Evaluating the effect of the SMART intervention in people with recently diagnosed breast cancer who are being treated at a public tertiary hospital in Australia: protocol and statistical analysis plan for a single-blinded, single centre randomised controlled trial
Susan Stinton, Dale Edwick, Chloe Maxwell-Smith, Natasha Bear, Lauren J. Breen, Alejandro Dominguez Garcia, Elizabeth Dylke, Kate Edwards, Sally Lynch, Adam Lloyd, Barbara Mullan, Niamh Moloney, Ru-Wen Teh, Carol Watson, Kylie Hill, Mohammad Jobair Khan, Mohammad Jobair Khan

TL;DR
This study tests a new exercise program for people with newly diagnosed breast cancer to improve their quality of life during treatment.
Contribution
The SMART intervention introduces a tailored, telehealth-supported exercise program for breast cancer patients.
Findings
The trial will assess the impact of the SMART intervention on health-related quality of life and physical outcomes.
Secondary outcomes include muscle strength, exercise tolerance, and psychological factors influencing behavior change.
Results may inform future exercise programs for breast cancer patients based on treatment type and cancer stage.
Abstract
Adults undergoing treatment for breast cancer (BC) are advised to participate in regular exercise. However, many struggle to exercise consistently due to the side effects of systemic treatments including nausea, fatigue, and pain. In adults with newly diagnosed BC, this trial will evaluate the effectiveness of a new exercise intervention, compared with usual care, on outcomes including health-related quality of life (HRQoL). This randomised controlled trial is underway at an Australian tertiary hospital. The protocol was prospectively registered (Australian New Zealand Clinical Trials RegistryACTRN12623001168640p). Consenting adults with BC diagnosed within the prior six months, with planned chemotherapy and/or endocrine treatment will be randomised to an intervention or control group. Both groups receive usual physiotherapy and medical care. Those allocated to the intervention group…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
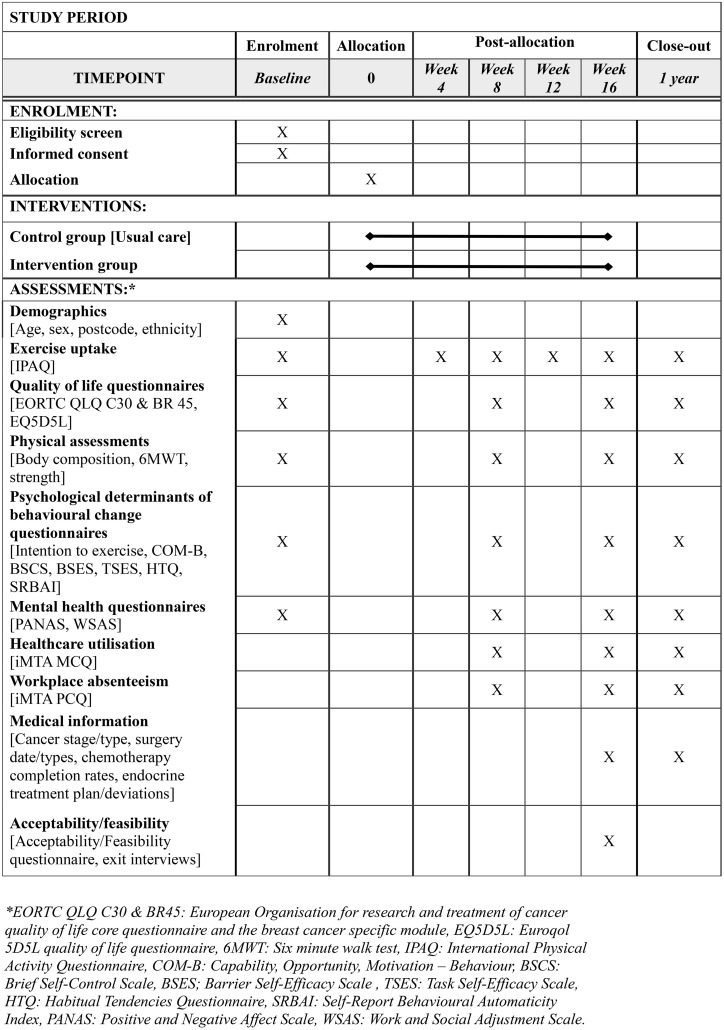 Fig 1
Fig 1- —http://dx.doi.org/10.13039/100012505Royal Perth Hospital Medical Research Foundation
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCancer survivorship and care · Lymphatic System and Diseases · Nutrition and Health in Aging
Introduction
Breast cancer affects mainly cisgendered women with a global incidence of 2.26 million in 2020 [1]. Fortunately, breast cancer survival rates have improved with up to nine out of ten people diagnosed with breast cancer deemed to be cancer-free at five years following their initial diagnosis [2]. Although largely successful in terms of survival, systemic treatments including chemotherapy and endocrine treatments for breast cancer have many unwanted side effects, such as fatigue, pain and worsened mental health, which reduce health-related quality of life (HRQoL) for many years after completion of treatment [3]. Strategies are needed to improve HRQoL during and following completion of treatment [3].
National and international oncology societies recommend that people undergoing treatment for cancer engage in 150 minutes of moderate intensity aerobic exercise and two sessions of resistance exercise each week [4,5]. This recommendation is informed by systematic reviews and meta-analyses of randomised controlled trials (RCTs) that favour exercise groups over control groups for measures of HRQoL [6,7], pain [8], fatigue [9], physical function [10], and mood [11]. Preliminary data suggest that exercise undertaken during treatment for cancer may improve chemotherapy completion rates [12] and reduce breast cancer related mortality [11].
