.e., woman did not report ART use AND no HIV-associated blood test results were observed in the NHLS National HIV Cohort prior to entry to antenatal care), then we classified that woman as not engaged in HIV care at the start of antenatal care for the current pregnancy.
Primary outcome variable: Our primary outcome was observed HIV viral load (VL) test result which we classified into two groups: 1) VL suppressed was defined as an observed VL test result <400 copies/mL; 2) VL unsuppressed was defined as VL test results ≥400 copies/ml. This threshold was the upper limit of detection for VL testing assays available in South Africa during the early part of study period. We chose this VL value threshold to allow for direct comparisons of VL outcomes between different policy eras.
Primary analysis: Our primary analyses estimated the effect of accessing HIV care prior to entry to antenatal care on VL outcomes. We measured this effect at two key time points for viral load testing during pregnancy: 1) entry to antenatal care (here we included any VL test within six months prior to date of entry to ANC), and 2) the pregnancy period between date of entry to ANC and delivery date.
Vertical transmission policy eras: We then defined three policy eras: 1) the period 1 January 2013 to 31 December 2014 was defined as “Prior to implementation of Option B+ policy”; 2) the period 1 January 2015 to 31 August 2016 was defined as “Option B+ era” and 3) the period from 1 September 2016 onwards as “Universal test and treat strategy (UTT) era.” We explored if the implementation of the Option B+ policy modified the effect of prior engagement in care on VL outcomes by further stratifying our primary analyses by vertical transmission policy era.
Statistical analysis
We commence the analysis by summarizing characteristics of mothers at entry to antenatal care using frequencies and simple proportions. We summarise rates of engagement in HIV care and describe characteristics of women with and without evidence of prior engagement in HIV care stratified by treatment policy era. We report frequency of VL testing at first antenatal care visit and during pregnancy and summarise proportions with viral suppression by engagement in care prior to pregnancy or during pregnancy. To assess for effect measure modification of vertical transmission policy era on effect of prior engagement in care on VL results at entry into ANC and during pregnancy, we stratify the proportion engaged in care prior to pregnancy achieving viral load suppression by policy era. Log-binomial regression is used to report crude and adjusted relative risks (aRR) and 95% confidence intervals (95%CI) of factors associated with study outcomes after adjusting for potential confounders.
Ethical considerations
This study was approved by the Human Research Ethics Committee (HREC) of the University of Witwatersrand. This is a secondary analysis of de-identified data collected as part of routine care and no direct participant interaction occurred.
Results
Characteristics of study participants at entry to antenatal care
A total of 4,865 pregnant women living with HIV included in the RMMCH Maternal HIV Cohort delivered infants at RMMCH during the study period 2013–2017 and were included in analyses (Fig 1).
Study eligibility flow chart of cohort of pregnant women living with HIV delivered infants at RMMCH during the study period 2013-2017.
Participant characteristics are shown in Table 1. The median maternal age at entry to antenatal care was 31 (IQR:26–35) years and median gestational age at entry to antenatal care was 21 (IQR:15–26) weeks. Overall, the median CD4 count cell count was 393 cells/mm^3^ (IQR:252–554). Overall, 17.0% of women had CD4 counts <200 cells/mm³ (advanced HIV disease). Stratification by gestational age at entry to ANC revealed that 11% of women booking in the first trimester had CD4 counts <200 cells/mm³, increasing to 18% in the second trimester and 19% in the third trimester. At first ANC visit, approximately half (51%) of women were in their second trimester while >80% had at least one other child. The majority of mothers were initiated onto standard first line as efavirenz based ART regimens with tenofovir and either lamivudine or emtricitabine.
Table 1: Characteristics of study participants at entry to antenatal care (n = 4,865).
Engagement in HIV care prior to entry to antenatal care
Overall, we found evidence of prior engagement in HIV care before entry to ANC for 65% of women (n = 3148). Of these, 10% (315/3148) self-reported prior ART use, 39% (1223/3148) had laboratory evidence of prior ART and 51% (1610/3148) had both. Fig 2 depicts trends in engagement in HIV care from 2013–2017. Overall, we found increasing evidence of engagement in HIV care prior to pregnancy by year through the study period, particularly among multigravida women. Proportions with prior engagement in HIV care increased from 17% in 2013 to 53% in 2017 among primigravid women and from 49% in 2013 to 73% in 2017 among multigravid women. More women engaged in HIV care before the first ANC visit during Option B+ era, compared to the period prior to Option B+ implementation (66% (2803/4,241) versus 55% (345/624), respectively).
Engagement in HIV care before and during Option B+ era among (A) primigravid pregnant women and (B) multigravida pregnant women.
