The Impact of Climate-Related Natural Disasters and Extreme Weather Events on Plastic and Reconstructive Surgery: A Scoping Review
Hannah D Shi, Alex J Dong, Seungil Lee, LaYow C Yu, Carol Mita, Colby Hyland, Justin Broyles

TL;DR
This review explores how climate-related disasters increase the need for plastic surgery interventions like wound closures and amputations, emphasizing the growing role of plastic surgeons in disaster response.
Contribution
The study provides a comprehensive overview of plastic and reconstructive surgery needs arising from climate-related disasters, highlighting regional and procedural trends.
Findings
35 studies showed a rise in plastic surgery needs following natural disasters, with hand and lower extremity surgeries being most common.
High-income countries contributed 74.3% of the studies, indicating regional disparities in disaster-related surgical research.
Burns, soft tissue trauma, and limb injuries were the most frequent injuries requiring plastic surgery interventions.
Abstract
The increasing frequency and severity of natural disasters, exacerbated by climate change, have significant implications for medicine, particularly in the realm of plastic and reconstructive surgery. Current research indicates that limb injuries, soft tissue trauma, and burns are among the most common injuries sustained during natural disasters. The immediate need for surgical interventions, such as wound closures, skin grafts, amputations, and limb salvage techniques, underscores the vital role of plastic and reconstructive surgery in disaster response. We conducted a comprehensive literature search across PubMed, Embase, Global Health, and Web of Science Core Collection on March 4, 2025. All English-language original research studies that described climate-related natural disasters, extreme weather, or pollution requiring plastic and reconstructive surgery intervention were screened…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
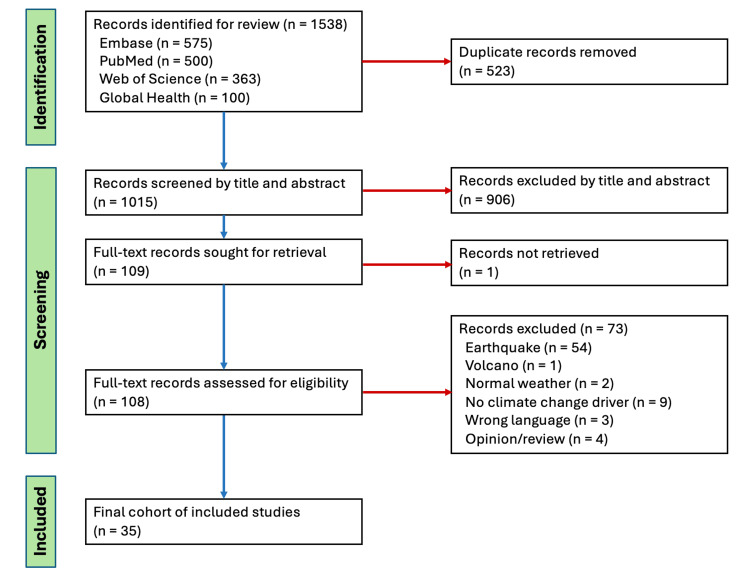 Figure 1
Figure 1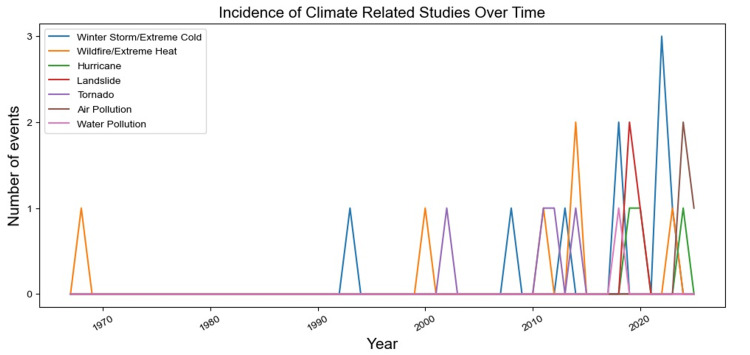 Figure 2
Figure 2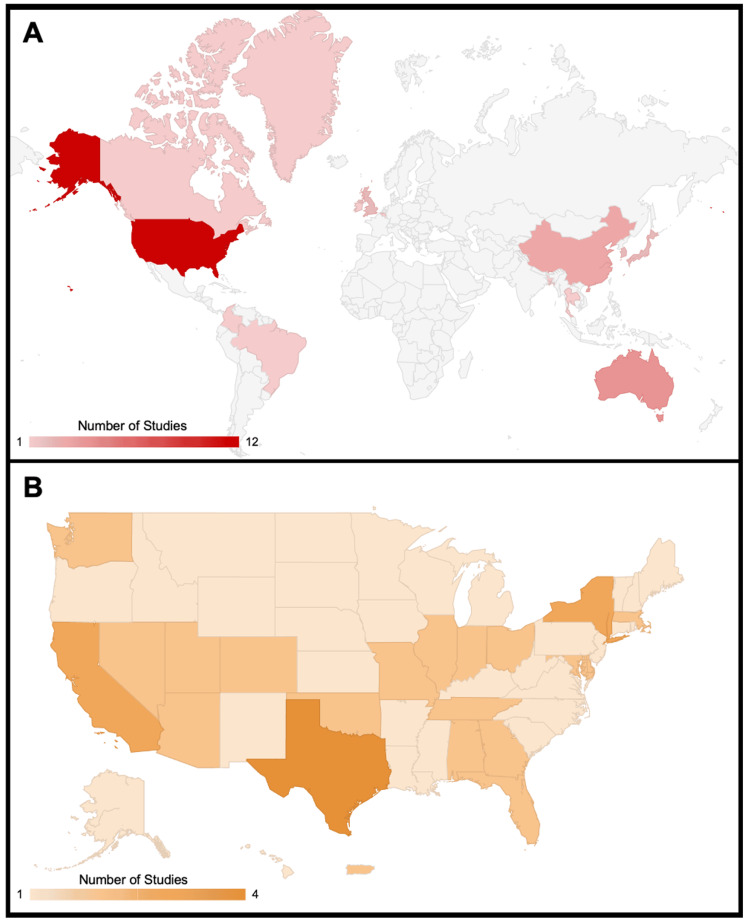 Figure 3
Figure 3| Study | Weather Event | Date of the Weather Event | Type of Injury | Type of Surgical Intervention | Total Number of Patients (n) | Patient Age as Reported | Patient Sex | Climate-Related Study Findings | Study Type | Duration of the Study Period |
| Krakauer et al. [ | Air pollution | 2016 - 2020 | Non-syndromic cleft lip and/or palate | Cleft lip and palate repair | 1,309 | - | - | SO₂ and PM exposure were linked to increased rates of non-syndromic cleft lip/palate, highlighting air pollution as a prenatal risk factor. | Retrospective cohort | 2016 - 2020 |
| Harris et al. [ | Air pollution | 1/1/1993-11/27/2017 | Increased breast cancer risk | Breast cancer reconstruction | 205 | 48.7 (mean), 13.3 (SD) | 0 M 205 F | Chronic exposure to air pollution and particulate matter mediates inflammatory processes that increase the risk of breast cancer. | Cross-sectional | 1/1/1993-11/27/2017 |
| Kim et al. [ | Air pollution | 2011 - 2019 | Diabetic foot injury | Lower limb artery operations, amputation | 347,543 | 61.69 ± 11.53 (mean) | 164,593 M 182,950 F | Urban regions of South Korea exposed to greater air pollution had significantly increased risks of diabetic foot complications. | Retrospective cohort | 2011 - 2019 |
| Choudhury et al. [ | Water pollution | 1/2004 - 12/2015 | Skin cancer | Resection | 960 | 18-95 | 528 M 432 F | Mucocutaneous skin lesions were significantly more prevalent in populations exposed to water pollution. | Case control | 1/2004 - 12/2015 |
| Taylor et al. [ | Wildfire | 2/7/1967 | Burns | Surgical excision, debridement, and skin grafting | 35 | 10 to 70 | 26 M 9 F | Hospital overload post-disaster led to high patient mortality, highlighting the need for better emergency capacity and support for smaller hospitals. | Case series | - |
| Zeman et al. [ | Wildfire | 1/1/1988 | Burns | Amputation and split skin grafts | 1 | 51 | 1 M 0 F | Prosthetic/orthotic techniques can lead to excellent functional results as an alternative to surgery. | Case report | - |