Notwithstanding these benefits, earlier work has reported that up to 78% of people undergoing treatment for breast cancer do not meet the recommended amount of exercise and further, 23% reduce their participation in exercise during cancer treatment [13]. Engaging in regular exercise during systemic treatments, such as chemotherapy and endocrine therapy, is challenging due to common and debilitating side effects such as nausea, fatigue and pain [14,15]. During this time, an intervention to increase participation in exercise should aim to adopt a flexible and individualised approach, be endorsed and supported by oncology care teams, and include specific behaviour change techniques to assist individuals receiving treatment for breast cancer with navigating barriers [16].
To optimise exercise among adults undergoing treatment for breast cancer, an exercise intervention was co-designed by a team that included physiotherapists, oncologists, psychologists, exercise physiologists and consumer representatives with lived experience of breast cancer. This exercise intervention has several novel aspects such as; i) bespoke tailoring of the program which considers age, baseline fitness levels, individual preferences and breast cancer stage, ii) inclusion and detailed mapping of behaviour change techniques, and iii) close monitoring using wearable devices to allow modification of programs dependent on treatment and other relevant health symptoms.
The primary research question that we will answer is:
In adults who are newly diagnosed with breast cancer, does the SMART intervention, compared with usual care, change HRQoL (primary outcome), peripheral muscle force-generating capacity, body composition, exercise tolerance, exercise adherence, healthcare utilisation, workplace absenteeism and presenteeism, chemotherapy or endocrine completion rates (secondary outcomes) at the primary trial endpoint, 16 weeks following randomisation? Exploration of the secondary outcomes will be hypothesis generating and look for evidence of an effect in outcomes deemed relevant by a project steering committee. In addition, we plan to utilise this dataset to undertake a number of secondary analysis. These will also be hypothesis-generating and help to inform future work in this area. These secondary analysis include:
An exploration of variables that influence the magnitude of any change in HRQoL following completion of the SMART intervention. These potential moderators include treatment pathways, cancer stage, and the type, quantity and frequency of exercise undertaken. Understanding which, if any variables related to the exercise prescription are associated with an increased magnitude of change in outcomes will assist with optimising future exercise interventions.To explore of any differences in the characteristics of those who respond well to exercise training (i.e., responders) versus those show minimal change (i.e., non-responders) will help with the design of future research that aims to improve outcomes in non-responders.An exploration of the influence psychological determinants of behaviour change, such as capability, opportunity, and motivation, have on changes in physical activity levels from baseline to post-intervention and to long-term follow-up. This will help identify which behavioural determinants are most strongly associated with short-term improvements and long-term maintenance of physical activity.An exploration of the associations between physical activity and psychological wellbeing, specifically changes in positive and negative affect, and impaired functioning due to mental health across the intervention and follow-up period. These analyses will help identify whether higher levels of physical activity are associated with improvements in psychological wellbeing and functioning.