Factors associated with engagement in HIV care among pregnant women accessing ANC services are summarized in Table 2. Younger women (age 18−24) were 20% less likely to have evidence of HIV care engagement prior to ANC compared to those 25−34 years (aRR 0.8; 95% CI:0.5–0.9). Those with very low CD4 (<200 cells/mm^3^) were 40% less likely to have evidence of earlier HIV care, compared to those with a CD4 of ≥500 cells/mm^3^ (aRR 0.6; 95% CI: 0.6–0.9). Women who were primigravid were also less likely to engage in HIV care early, compared to those with 2−3 pregnancies, (aRR: 0.7; 95%CI: 0.4–0.6). Women were 28% more likely to engage in HIV care early during the UTT era (aRR: 1.28; 95% CI: 1.18–1.38).
Table 2: Engagement in HIV care prior to antenatal care and predictors of prior engagement in HIV care.
HIV Viral load monitoring and viral suppression
A total of 4,910 viral loads were observed between entry to ANC and delivery among the 4,865 study participants. Of these, 41% (2002/4865) women had a VL test at entry to ANC, and 60% (2908/4865) had at least one VL observed between ANC booking date and delivery date.
Overall, 48% (n = 1520) of the 3148 women with evidence of engagement in prior HIV care had an observed VL at entry to ANC (Fig 3A). Of these, 61% (922/1520) were virally suppressed. In contrast, of the 1717 women with no evidence of prior HIV care at ANC, 482 (28%) had a VL test at entry to ANC and 32% (153/482) of these were virally suppressed. Overall, viral suppression at ANC among pregnant women reporting prior ART use was 29% (922/3148). Overall population level VL suppression at entry to ANC was 22% (1075/4865).
HIV viral suppression at A) entry to ANC and B) during pregnancy stratified by use of ART prior to ANC entry.
During pregnancy, VL testing was observed for 58% (n = 1825) of the 3148 women with evidence of engagement in prior HIV care (Fig 3B). Of these, 58% (1066/1825) were virally suppressed. Overall, rates of viral suppression during pregnancy were higher among pregnant women reporting prior ART use compared to suppression rates observed among women reporting no HIV care prior to entry into ANC (33% (1066/3148) vs 19% (322/1717). Overall population level VL suppression during pregnancy was 29% (1388/4865).
Fig 4 represents trends in viral suppression among women from 2014 to 2017 during pregnancy. In 2014 and 2015, a substantial proportion had suppressed VL (76% and 78%, respectively). However, in 2016, there was a notable increase in unsuppressed VL, rising to 36%; there was a slight recovery in 2017, with 67% suppressed. Overall, we observed higher viral suppression in 2014 and 2015 than 2016 or 2017.
Trends in viral load suppression rates during pregnancy, 2014-2017.
Factors associated with viral load suppression between ANC until delivery from multivariate log-binomial regression models are presented in Table 3. Women who started ART prior to pregnancy were more likely to achieve viral suppression than those who starting ART during ANC (aRR 1.10; 95% CI:1.11–1.33). Women initiating ART with higher CD4 count (≥500 vs < 200) were also more likely to achieve viral load suppression (aRR 1.61; 95% CI:1.40–1.72).
Table 3: Multivariate log-binomial regression model of factors associated with viral suppression among pregnant women during pregnancy.
Aligned with this, likelihood of VL suppression improved as policy eras shifted towards expanded access to ART (14% prior to Option B+, 29% during Option B+ and 33% during UTT; Table 3). In analyses stratifying the proportion engaged in care prior to pregnancy achieving viral load suppression by policy era, we found that engagement in HIV care prior to entry to ANC was associated with a higher probability of viral suppression across all policy eras (Table 4).
Table 4: Effect measure modification analysis of the impact of Option B+ era on effect of prior engagement in care on viral load suppression at entry to ANC and during pregnancy.
Discussion
Universal access to HIV care and treatment has been a reality for pregnant women in South Africa for over a decade [20]. Despite this, engagement in HIV care remains below treatment targets [21]. This observational study describes the engagement of pregnant women living with HIV in care prior to pregnancy and its impact on viral load monitoring and suppression, particularly in the context of changing HIV care policies. We report several key findings concerning engagement in HIV care prior to pregnancy. First, despite expanded access to HIV care, antenatal services continue to be a critical entry point for HIV care. In 2017, nearly half of primigravid women had no prior exposure to HIV care at their ANC booking, posing significant risks to their health and increasing the likelihood of vertical transmission to their infants. However, the expansion of access to ART as implemented under the Option B+ and UTT policies appears to have had a positive impact on engagement in care. More women (66%) engaged in HIV care before the first ANC visit during the Option B+ era, compared to 55% before Option B+. Similar improvements in engagement in care have been observed in the region, including a Malawian study that reported more women living with HIV entering ANC already on ART after introduction of Option B+ (18.7% pre- versus 30.2% post-Option B+) compared to the era prior to Option B+ implementation [22]. Data from Zambia also showed an increase in those on ART at first ANC visit from 9% in 2011, before Option B+, to 74% in 2015 during Option B+ [23]. Timely engagement in ANC may be influenced not only by structural barriers, in terms of access to care, but also dissemination of information about timely HIV care [24].