| Cleland et al. [ | Wildfire | 2/2009 | Burns | Skin grafts and escharotomy | 19 | 31-77 | 14 M 5 F | Seventeen out of the 19 patients admitted following the first 48 hours of the bushfires underwent surgery, resulting in 4355 minutes of OR time in the first week. | Retrospective cohort | 2/2009 |
| Whiting et al. [ | Extreme heat | - | Burns | Surgical excision, debridement, and skin grafting | 2 | 66, 58 | 1 M 1 F | Contact pavement burns are a new mechanism of injury from climate change and result in longer hospital stays and more intensive surgical intervention compared to traditional burns. | Case series | - |
| Nakamura et al. [ | Extreme heat | 6/2011 - 7/2011 | Dry necrosis | Debridement, skin graft, amputation, and flap | 2 | 81, 77 | 1 M 1 F | Heat stress related to heatwaves may predispose patients to necrotic damage that requires surgical interventions. | Case series | 6/2011 - 7/2011 |
| Xiang et al. [ | Extreme heat | 7/01/2001 - 6/30/2010 | Soft wound injuries, amputations, MSK and connective tissue diseases | - | 125,267 | Large Range, with many (~1/2) patients between 35-54 | 85138 M 40129 F | Heatwaves increased occupational burns, wounds, lacerations, and amputations, especially among older male workers. | Retrospective cohort | 7/01/2001 - 6/30/2010 |
| Lorentzen et al. [ | Winter storm | 12/2016 - 2/2017 | Frostbite | Wound debridement, drainage, and amputation | 6 | 46, 31, 44, 32, 53, 57 | 5M 1F | Populations in the Arctic Circle are particularly at risk of frostbite due to frequent cold temperature extremes. | Case series | 12/2016 - 2/2017 |
| Cindass et al. [ | Winter storm | 2/12/21 - 4/1/21 | Frostbite | Amputation | 13 | 35-66 | 13 M 0 F | Homelessness is a serious risk factor for weather exposures. Out of 13 patients, 10 considered themselves homeless; 7 out of the 13 patients required operative management. | Retrospective cohort | 2/12/21 - 4/1/21 |
| Ahmad et al. [ | Extreme cold | - | Frostbite | Wound debridement, skin grafts, and amputation | 1 | 23 | 1 M 0 F | Case of an intoxicated man who developed frostbite after walking without shoes in freezing weather. | Case report | - |
| Boles et al. [ | Extreme cold | 1/2007 - 4/2017 | Frostbite | Skin graft, escharotomy, and amputation | 47 | 15 (medium) | 24 M 23 F | Frostbite in children was tied to lack of supervision and alcohol use, with risks rising at temperatures below −6°C. | Retrospective cohort | 1/2007 - 4/2017 |
| Roche-Nagle et al. [ | Extreme cold | - | Frostbite, hemorrhagic blistering, and sepsis | Bilateral below-knee amputations | 1 | 47 | 1 M 0 F | Frostbite case report emphasized varied causes of injury (social, occupational, recreational) and importance of clinical management knowledge. | Case report | - |
| Xiao et al. [ | Extreme cold | 1/2009 - 1/2019 | Frostbite | Amputation | 27 | 14 to 81 | 23 M 4 F | Pilgrimage is an essential and sacred ritual for Tibetan Buddhists. Nonstop travel without proper shelter risks exposures to extreme weather patterns such as blizzards. | Retrospective cohort | 1/2009 - 1/2019 |
| Xiao et al. [ | Extreme cold | 12/20/2018 | Frostbite with mummified gangrene | Bilateral amputation | 1 | 18 | 0 M 1 F | Case of an 18-year-old exposed to a blizzard during a pilgrimage, developed cold mummified gangrene that resulted in amputation. Treatment complicated by language barriers, ethnic tensions, and lack of education on frostbite. | Case report | - |
| Endorf et al. [ | Extreme cold | 2016-2018 | Frostbite | Amputation | 7560 | 51.5 | 6040 M 1520 F | Black race, homelessness, and substance use were linked to increased frostbite incidence and higher amputation rates. | Retrospective database analysis | 2016-2018 |
| Zhang et al. [ | Extreme cold | 10/1986 - 10/1991 | Injuries from electric saw, cutting, punching, avulsion, pounding, and crush resulting | Multiple digit replantation, blood vessel and nerve repair, and amputation | 130 | 2 to 58 | 102 M 28 F | Multiple-digit replantation had positive outcomes (94% survival rate). Conditions permitting, all fingers should be replanted. Warming of the frozen digit is recommended prior to debridement and replantation. | Case series | 10/1986 - 10/1991 |