Methods
This RCT will evaluate the effect of an experimental exercise program called the SMART intervention (Self-determined, Monitored, Adaptable Rehabilitation program with Telehealth support) in adults who have been diagnosed with breast cancer within the previous 6 months who require chemotherapy and/or endocrine treatment. This study was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12623001168640p) prior to commencing recruitment (detailed in Supplementary Item 1). Ethics approval has been given from the Central WA Health Human Research Ethics Committee (formally under Royal Perth Hospital Human Research Ethics Committee RGS00006136) and Curtin University Human Research Ethics Committee (HRE2024−0153). Site specific approvals were obtained from the participating health service. Any protocol (Supplementary Item 2: Full protocol V3.0) amendments will be submitted to this registry and the ethics committees. This manuscript has been described in accordance with the SPIRIT guidelines (SPIRIT: http://spirit-statement.org, checklist in Supplementary Item 3).
Setting
This is a single-blinded randomised controlled trial that is being conducted at Royal Perth Hospital (RPH); a 450-bed tertiary public hospital in Australia. Royal Perth Hospital offers a multi-disciplinary breast cancer treatment clinic (RPH-BC) which treats people diagnosed with breast cancer who reside in metropolitan and rural locations throughout the state of Western Australia.
Recruitment
Adults are eligible for inclusion if they have a primary breast cancer, diagnosed within the previous six months and have planned (or have started) chemotherapy or endocrine treatment for their breast cancer. Potential participants are excluded if they; i) are undergoing active treatment for any other primary cancer diagnosis or are receiving systemic treatment for a prior breast cancer diagnosis, ii) were diagnosed with breast cancer more than six months prior to recruitment or, iii) have a co-morbid condition which precludes independent participation in exercise. Potential participants with Stage 4 Breast Cancer (according to the American Joint Committee on Cancer Staging Manual, 8^th^ Edition) [17] are eligible to participate in the study, providing they have consent from their treating medical oncologist. Participants are required to have telephone and internet access or agree to attend RPH for all assessments and relevant components of the SMART intervention.
Eligible participants are identified at the RPH-BC. A clinician who is independent to the study team makes first contact with potential participants. Those who meet the study criteria and express an interest in participating in the study are contacted by a member of the research team to provide verbal and written information about the study (Supplementary Item 4). The study is also advertised in hospital outpatient clinics using posters and pamphlets and potential participants are encouraged to contact the study team (via phone or email) to express interest.
Consent and randomisation
Once the participant has had time to consider their enrolment, written informed consent is obtained prior to any data collection. The written informed consent form will be signed by the participant, the study researcher, and witnessed by an adult independent to the research team. Participants are required to complete all baseline assessments before proceeding to randomisation. Participants are randomised to the intervention group (IG) or the control group (CG) on a 1:1 ratio, according to a computer-generated randomisation sequence. This sequence is stratified for; i) treatment pathway (chemotherapy vs endocrine treatment vs combined chemotherapy and endocrine treatment) and, ii) whether the participant regularly engages in exercise (defined as participating in exercise at least once a month for the six months prior to recruitment) prior to their breast cancer diagnosis. The sequence is stored and concealed using a secure web-based data management application, Research Electronic Data Capture (REDCap). Fig 1 summarises the participant flow according to the SPIRIT schedule of enrolment, interventions, and assessments.
