Risk of Hospital Readmissions and Association With Receipt of Post‐Hospitalization Care Coordination Services Among High‐Risk Veterans
Diana J. Govier, Meike Niederhausen, Alex Hickok, Mazhgan Rowneki, Holly McCready, Abby Moss, Kristina M. Cordasco, Kathryn M. McDonald, Matthew L. Maciejewski, Kathleen C. Thomas, Denise M. Hynes

TL;DR
This study found that post-hospital care coordination did not significantly reduce readmission rates among high-risk Veterans, suggesting the need for better interventions.
Contribution
The study provides new evidence on the limited impact of post-hospital care coordination on reducing readmissions in high-risk Veterans.
Findings
Post-hospital care coordination was not associated with a significant reduction in 30-day all-cause readmissions.
There was no significant difference in ambulatory care sensitive condition readmissions between groups.
Alternative or additional services may be needed to address readmissions in high-risk Veterans.
Abstract
To examine associations between receipt of post‐hospitalization care coordination and VA‐delivered, VA‐purchased, and Medicare fee‐for‐service hospital readmissions among Veterans at high risk for hospitalization and/or mortality. In this observational retrospective cohort study, we compared high‐risk Veterans who received care coordination within one day after hospital discharge (“treated”) with up to five matched high‐risk Veterans who did not receive care coordination during this time (“comparators”). Competing risk models estimated adjusted sub‐hazard ratios (aSHR) for 30‐day all‐cause and ambulatory care sensitive condition (ACSC) readmissions between treated and comparators, with death as a competing risk. In sensitivity analyses, we implemented inverse probability of censoring weights to account for censoring due to cross‐over to treatment among comparators during follow‐up.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
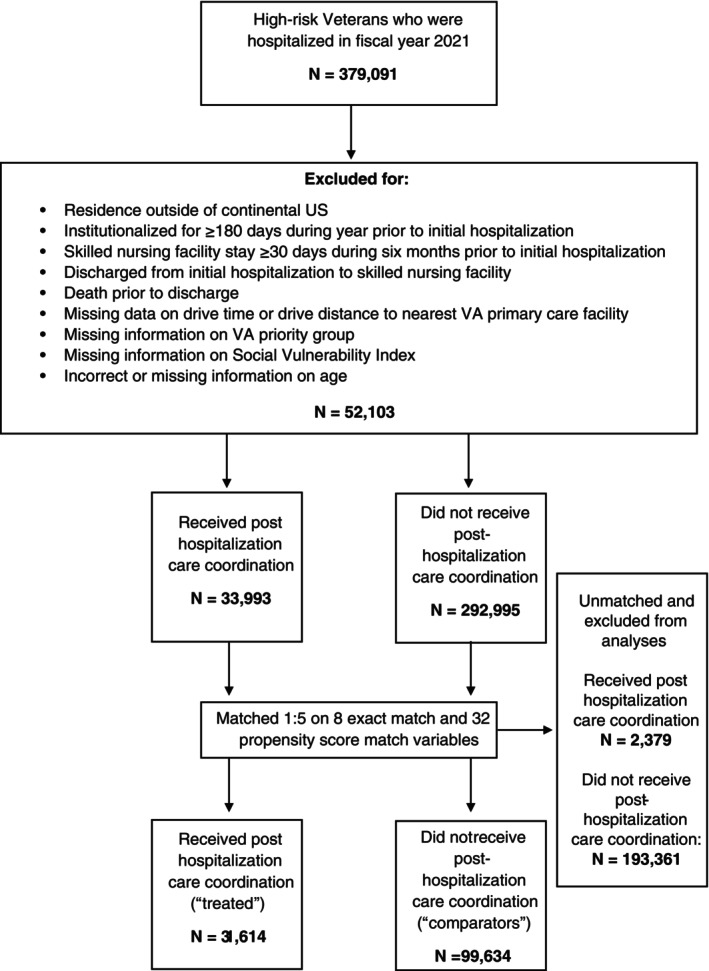 FIGURE 1
FIGURE 1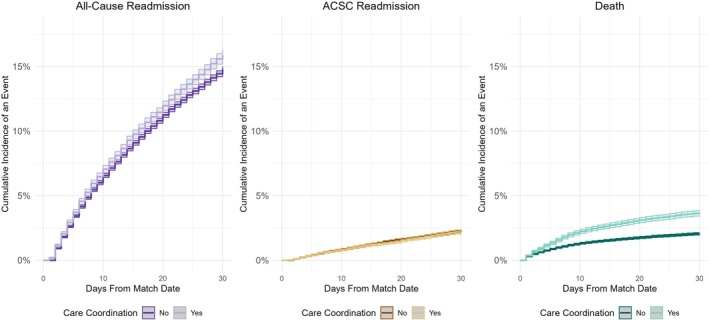 FIGURE 2
FIGURE 2| Post‐hospitalization care coordination status | |||||||
|---|---|---|---|---|---|---|---|
| Characteristic | Overall ( | Overall (% or SD) 100% | No ( | No (% or SD) 76% | Yes ( | Yes (% or SD) 24% | SMD |
| Sex, no. (%) | 0.05 | ||||||