| Buckle et al. [ | Hurricane | 8/25/2017 - 9/22/2017 | Open fracture with soft tissue damage | Wound debridement (followed by multiple plastics procedures due to resistant infection): tissue expansion & wound closure, full thickness rotational flap, split thickness skin graft | 1 | 25 | 1 M 0 F | Water-exposed open fractures in disaster settings require intensive debridement and infection prevention. Primary wound closure can lead to high rates of serious infections. | Case report | 8/25/2017 - 9/22/2017 |
| Mellgard et al. [ | Hurricane | 2017 | Stump ulceration with distal necrotic tissue | - | 1 | 59 | 1 M 0 F | Natural disasters do not fall within state boundaries or territory lines, but Medicare coverage can vary substantially. This patient's case from Puerto Rico illustrates the difficulty to assure continuity of care after Hurricane Maria. | Case report | 2017 |
| Muñoz-Torres et al. [ | Hurricane | 12/2019 - 3/2021 | Increased breast cancer risk | Breast cancer reconstruction | 241 | 62.6 (mean) | 19 M 80 F | Cancer care delays due to natural disasters were worsened by regional disparities in Puerto Rico. | Cross sectional | 12/2019 to 3/2021 |
| Langdon et al. [ | Landslide | 1/2018 | Skin and soft tissue injury, craniofacial trauma, corneal abrasion/eye irritation, orthopedic injury, pelvic fracture, spinal fracture, scapula fracture, mud impaction, burns, traumatic brain injury, wound infection, acute kidney injury | Soft tissue irrigation and debridement, wound vacuum therapy, skin graft, internal fixation of fractures, ligament/tendon repair, and body orifice irrigation | 24 | 52.5 (median) | 10 F 13 M | Debris flow syndrome is a pattern of injuries including soft tissue injuries, hypothermia, craniofacial trauma, corneal abrasions, orthopedic injuries, and mud impaction that occur after a debris flow. | Retrospective cohort | 1/2018 |
| Arango-Granados et al. [ | Landslide | - | Crush injury | Fasciotomy, above knee amputation | 1 | 29 | 1 M 0 F | Case of a patient under a landslide for 50 hours who benefited from early amputation due to progressive deterioration. | Case report | - |
| Carvalho et al. [ | Landslide | - | Fractures, crush injury and soft tissue injury | Fracture fixation, soft tissue reconstruction, and amputation | 11 | 1 in 20s-30s, 2 in 30s-40s, 4 in 40s-50s, 2 in 50-60s, 2 in 60s-70s | 3 M 8 F | Rehabilitation after landslides was underused due to competing needs, limited access, and knowledge of such resources. | Cross sectional | - |
| Austin et al. [ | Tornado | - | Burns and soft tissue injury | Wound debridement and skin grafting | 4 | 50, 48, 17 | 2 M 2 F | Fungal burn infections have increased 10x since 1960s; survival improves with combined surgical and antifungal treatment. | Case series | - |
| Hartmann et al. [ | Tornado | 4/27/2011-4/28/2011 | Soft tissue injury, orthopedic injury, brain hemorrhage, and abdominal and thoracic injury | Laparotomy, craniotomy, soft tissue reconstruction, orthopedic fixation, thoracostomy, thoracotomy, split-thickness skin graft, BKA, splenic embolization, dilation and curettage | 28 | 21-87 | 16 M 12 F | Following a tornado, the main surgical interventions performed included soft tissue debridement and reconstruction, as well as orthopedic fixation. | Retrospective cohort | 4/27/2011-4/28/2011 |
| May et al. [ | Tornado | 5/1999 | Soft tissue injury, soft tissue infection and contamination, head injuries (scalp lacerations and contusions, concussions, skull fracture, intracranial bleeding), fractures, dislocations, blunt abdominal and chest trauma, and penetrating trauma | Wound debridement, soft tissue reconstruction, fracture fixation, and neurosurgery | 147 | 35.7 (estimated mean based on a subset of patients whose ages were recorded) | 67 M 79 F 1 unspecified | This single-site experience of care for tornado-related injuries suggests complex soft tissue wounds, head injuries, and fractures are most common. | Retrospective review | 5/1999 |