SPIRIT study protocol schedule of enrolment, interventions, and assessments.
Interventions
Participants in both groups receive usual care from the RPH-BC and oncology service. Specifically, all people who require mastectomy or surgical resection of tumours with sentinel node clearance and/or axillary clearance are referred to a physiotherapist. Pre- and post-operative physiotherapy care may include education regarding the importance of exercise throughout cancer treatment, post-operative upper limb range of motion exercises, and/or referral to off-site oncology exercise groups. Lymphoedema surveillance and management, lymphatic cording, reduced shoulder range of motion, and/or other post operative complications are managed by physiotherapists on an as-needed basis. In addition, people can request to see a physiotherapist and the medical team can refer people to a physiotherapist for education regarding participation in exercise while undergoing chemotherapy at RPH. Any concomitant care relating to breast cancer treatment and/or other medical conditions will be offered in both groups, as per usual care.
Those allocated to the IG will receive the SMART intervention, which was co-designed with people who have breast cancer, to address many of the known barriers to exercising during cancer treatment. Consumer representatives have collaborated on the development of the protocol from trial inception. The core components of the program include; i) up to 16 one-on-one training sessions over the 16-week intervention period, ii) access to semi-supervised group gym sessions for participants to carry out their individual exercise programs, and iii) monitoring of supervised and home exercise sessions using strategies (described below). The SMART program will be delivered in an adaptable way, specific to each person, according to treatment symptoms, and progressed/regressed accordingly. An example of a supervised exercise session is detailed in Table 1 below.
Table 1: Example of a supervised exercise session. Note that all exercise prescription is based on individual preferences, abilities, medical considerations and goals.
The guiding principles that have shaped this intervention are as follows:
S**elf-determined: Participants are encouraged to select exercises they enjoy (e.g., walking, swimming, cycling, dance) at the time of day that suits them best. They are encouraged to exercise at home, in the community or can access the gymnasium in the Physiotherapy Department at set times each week. Participants are encouraged to use a diary to record participation in exercise and to rate their physical and emotional health on a Visual Analogue Scale (VAS). These entries are reviewed at their one-on-one sessions.
M**onitored: Participants are encouraged to attend regular one-on-one 60-minute exercise training sessions with a physiotherapist. During these sessions, together with a physiotherapist, the participant will; i) reflect on the achievement of the target behaviour and their response to the exercise (e.g., pulse rate and rating of perceived exertion [RPE]) [18] over the previous week, ii) report any adverse events or post-exertional malaise, iii) undertakes aerobic and resistance exercise with feedback, adjustment and reassurance as needed, iv) plan the exercise training sessions for the following week, and v) discuss behaviour change techniques (BCTs) to optimise success with achieving the intervention message. [19] Physiotherapists providing the SMART intervention will be upskilled in these techniques through a custom written resource for the study and one-on-one education with the trial staff member supporting the psychological and behaviour change components [20]. Example BCTs include goal setting around the target behaviour, feedback from clinic physiotherapists, action- and coping-planning for managing barriers, and environmental restructuring.
A**daptable: The one-on-one sessions may be scheduled weekly on a regular day and time, or if the participant is suffering from treatment side effects (e.g., nausea and vomiting from day two to seven following chemotherapy), scheduling of these appointments may be more variable. They can choose to complete these sessions in person (at RPH) or via a telehealth appointment.