Secondly, early access to ART remains a critical step towards eliminating vertical transmission of HIV [21], as sustained viral suppression through continuous ART use is essential for this goal. Our findings highlight that increased maternal engagement in HIV care prior to pregnancy, particularly through early ART initiation, is crucial. We found that pregnant women who reported prior ART use had increased uptake of viral load testing and a higher proportion of viral suppression during pregnancy compared to those who initiated ART during pregnancy. Hence, interventions are needed to improve maternal engagement in HIV care before pregnancy to ensure sustained viral suppression and reduce the risk of vertical transmission. This findings are consistent with a previous study among participants initiating ART prior to pregnancy having had higher viral suppression [25].
Thirdly, we found that maternal age is an important factor in patterns of engagement in HIV and antenatal care. Younger women in our study were less likely (20%) to engage in HIV care before ANC compared to those aged 26–34 and older, consistent with other work indicating younger maternal age is a risk factor for poor HIV care engagement [10]. This pattern is closely linked with parity, as younger women are more likely to be experiencing their first pregnancy and thus new to both HIV care and ANC services. By the second pregnancy, rates of engagement in HIV care prior to ANC improve, as maternal age increases and women may have already been exposed to HIV care during a prior pregnancy [26]. Therefore, age on its own is not the sole driver of accessing care, but is influenced by prior exposure to care through earlier pregnancies.
Barriers to maternal HIV care engagement identified among younger mothers in other studies include instability in romantic relationships [27,28], difficulty accepting one’s HIV status [29], and fear of beginning lifelong treatment [30]. Efforts to support younger women in maternal HIV care should focus on strengthening social support networks, either by engaging existing supporters or introducing external peer supporters, such as other young women living healthy lives with HIV. Similarly, primigravid women were less likely to engage in prior HIV care compared to multigravida women. A recent study among women with an established HIV diagnosis at ANC found that those pregnant for the first time had an increased risk of poor care engagement, consistent with our findings [10]. This may be attributed to a lack of knowledge or experience with HIV testing and care services, fear of stigma or discrimination, and limited access to services [31,32]. Additionally, pregnancy and the postpartum period are high-risk times for HIV acquisition, further complicating engagement in care.
Despite continually expanding access to ART for pregnant women, we noted persistence of advanced HIV disease at presentation. Overall, 17% of women entering antenatal care did so with a CD4 count <200 cells/mm^3^. Unsurprisingly, those with low CD4 at entry to care were less likely to have engaged in HIV care prior to the current pregnancy. A previous study of a retrospective cohort of adult women also found that those with pre-pregnancy ART were more likely to start ANC with CD4 count ≥500 [27]. Pre-pregnancy ART improves immunologic and virologic control during pregnancy and there is therefore a need for renewed efforts in HIV testing, linkage to ART and viral monitoring. Additionally, stratification by gestational age at entry to ANC revealed concerning trends: 11% of women booking in the first trimester had a CD4 count <200 cells/mm^3^, while this proportion increased to 18% in the second trimester and 19% in the third trimester. These findings suggest that delayed ANC booking is associated with a higher likelihood of presenting with advanced immunosuppression. Thus, there is a pressing need to promote early ANC attendance, especially for women not previously engaged in HIV care, to reduce the burden of advanced HIV disease.
Finally, we noted with concern, low rates of VL testing during pregnancy (58%). Though this estimate is higher than previous estimates reported 20% in Gauteng Province, South Africa [28], 30% in Mozambique [33], and 40% from three districts of Kwazulu-Natal Province, South Africa [29], low rates VL monitoring during pregnancy calls for renewed attention to VL testing efforts during ANC. Our overall population level VL suppression during pregnancy of 29% is substantially lower than the UNAIDS target of 73%. While increased monitoring is important, improving VL suppression rates requires enhanced adherence support, timely ART initiation before pregnancy, and targeted interventions to address barriers to sustained ART use among pregnant women [30]. The findings that women with higher CD4 counts at the start of ART had a 1.5 times higher likelihood of achieving viral load suppression and viral load suppression rates increased as policies of expanded access to ART were introduced are consistent with the well-established benefits of initiating ART early in the course of HIV infection [34]. While the effect of engagement in care on VL suppression rates did not differ across expanded access policy eras, our results underscore the importance of early diagnosis and linkage to care, which allows for timely initiation of ART. By starting treatment at a higher CD4 count, the immune system is better preserved, and HIV can be suppressed more effectively. This not only improves health outcomes but also reduces the risk of transmission to others.