| Chern et al. [ | Tornado | 4/27/11 - 4/28/11 | Cranial, spine, and peripheral nerve injuries | Craniectomy, EVD placement, bedside scalp closure | 24 | 1 month - 14 years | - | Within the first 24 hours post-tornado, 24 pediatric patients received neurosurgical care with 15 undergoing surgery. | Retrospective Cohort | 4/27/11 - 4/28/11 |
| Ozaki et al. [ | Typhoon | 2019 | Skin infection | Would care (surgical drainage tube) | 1 | 80 | 0 M 1 F | Case of an 80-year old post operative breast cancer patient highlights how risks including cancer diagnosis, post-operative status, and advanced age increase the likelihood of skin infection following immersion in flood waters. | Cross-sectional | 2019 |
| Kaneda et al. [ | Typhoon | 4/2019 - 9/2021 | Increased breast cancer risk | Mastectomy and axillary dissection, and breast reconstruction | 1 | 50s | 0 M 1 F | Case of a Japanese woman showing signs of breast cancer; however, intervention was delayed due to Typhoon Hagibis and the COVID-19 pandemic. | Retrospective cohort | 4/2019 - 9/2021 |
| Selvaggi et al. [ | Ball lightning | - | Burns | Surgical debridement and coverage with a split-thickness skin graft | 2 | 28, 5 | 1 M 1 F | Ball lightning, a mixture of fire and electricity, caused fire and electrical burns in a father and daughter. Both recovered following medical and surgical burn treatment within 43 days. | Case control | - |
| Laohawiriyakamol et al. [ | Snake bite | 1/1999 - 12/2008 | Soft tissue injury and compartment syndrome | Serial wound debridement, skin grafting, fasciotomy due to compartment syndrome, cutaneous resurfacing, toe amputation due to necrosis | 58 | 2-3 yrs | 43 M 15 F | Snake bites are common in children in developing countries. The majority occurred in the summer and rainy seasons (Feb-August), especially during floods. | Case series | 1/1999 - 12/2008 |
| Lee et al. [ | Unspecified | 2000 - 2011 | Crushing, fracture, and internal organ rupture | - | 642 | 51.56 (mean) | 400 M 242 F | Deaths from natural disastersdisproportionately affected agricultural workers. | Case report | 2000 - 2011 |
| Naidu et al. [ | Unspecified | 1/1/2008 - 12/31/2017 | Limb injury | Limb amputation | 936 | 27 (median) | 706 M 230 F | Humanitarian crises are associated with increased rates of limb amputations. | Retrospective cohort | 1/1/2008 - 12/31/2017 |
| Plastic Surgery Specialty | Percentage of Studies Inclusive of Each Specialty | Climate Event | Plastic Surgery-Specific Indication | Plastic Surgery-Specific Intervention |
| General Reconstruction | 31.4% | Extreme heat | Dry necrosis | Flap, wound debridement, skin grafting [ |
| Winter storm | Frostbite | Wound debridement and drainage [ | ||
| Landslide | Soft tissue injury | Soft tissue reconstruction [ | ||
| Skin & soft tissue injury and infection | Wound irrigation & debridement, wound vacuum therapy, skin grafting [ | |||
| Crush injury | Fasciotomy [ | |||
| Tornado | Soft tissue injury | Soft tissue reconstruction [ | ||
| Skin grafting [ | ||||
| Soft tissue infection | Wound debridement [ | |||
| Hurricane | Stump ulceration with necrotic tissue [ | N/A | ||
| Typhoon | Skin infection | Surgical wound care & drainage [ | ||
| Snake bite | Soft tissue injury, compartment syndrome | Wound debridement, skin grafting, fasciotomy, cutaneous resurfacing [ | ||
| Water pollution | Skin cancer | Surgical resection [ | ||
| Hand & Lower Extremity | 62.9% | Air pollution | Diabetic foot injury | Lower limb amputation [ |
| Wildfire | Burns | Amputation [ | ||
| Extreme heat | Dry necrosis | Amputation [ | ||
| Musculoskeletal and soft tissue injury | Amputation [ | |||
| Winter storm | Frostbite | Amputation [ | ||
| Extreme cold | Frostbite | Amputation [ | ||
| Frostbite, hemorrhagic blistering, sepsis | Amputation [ | |||
| Blunt trauma, crush, avulsion injuries | Amputation, multiple digit replantation, blood vessel & nerve repair [ | |||
| Hurricane | Open fracture | Wound debridement, tissue expansion & wound closure, flap, skin grafting [ | ||