R**ehabilitation: The target behaviours of the SMART program are informed by guidelines endorsed by National and International organisation including the American College of Sports Medicine (ACSM) and Clinical Oncology Society of Australia (COSA) [5,21]. Participants are encouraged to engage in both moderate intensity aerobic and resistance exercise. Aerobic exercise has been defined as any exercise that involves continuous repetitive movement using large muscle groups or whole-body exercise. Moderate intensity has been defined as that which requires either; i) a heart rate at 60–75% of their age-predicted maximum heart rate [22] or, ii) effort that is perceived to be ‘somewhat hard’ or 13–14 on the Borg RPE [18]. Vigorous intensity aerobic exercise will be defined as exercise performed at over 75% of their age predicted maximum heart rate or a Borg RPE rating of 15 (‘hard’) or more. Resistance exercises are prescribed for both upper body and lower body muscle groups. The mode (i.e., free weights, TheraBand, body weight, machine based) and specific exercise are tailored to each participant, according to their preference. In order to prescribe the load used for each exercise, the 10 repetition-maximum (RM) is determined [23] and training is prescribed at this load for 2 sets of 8 repetitions. Exercises are progressed by increasing repetitions (to 12), then sets (to 3) then weight. Exercises will be progressed if the Borg RPE scale for each exercise is less than 13 OR if participants are able to complete more than 3 sets of 12 repetitions without concern. Exercises will be progressed or regressed at the one-on-one sessions. If a participant has Stage 4 Breast Cancer, the exercise prescriptions set out above are adapted according to their individual safety considerations based on the location of metastases. [21]
T**elehealth support: Participants are offered to attend their one-on-one sessions via telehealth. In this way, the study can enrol people who live in rural or remote areas of Western Australia. Additional online support using an online exercise prescription service, Physitrack, an online exercise prescription tool with a website or app interface (Physitrack PLC), will provide means for written exercise prescription, monitoring and exercise reminders.
Managing hospital admissions, complications and sub-optimal adherence
It is anticipated that some study participants will require planned surgery such as the resection of their cancer, breast reconstruction procedures, and/or inpatient hospital care during the 16-week intervention period. Participants in both groups will have their 16-week intervention period paused during any inpatient admission or period of post-operative exercise restriction. For participants who develop medical complications such as low platelets, anaemia, or post-operative complications, exercise prescription will be modified following consultation with the treating oncologist and in accordance with national guidelines and position statements. [21,24]
In cases where participants in the IG do not report reasonable progress towards meeting their intervention goals over two consecutive weeks, the physiotherapist will meet with a member of the research team with expertise in the behaviour change theory to debrief and adjust the BCTs delivered if required. An example of an exercise plan is included in Table 2.
Table 2: Example exercise plan.
Implementation fidelity
Fidelity with the SMART intervention will be assessed using two methods: participant reporting and wearable technology.
Participant reports.
Participants in the IG are encouraged to diarise any participation in exercise as well as physical and emotional health on a VAS. These entries are reviewed at the one-on-one sessions. Content of these sessions will be documented by the physiotherapists. Additionally, participants will be contacted by the physiotherapist (via telephone) to complete the International Physical Activity Questionnaire (IPAQ) [25] at baseline assessment, on commencement of the intervention and at four-week intervals until completion of the intervention.
Wearable technology.
For the duration of the intervention period, participants in the IG will be asked to wear a Fitbit (Charge 5, Google Fitbit) which records pulse rate and bodily movement (e.g., activity and exercise minutes). Data from the Fitbit will be compared with diary entries to corroborate participation in exercise [26].
Measurement and blinding
At the time informed consent is obtained, participant characteristics (e.g., gender, height, weight, employment status, ethnicity, and postcode), breast cancer staging (according to the 8^th^ Edition AJCC Manual) [17] and expected treatment pathway for their breast cancer (e.g., chemotherapy and/or endocrine therapy) will be recorded. If a participant requests to withdraw from the study, they will be asked if we can retain any previously collected data to be used in the analysis.
To reduce potential bias the person collecting outcome measures is blinded to group allocation. This is achieved through two strategies. First, baseline assessments will be completed prior to randomisation. Second, the physiotherapy staff who deliver usual care and/or the experimental intervention will not perform any follow-up assessments. Data collected via self-reported questionnaires will be completed by the participants via the REDCap automated survey invitation feature.