Our results should be interpreted in light of some limitations. Firstly, linking of maternal records to the National HIV cohort restricted our analysis to 2013–2017 since the NHLS cohort data are available until March 2018 but maternal records from RMMCH are through 2021. Secondly, while linking maternal and laboratory test datasets offers the opportunity to analyse laboratory results for ART clients beyond their originating facility, increasing the robustness of our estimates for VL testing, there are still challenges related to the generalizability of our findings. The cohort primarily reflects the population and practices of a single facility, which may not be representative of all ART clients in different regions or settings, especially outside urban areas. Moreover, missing data, particularly in the form of incomplete records or discrepancies between datasets, may introduce bias. This could potentially affect the accuracy of our estimates and should be considered when interpreting the findings. Lastly, we chose the VL threshold of <400 copies/mL as this was the assay detection threshold used in South Africa during the study period. We note that newer assays were introduced towards the end of the study period that were able to detect VL thresholds as low as 50 copies/mL and using the 400 copies/mL threshold would incorrectly classify test results with low level viraemia (50–400 copies/mL) as suppressed. We acknowledge that even low level viremia may be associated with poor health outcomes and this is directly addressed in a separate analysis [35].
Despite these limitations, our study leverages linking of maternal and laboratory test datasets which offers the opportunity to analyse laboratory results for ART clients beyond their originating facility, increasing the robustness of estimates for VL testing.
Conclusion
Expanded access to HIV care and treatment for pregnant women living with HIV under the Option B+ and UTT policies appears to have increased rates of engagement in HIV care prior to entry to antenatal care. Despite this, pregnancy and antenatal care services remain an essential portal of entry to HIV care among women living with HIV in South Africa, and a large proportion of pregnant women living with HIV still present for HIV care with advanced HIV disease. Prior use of ART at entry to antenatal care is also associated with other positive treatment outcomes including timely monitoring of HIV viral load and also likelihood of viral suppression during pregnancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection: recommendations for a public health approach. 2nd ed. Geneva: World Health Organization; 2016.27466667 · pubmed ↗
- 2Republic of South Africa Department of Health. National consolidated guidelines for the prevention of mother-to-child transmission of HIV (PMTCT) and the management of HIV in children, adolescents and adults. 2015.
- 3Wessels J, Sherman G, Bamford L, Makua M, Ntloana M, Nuttall J. The updated South African National Guideline for the prevention of mother to child transmission of communicable infections. South Afr J HIV Med. 2020;21(1):1079.32832113 10.4102/sajhivmed.v 21i 1.1079 PMC 7433286 · doi ↗ · pubmed ↗
- 4Di Carlo AL, Gachuhi AB, Mthethwa-Hleta S, Shongwe S, Hlophe T, Peters ZJ, et al. Healthcare worker experiences with Option B+ for prevention of mother-to-child HIV transmission in e Swatini: findings from a two-year follow-up study. BMC Health Serv Res. 2019;19(1):210. doi: 10.1186/s 12913-019-3997-1 30940149 PMC 6444445 · doi ↗ · pubmed ↗
- 5Maingi M, Stark AH, Iron-Segev S. The impact of Option B+ on mother-to-child transmission of HIV in Africa: a systematic review. Trop Med Int Health. 2022;27(6):553–63. doi: 10.1111/tmi.13756 35477948 PMC 9328372 · doi ↗ · pubmed ↗
- 6de Beer S, Kalk E, Kroon M, Boulle A, Osler M, Euvrard J, et al. A longitudinal analysis of the completeness of maternal HIV testing, including repeat testing in Cape Town, South Africa. J Int AIDS Soc. 2020;23(1):e 25441. doi: 10.1002/jia 2.25441 31997583 PMC 6989397 · doi ↗ · pubmed ↗
- 7Ngandu NK, Lombard CJ, Mbira TE, Puren A, Waitt C, Prendergast AJ, et al. HIV viral load non-suppression and associated factors among pregnant and postpartum women in rural northeastern South Africa: a cross-sectional survey. BMJ Open. 2022;12(3):e 058347. doi: 10.1136/bmjopen-2021-058347 35273061 PMC 8915310 · doi ↗ · pubmed ↗
- 8Yang L, Cambou MC, Nielsen-Saines K. The end is in sight: current strategies for the elimination of HIV vertical transmission. Curr HIV/AIDS Rep. 2023;20(3):121–30. doi: 10.1007/s 11904-023-00655-z 36971951 PMC 10239317 · doi ↗ · pubmed ↗