| Landslide | Crush injury | Amputation [ | ||
| Fractures | Fracture fixation [ | |||
| Tendon/Ligament damage | Tendon/Ligament repair [ | |||
| Tornado | Fractures | Fracture fixation [ | ||
| Musculoskeletal and soft tissue injury | Amputation [ | |||
| Snakebite | Soft tissue injury | Toe amputation [ | ||
| Mixed climate events | Limb injury | Limb amputation [ | ||
| Crushing, fractures | N/A [ | |||
| Craniofacial | 11.4% | Air pollution | Non-syndromic cleft lip and palate | Cleft lip and palate repair [ |
| Landslide | Craniofacial trauma | Internal fracture fixation, facial reconstruction [ | ||
| Tornado | Head and scalp injuries | Facial reconstruction [ | ||
| Scalp closure [ | ||||
| Burn | 22.9% | Wildfire | Burns | Skin grafting [ |
| Wound debridement, surgical excision [ | ||||
| Escharotomy [ | ||||
| Extreme heat | Burns | Wound debridement, skin grafting, and surgical excision [ | ||
| Ball lightning | Burns | Wound debridement and skin grafting [ | ||
| Tornado | Burns | Wound debridement and skin grafting [ | ||
| Extreme cold | Frostbite | Escharotomy [ | ||
| Wound debridement [ | ||||
| Skin grafting [ | ||||
| Breast Reconstruction | 8.6% | Air pollution | Increased breast cancer risk | Breast reconstruction [ |
| Hurricane | Increased breast cancer risk | Breast reconstruction [ | ||
| Typhoon | Increased breast cancer risk | Breast reconstruction [ |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClimate Change and Health Impacts · Disaster Response and Management · Burn Injury Management and Outcomes
Introduction and background
Climate change is a timely issue that hardly spares any part of society, and the healthcare system is no exception. In 2023, indicators of climate change revealed a consternating reality despite international attempts to counteract its unmitigated progression [1]. Compared to the pre-industrial baseline, the mean annual temperature had reached a record high, extreme precipitation had increased in 61% of the global land, and heat-related mortality of people older than 65 years increased by 167%, an unprecedented figure [1]. This intensification of climate change has been increasing the burden on the healthcare system, which has in part been attributed to the spread of infectious diseases [2,3] and the rise in chronic illnesses [4-6], mental health disorders [7], and heat-related mortality [8]. These examples are, however, by no means comprehensive as the far-reaching effects of climate change on human health remain an ongoing area of study.
A direct mechanism by which climate change results in health care needs is natural disasters. Some natural disasters, such as tropical cyclones, floods, droughts, wildfires, and polar vortexes, are intimately associated with climate change, as rising global temperatures can perturb the stability of the Earth’s atmosphere, which can give rise to such extreme weather conditions [9]. These climate-related natural disasters are capable of wreaking havoc, damaging infrastructure, inducing prolonged power outages, and causing victims injuries and trauma [10], leaving in their wake dire medical needs that must be addressed with a prompt and concerted response led at least partly by the healthcare system. Consistent with the potential devastation, prior studies have identified that climate-related natural disasters are followed by a surge in the use of medical care [11], including surgical interventions [12].
A significant fraction of the aforementioned surgical needs may fall under the scope of plastic and reconstructive surgery. The injuries that arise may require reconstruction and persistent surgical wound management [13]. As climate-related natural disasters are projected to become increasingly far-reaching in the foreseeable future [1], their relationship with the demand for plastic and reconstructive surgeries may be an important area of investigation that further defines surgeons’ stakes in climate change, informs the kinds of surgical needs that may become more commonplace, and contributes to the planning of more comprehensive disaster response.