Outcomes
Health-related quality-of-life is the primary outcome and will be assessed using three self-reported questionnaires; the disease specific European Organisation for Research and Treatment of Cancer (EORTC) Quality of Life C30 [27] questionnaire together with the breast cancer specific BR45 module [28], and the non-disease specific Euroqol EQ-5D-5L questionnaire, detailed in Table 3 [29]. These questionnaires have been validated for use in the breast cancer population [30,31]. All other secondary outcomes are listed in Table 3, with details of the methods of assessments, measurements variables, modes of assessment and methods of aggregation. Where available for the breast cancer population, minimum clinically important differences and psychometric properties are also noted in Table 3.
Table 3: Description, measurement variables, methods of assessment, and aggregation for secondary outcomes.
Timeline
The SMART trial will recruit participants over an estimated two-year period which commenced on the 17^th^ June 2024 and is estimated to end on the 17^th^ June 2026. To allow for long term follow-up, planned data collection will continue for one-year following recruitment of the last participant, estimated to end in June 2027. At the time of submission of this paper, 56 participants had been recruited, with no data analysis, and no submission of publication of results. Results from the primary end point, 16 weeks following the baseline assessment, are expected by the end of 2026, and from the long-term follow-up by the end of 2027.
Sample size calculation
Sample size calculations were conducted using the physical functioning scale in the EORTC BR-30 (continuous data) as the dependent variable. To detect a between group difference in this outcome of at least 8 (out of 100) (estimated minimal clinically important difference), [30] assuming a standard deviation of 20.5 (derived from published literature) with an α = 0.05 and 1-β = 0.8, we will need to recruit 104 participants in the IG and 104 participants in the CG. To account for 20% drop-out, we plan to recruit a sample size of 130 participants in each group. Therefore, we aim to recruit 260 participants over 24 months.
Data management and availability
Signed written informed consent forms will be maintained within locked cabinets in the physiotherapy department at RPH, only accessible to the research team. De-identified data will be collected and managed on REDCap. On analysis, data will be examined for outliers, implausible values, duplicates, and logic checks performed between variables.. Full data management procedures are detailed in the full protocol, Supplementary Item 2. As this is a protocol paper, no datasets were generated or analysed. The results will be published in a scientific journal. Upon study completion, the data generated from this study will be available from an online repository or from the corresponding author upon reasonable request, as far as possible under legislation.
Analysis
To ensure the study statistician remains blinded to the study group, a member of the research team who is not involved in the analysis, will extract the group randomisation list and assign a generic name to each group (e.g., red and blue group). Patterns of missing data will be explored and multiple imputations considered for missing independent covariates where appropriate. [66,67].
The analyses for the primary research objective will be performed according to the intention-to-treat principle. For the primary outcome, HRQoL, with 4 assessment points, linear mixed models will be used to account for repeated measures with participant ID entered as a random effect. The primary time point of interest will be the end of the intervention phase. Group, time, and group-by-time interactions will be included as fixed effects in the regression model. The baseline measure of the outcome will be included as a covariate to adjust for baseline differences. The model will also be adjusted for randomisation variables and confounders, such as age, surgery type and weeks since surgery and/or chemotherapy pathway (neoadjuvant or adjuvant). Estimates of the effects will be reported with their corresponding 95% confidence intervals.
Between group differences for the secondary measures (peripheral muscle force-generating capacity, muscle mass, exercise tolerance) will be examined using the same method described for the primary outcome.
To understand any moderator effects, the listed covariates will be entered into a multivariable model using the outcomes listed above. In addition, adherence will be examined to see if it mediates the relationship with the outcomes, by calculating the indirect through the use of partial coefficients.
To address the research question investigating whether psychological determinants and mechanisms of behaviour change predict changes in physical activity levels in participants, bivariate correlations will first be conducted to explore associations between intention, self-efficacy, habit strength, and COM-B constructs (capability, opportunity, and motivation) with physical activity levels at each time-point. All relevant behavioural determinants will then be entered into a mixed-effect regression model, to examine if any behavioural determinants relate to physical activity levels.