Thus, our scoping review attempts to achieve the following objectives: (i) provide a map of the current literature on the need for plastic and reconstructive surgeries following climate-related natural disasters, (ii) underscore specific mechanisms of injury requiring such surgical interventions that are becoming more prominent due to climate-related natural disasters, (iii) describe the complexities of socioeconomic and geographic variables at play, and (iv) identify the gaps in the literature.
Review
Methods
Search Strategy
We registered our search protocol in Open Science Framework (OSF registration number: 10.17605/ OSF.IO/RP9HE) prior to starting this review. In addition to following the methods for scoping reviews described by Peters et al. in 2020 [14], our search strategy adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)-ScR reporting guidelines [15]. Studies were identified by searching PubMed (National Center for Biotechnology Information), Embase (Elsevier, embase.com), Global Health (C.A.B. International, EBSCOhost), and Web of Science Core Collection (Clarivate) on March 4, 2025. Controlled vocabulary terms (i.e., MeSH, Emtree, and CABI Thesaurus) were included when available and appropriate. The search strategies were designed and carried out by a health sciences librarian (CM). The exact search terms used in each of the databases are provided in the supplementary document (Appendix 1).
Inclusion Criteria
All original research articles discussing plastic surgical procedures associated with climate-related natural disasters and extreme weather events were included. Only English articles were included. No publication date limits were applied.
Exclusion Criteria
Studies that lacked primary data, did not include a clear climate-related weather or pollution event, and were published outside our authors’ native fluency were excluded. Studies that focused exclusively on earthquakes, tsunamis, and volcanoes were also excluded due to a lack of a well-established link with climate change.
Study Selection and Data Extraction
All articles were uploaded to Covidence systematic review software (Veritas Health Innovation Ltd., Melbourne, Australia); duplicate records were removed during the import process. Two independent reviewers screened each title and abstract to identify studies for full-text review. Of the articles that passed the abstract and title screening, we carefully reviewed the full text of each article to identify relevant studies for inclusion in our analysis. Conflicts between reviewers were resolved by discussion in all stages of screening. With our final cohort of included studies, we extracted data using pre-specified parameters including study type, weather event, date of weather event, type of injury, type of surgical intervention, total number of patients, patient age, patient sex, climate-related study findings, economic implications, duration of study period, country, and U.S. state when applicable. The full data extraction table is included in Appendix 2.
Limitations
This scoping review was conducted in accordance with the PRISMA-ScR guidelines to map the breadth of the existing evidence, rather than to evaluate the effectiveness of specific interventions or to generate quantitative summary estimates. In line with current methodological guidance for scoping reviews, we did not conduct a formal risk-of-bias or methodological quality assessment of the included studies.
Data Analysis
We generated descriptive statistics and figures using Python, Excel, Word, and PowerPoint. Given the nature of a scoping review, we did not conduct any further meta-analyses.
Ethics Approval
Institutional Review Board approval and oversight were not required for our study as we did not work with any human subjects as part of this research.
Results
Study Characteristics
A total of 1,538 records were identified by the literature searches. One thousand fifteen unique records were available for screening after removal of duplicates. We excluded 906 articles during the title and abstract screening and an additional 73 articles following the full-text screening. In total, we included 35 studies in our final analysis (Figure 1).
PRISMA Flow Diagram of the Scoping Review Process.PRISMA: Preferred Reporting Items for Systematic Reviews and Meta-Analyses
Relevant study characteristics and findings of our included studies (n=35) are summarized in Table 1. The most commonly included studies in our analysis were case reports and case series (n=17, 48.6%). The next most common study types were retrospective cohort studies (n=9, 25.7%), retrospective observational studies (n=4, 11.4%), and cross-sectional studies (n=3, 8.6%).
Temporal and Geographic Distribution of Studies
There was an increase in climate-related studies over time, with the majority of studies (n= 20, 57.1%) being published between 2015-2020 alone (Figure 2). Referencing the World Bank’s income group classification system, we found that the majority of studies were published in high-income countries (HICs) (n=26, 74.3%), followed by upper-middle-income countries (UMIC) (n=6, 17.1%), lower-middle-income countries (LMICs) (n=2, 5.7%), and low-income countries (LICs) (n=1, 2.9%) (Appendix 3). Within the U.S., we also categorized studies by the individual states and territories impacted by natural disasters, extreme weather, or pollution. Texas (n=4, 11.4%), California (n=3, 8.6%), and New York (n=3, 8.6%) had the highest number of published studies describing a climate event in the region (Appendix 2). There was one study that included all 50 U.S. states in a retrospective database analysis of extreme cold (Appendix 2).
Incidence of Climate-Related Studies Over TimeThe figure displays the number of studies meeting our inclusion criteria published each year per climate event.
Incidence of Climate Events Reported
The included studies reported on a range of climate-related natural disasters and extreme weather events, including hurricanes (n=3, 8.6%), tornados (n=4, 11.4%), landslides (n=3, 8.6%), typhoons (n=2, 5.7%), wildfires (n=3, 8.6%), air pollution (n=3, 8.6%), winter storms (n=2, 5.7%), extreme heat (n = 3, 8.6%), and extreme cold (n = 7, 20.0%) (Table 1). Each climate event type was associated with various plastic surgery indications and interventions, as outlined in Table 2.
Plastic and Reconstructive Surgery Interventions
When summarizing the studies, if a paper reported on interventions that applied to more than one plastic surgery subspecialty, we counted that study separately in each relevant category. Among plastic surgery subspecialties, hand and lower extremity surgery was most indicated after an acute weather event (n=22, 62.9%), with common procedures including amputation, wound closure, digit replantation, and nerve repair (Table 2). General reconstruction was also highly indicated (n=11, 31.4%) in our study cohort, as soft tissue reconstruction, skin grafts and flaps, and wound debridement were frequently performed (Table 2). Burn care (n=8, 22.9%) following wildfires, extreme heat, and lightning strikes required interventions such as wound debridement, skin graft, and escharotomy (Table 2). Additional plastic surgery indications included craniofacial (n=4, 11.4%) and breast reconstruction (n=3, 8.6%) (Table 2).
Discussion
Although disaster medicine is an entire specialty of its own, this review elucidates the lesser-described impact of climate events on plastic and reconstructive surgery to raise awareness of disaster preparedness in this field. As these events will only become more severe and commonplace in the future - and as population centers located in susceptible areas are increasingly affected - policy actions and infrastructure reinforcements should also be enacted to mitigate these effects. Our study also highlights the geographic, economic, and social factors that exacerbate the burdens of both injury and surgical care.
Geographic Disparities
Despite the large majority of studies being published in HICs (n=26, 74.3%), with the United States alone comprising over a third of the included studies (n=12, 34.3%), the impact of natural disasters is felt throughout the world and disproportionately affects under-resourced nations, due to both their pre-event vulnerability and post-event response [51]. According to a report by the United Nations Office for Disaster Risk Reduction, 90.7% of deaths caused by natural disasters between 1996 and 2015 occurred in low- and middle-income countries [52]. Studies focusing on these countries (UMIC, LMIC, LIC) only comprised 25.7% of the included literature on this topic, which may demonstrate not only their underlying vulnerability to climate events, but also the lack of resources and literature to bolster disaster response in these areas (Figure 3a).
Geographic Distribution of Included Studies(A) World Map showing geographic distribution of climate events in the included studies. Countries shaded in gray had no climate event studies that fit our inclusion criteria. (B) U.S. State Map showing geographic distribution of climate events in the United States present in the included studies. The baseline level of n=1 represents a national U.S. study.
Within the United States, state-level trends were also observed (Figure 3b). Texas had the highest number of included studies (n=4), which examined air pollution, winter storms, extreme cold, and hurricanes. Notably, there were more studies on Texas (n=4) than all low-income and lower middle-income countries combined (n=3). States in the Midwest and Mountain West had the fewest included studies, despite being notably affected by a range of climate events such as wildfires, severe storms, air pollution, and extreme temperatures.
Socioeconomic Considerations
Lower-income individuals are generally most affected by climate events. For instance, frostbite is exacerbated by inadequate shelter, prolonged cold exposure, and community infrastructure. A single-center analysis in San Antonio, Texas examined 13 patients with frostbite impacted by the 2021 Winter Storm Uri, of which 10 (76.9%) were experiencing homelessness. This already-vulnerable population also had limited experience with the extreme cold, which may have led to their 3-day median delay in seeking treatment [27]. In a 2017 case report by Mellgard et al., a Puerto Rican patient who had developed stump ulceration with distal necrotic tissue experienced delayed care after Hurricane Maria due to managed Medicare coverage gaps in Puerto Rico [36]. Natural disasters can thereby compromise the continuity of care despite federal insurance programs and exacerbate existing socioeconomic disparities.
This study also identifies how climate events can create an increased cost burden on healthcare systems more broadly. A case series on extreme heat in the UK showed that pavement burns, a new mechanism of injury becoming more common with climate change, result in longer hospital stays and more intensive surgical intervention compared to similarly-sized traditional burns [23]. As such, contact pavement burns require more resources, resulting in a greater cost per surface area burned. Moreover, a retrospective cohort study in Australia showed that worker compensation claims rose 6.2% during heatwaves, given the increase in occupational burns, wounds, lacerations, and amputations that were especially prevalent among older male workers [25].
Other sociodemographic determinants of injury associated with climate events were also found. For example, of 13 Tibetan Buddhist patients examined in a retrospective cohort study in China, pilgrimage was overwhelmingly responsible for frostbite (n=9, 69.2%), as the endurance of extreme conditions was a sign of religious devotion [31].
These geographic, social, and economic factors have all been compounded by the increasing occurrence and severity of climate events. The majority of included studies (n= 20, 57%) were published between 2015-2020, likely reflecting not just the rising interest in studying the implications of climate change, but also the growing impact of natural disasters on our lives, and especially on those who are the most vulnerable (Figure 2).
Indirect Health Impacts
This review also shines light on both the direct and indirect impacts of climate events on the occurrence and management of cancer. A 2025 study in Maryland showed that chronic exposure to air pollution and particulate matter mediate inflammatory processes that may increase the risk of breast cancer [17]. Likewise, a 2018 study in Bangladesh demonstrated that populations exposed to water pollution had a significantly higher prevalence of mucocutaneous skin lesions that can lead to skin cancer [19]. Coastal regions and countries susceptible to heavy flooding, storms, and water pollution may have an increased oncological burden that may not be immediately obvious.