The research question investigating whether physical activity is associated with psychological wellbeing will be assessed using correlations between physical activity levels, positive and negative affect data from the PANAS, and scores from the WSAS assessing impaired functioning due to mental health at each time-point. If appropriate, mixed-effects models will then be used to examine if physical activity relates to any of the psychological wellbeing variables.
Participants’ perceptions of the SMART intervention will be explored using data from the feasibility/acceptability questionnaire [63]. Quantitative data will be assessed using descriptive statistics. Additionally, responses to the open-ended items from the questionnaire will be coded and analysed using conventional content analysis using an inductive coding approach [68]. Data from the exit interviews will also be analysed using qualitative methods (such as thematic analysis) to explore participants’ reasons for engagement [or lack of engagement) [69].
Sub-group analysis will be performed for the HRQoL EORTC and EQ5D5L questionnaires for; i) those with Stage 4 breast cancer at the time of recruitment versus those with lower cancer stages, and ii) treatment regimens involving curative intent to treat versus palliative treatment. Model fit for regression models will be performed by examining residuals (normality and constant variance). For models with repeated measures random coefficients will also be examined for normality and constant variance. If model fit is poor, such as for skewed or bounded distributions then non-linear models will be explored using a gamma or inverse gamma generalised linear mixed model [70]. Any deviations from the plan will be described in the final manuscript.
Trial governance, risk management and monitoring
A steering committee will meet monthly and oversee the running of the trial and administrative requirements. Any adverse events will be reported to the steering committee and recorded in the person’s medical record and classified as minor (i.e., resolve without any need for a medical review) or non-minor (i.e., those that warranted a medical review). Examples of minor adverse events might include episodes of dizziness or nausea during exercise or muscle soreness and generalised malaise on completion of an exercise session. Example of non-minor adverse events might include an injurious fall or cardiac event.
The trial intervention and assessments will be delivered by physiotherapists employed at RPH. Physiotherapists in Australia are trained in providing exercise prescription for a wide variety of health conditions. All trial physiotherapy staff are registered and fulfill the requirements of the Australian Health Professional Regulation Agency and have annual training to stay up to date with departmental emergency procedure training specific to gym-based exercise sessions and telehealth appointments run through the RPH.
A data and safety monitoring board (DSMB) has been established for this research project to review trial data every 6 months and for reporting of potential adverse events. The DSMB comprises three experienced researchers, independent to the clinical researchers actively working on the project. Any adverse events will be reported to the HREC within 48 hours, will be discussed at the DSMB meetings and reported to the treating medical team as appropriate.
Discussion
This trial will investigate whether a more structured and supported exercise program provided via the SMART intervention will optimise exercise participation and improved health-related quality of life, and/or other secondary outcomes, compared to those receiving usual physiotherapy care alone. If successful, there will be justification to change routine clinical practice in a hospital setting. Heightened understanding of any variables that are associated with better outcomes will refine implementation of exercise interventions, so that physiotherapists or other exercise providers are able to optimise delivery of programs in a flexible way, with clear target goals to optimise outcomes through the breast cancer treatment journey. A greater understanding of the psychological determinants and mechanisms of change for exercise will guide interventions promoting exercise and the behavioural strategies underpinning them. As barriers to exercise are heightened for people undergoing a cancer journey, and people are at elevated risk of comorbidity following cancer treatment, exercise interventions are of particular importance for improving quality of life and related function and psychological outcomes in this population [14]. Findings will be shared through publications to inform usual care practices delivered by both the immediate care team and allied health professionals, harnessing the multidisciplinary care approach.