The delayed care and surgical intervention of patients with chronic diseases and cancer as a consequence of natural disasters is another indirect effect that cannot be understated. A 2024 cross-sectional study by Muñoz-Torres et al. found that cancer care delays in Puerto Rico were worsened due to climate events, leading to increased oncological risk and fewer resources for procedures such as breast reconstruction [37]. In addition, a 2022 study in Japan found that a woman with signs of breast cancer had time-sensitive interventions delayed due to Typhoon Hagibis and the COVID-19 pandemic, leading to distant bone metastases [46].
Importantly, this study identified associations between various climate events, socioeconomic and geographic risk factors, mechanisms of injury, and surgical interventions to promote awareness among plastic and reconstructive surgeons. Improving emergency preparedness in the coming years will be especially necessary as weather events are predicted to increase in frequency and severity.
Future Directions & Policy Implications
Our findings demonstrate a global need for more disaster-related education and disaster response. Already, plastic and reconstructive surgeons in Florida have launched the Surgeon Aftercare during Emergencies (SAfE) initiative after witnessing the devastating impact of local hurricanes that displace many patients and disrupt medical practices [53]. This SAfE initiative intends to provide post-operative care to patients during emergency situations using an accessible network of volunteer surgeons [53]. In LMIC and LIC countries that are most vulnerable to the effects of these disasters, national and global plastic surgery networks can be particularly crucial in organizing a coordinated medical response after a climate event. Training the healthcare workforce to better address the surgical demand in disaster-prone areas, as well as establishing a registry for weather and disaster related injuries, will be critical in ensuring future preparedness.
Limitations
There were a number of limitations in this study. First, our selection of only studies written in English likely led to the exclusion of several studies from low- and middle-income countries, and there were no studies from Africa that met our inclusion criteria. As such, certain climate events and surgical interventions may be over- or under-represented. In addition, eight of the studies that we excluded examined the 2004 Indian Ocean earthquake and tsunami that hit Southeast Asia, and there was no other single disaster with as many studies that reported on its health impacts. Many of the affected countries were middle income countries, such as Indonesia, Sri Lanka, and Thailand. Furthermore, while not the primary focus of our study, it is difficult to quantify the delayed health impacts of a natural disaster, although we did consider the delays in surgery for non-emergent procedures that increase the risks of cancer and chronic disease progression. Overall, these findings help characterize the impact of weather events as a result of climate change on the field of plastic surgery.
Conclusions
Climate-related natural disasters and extreme weather are producing surges in demand for certain plastic and reconstructive surgeries, such as general reconstruction, upper and lower extremity surgeries, craniofacial surgeries, burn care, and breast reconstruction. This is partly due to increasing immediate trauma burden, followed by a delay in routine care and screenings that may, in turn, increase the need for future operations, such as breast cancer surgeries. Thus, the complex relationship between the rising threat of climate-related natural disasters and plastic and reconstructive surgery is a timely and relevant area of research that warrants further investigation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The 2024 report of the Lancet Countdown on health and climate change: facing record-breaking threats from delayed action Lancet Romanello M Walawender M Hsu SC 1847189640420243948822210.1016/S 0140-6736(24)01822-1PMC 7616816 · doi ↗ · pubmed ↗
- 2Climate change-related migration and infectious disease Virulence Mc Michael C 548553620152615122110.1080/21505594.2015.1021539 PMC 4720222 · doi ↗ · pubmed ↗
- 3The impact of increasing temperatures due to climate change on infectious diseases BMJ Anikeeva O Hansen A Varghese B Borg M Zhang Y Xiang J Bi P 0387202410.1136/bmj-2024-07934339366706 · doi ↗ · pubmed ↗
- 4Role of climate change in urologic health: kidney stone disease Eur Urol Focus Spiardi R Goldfarb DS Tasian GE 866868920233783997510.1016/j.euf.2023.10.001 · doi ↗ · pubmed ↗
- 5Climate change effects on respiratory health: implications for nursing J Nurs Scholarsh George M Bruzzese JM Matura LA 6446524920172880646910.1111/jnu.12330 · doi ↗ · pubmed ↗
- 6Climate change and kidney disease-threats and opportunities Kidney Int Barraclough KA Blashki GA Holt SG Agar JW 5265309220172880725610.1016/j.kint.2017.03.047 · doi ↗ · pubmed ↗
- 7The effects of climate change on mental health Dtsch Arztebl Int Walinski A Sander J Gerlinger G Clemens V Meyer-Lindenberg A Heinz A 11712412020233664758410.3238/arztebl.m 2022.0403 PMC 10154789 · doi ↗ · pubmed ↗
- 8Climate change and heat-related excess mortality in the eastern USA Ecohealth Limaye VS Vargo J Harkey M Holloway T Patz JA 4854961520183015965110.1007/s 10393-018-1363-0PMC 6572724 · doi ↗ · pubmed ↗