A major strength of this study was the co-design of the exercise intervention which took into consideration perspectives of several healthcare disciplines and, perhaps most importantly, the voices of people who have survived breast cancer. In addition, the exercise intervention was designed to be inclusive of both males and females, with any stage of breast cancer (including stage 4), who resided in either rural or metropolitan areas.
Limitations of this study involve the single centre design, which potentially will reduce the generalisability of the results, as usual care practices may differ between health services providers both within and outside Australia. Variations in usual care may reduce the generalisability of our estimate of the between-group differences. Although all follow-up assessments are completed by a researcher blinded to the study group, it was not possible to blind the participants or the physiotherapist delivering the intervention to their group allocation. This is a common shortcoming of studies that explore exercise interventions. Although the primary research question does not attempt to inform the mechanism of the interventions, our secondary analysis will allow us to explore factors that may modify the magnitude of between-group differences which will inform future service delivery. Overall, we feel there is high likelihood that the results will be clinically meaningful.
Supporting information
S1 FileTrial registration data.(DOCX)
S2 FileFull protocol [as per version in ethics approval].(PDF)
S3 FileSPIRIT checklist.(PDF)
S4 FileParticipant information and consent form [as per version in ethics approval].(PDF)
S5 FileHealthcare utilisation questionnaire (revised).(PDF)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Piñeros M, Znaor A, et al. Cancer statistics for the year 2020: An overview. Int J Cancer. 2021:10.1002/ijc.33588. doi: 10.1002/ijc.33588 33818764 · doi ↗ · pubmed ↗
- 2Giaquinto AN, Sung H, Miller KD, Kramer JL, Newman LA, Minihan A, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72(6):524–41. doi: 10.3322/caac.21754 36190501 · doi ↗ · pubmed ↗
- 3Di Meglio A, Havas J, Gbenou AS, Martin E, El-Mouhebb M, Pistilli B, et al. Dynamics of long-term patient-reported quality of life and health behaviors after adjuvant breast cancer chemotherapy. J Clin Oncol. 2022;40(27):3190–204. doi: 10.1200/JCO.21.00277 35446677 PMC 9509127 · doi ↗ · pubmed ↗
- 4Hart NH, Stout NL, Haywood D, Ashbury FD, Chan RJ, Fitch MI, et al. World Health Organization package of interventions for rehabilitation for cancer: a MASCC-endorsed resource for global action to address unmet rehabilitation needs of people affected by cancer. Support Care Cancer. 2024;32(7):417. doi: 10.1007/s 00520-024-08569-1 38847912 · doi ↗ · pubmed ↗
- 5Cormie P, Atkinson M, Bucci L, Cust A, Eakin E, Hayes S, et al. Clinical oncology society of Australia position statement on exercise in cancer care (Version 3). Med J Australia. 2020;209(4):184–7.10.5694/mja 18.0019929719196 · doi ↗ · pubmed ↗
- 6Hart NH, Stout NL, Haywood D, Ashbury FD, Chan RJ, Fitch MI, et al. World Health Organization package of interventions for rehabilitation for cancer: a MASCC-endorsed resource for global action to address unmet rehabilitation needs of people affected by cancer. Support Care Cancer. 2024;32(7):417. doi: 10.1007/s 00520-024-08569-1 38847912 · doi ↗ · pubmed ↗
- 7Nie X, Yang T, Nie X, Yuan J. Comparative effects of different types of physical activity on health-related quality of life in breast cancer survivors: A systematic review, network meta-analysis, and meta-regression. Heliyon. 2024;10(10):e 31555. doi: 10.1016/j.heliyon.2024.e 31555 38831804 PMC 11145476 · doi ↗ · pubmed ↗
- 8Plinsinga ML, Singh B, Rose GL, Clifford B, Bailey TG, Spence RR, et al. The effect of exercise on pain in people with cancer: a systematic review with meta-analysis. Sports Med. 2023;53(9):1737–52. doi: 10.1007/s 40279-023-01862-9 37213049 PMC 10432370 · doi ↗ · pubmed ↗