| Female | 4519 | 3.4 | 3198 | 3.2 | 1321 | 4.2 | |
| Male | 126,729 | 96.6 | 96,436 | 96.8 | 30,293 | 95.8 | |
| Age group (years), no. (%) | 0.06 | ||||||
| < 45 | 3757 | 2.9 | 2698 | 2.7 | 1059 | 3.4 | |
| 45–64 | 33,681 | 25.7 | 25,587 | 25.7 | 8094 | 25.6 | |
| 65–74 | 52,477 | 40.0 | 40,148 | 40.3 | 12,329 | 39.0 | |
| 75–84 | 27,449 | 20.9 | 20,936 | 21.0 | 6513 | 20.6 | |
| 85+ | 13,884 | 10.6 | 10,265 | 10.3 | 3619 | 11.5 | |
| Mean CAN score category 1‐year pre‐hospitalization, no. (%) | 0.06 | ||||||
| (3, < 81.6) | 27,498 | 21.0 | 21,266 | 21.3 | 6232 | 19.7 | |
| (81.6, < 88.3) | 27,550 | 21.0 | 21,131 | 21.2 | 6419 | 20.3 | |
| (88.3, < 94.5) | 33,061 | 25.2 | 25,106 | 25.2 | 7955 | 25.2 | |
| (94.5, 99) | 43,139 | 32.9 | 32,131 | 32.3 | 11,008 | 34.8 | |
| Veteran's assigned VA facility is a CCICM early adopter site, No. (%) | 26,040 | 19.8 | 19,714 | 19.8 | 6326 | 20.0 | 0.01 |
| Receipt of care coordination 1‐year pre‐hospitalization, no. (%) | 59,788 | 45.6 | 43,829 | 44.0 | 15,959 | 50.5 | 0.13 |
| Discharge quarter, no. (%) | 0.01 | ||||||
| Q1 FY21 | 44,275 | 33.7 | 33,658 | 33.8 | 10,617 | 33.6 | |
| Q2 FY21 | 33,027 | 25.2 | 25,056 | 25.2 | 7971 | 25.2 | |
| Q3 FY21 | 30,475 | 23.2 | 23,037 | 23.1 | 7438 | 23.5 | |
| Q4 FY21 | 23,471 | 17.9 | 17,883 | 18.0 | 5588 | 17.7 | |
| Setting of initial hospitalization, no. (%) | 0.11 | ||||||
| Medicare FFS | 2665 | 2.0 | 2159 | 2.2 | 506 | 1.6 | |
| VA‐purchased | 11,517 | 8.8 | 9406 | 9.4 | 2111 | 6.7 | |
| VA‐delivered | 117,066 | 89.2 | 88,069 | 88.4 | 28,997 | 91.7 | |
| Race, no. (%) | 0.04 | ||||||
| American Indian/Alaska Native | 991 | 0.8 | 752 | 0.8 | 239 | 0.8 | |
| Asian | 468 | 0.4 | 372 | 0.4 | 96 | 0.3 | |
| Black/African American | 34,445 | 26.2 | 25,812 | 25.9 | 8633 | 27.3 | |
| Multiracial | 1137 | 0.9 | 850 | 0.9 | 287 | 0.9 | |
| Native Hawaiian/Pacific Islander | 859 | 0.7 | 678 | 0.7 | 181 | 0.6 | |
| White | 91,791 | 69.9 | 69,968 | 70.2 | 21,823 | 69.0 | |
| Other/unknown race identity | 1557 | 1.2 | 1202 | 1.2 | 355 | 1.1 | |
| Hispanic/latino/a/−x ethnicity, no. (%) | 0.02 | ||||||
| Non‐Hispanic/latino/a/−x | 124,617 | 95.0 | 94,488 | 94.8 | 30,129 | 95.3 | |
| Hispanic/latino/a/−x | 6631 | 5.1 | 5146 | 5.2 | 1485 | 4.7 | |
| Insurance/coverage status, no. (%) | 0.05 | ||||||
| VA only | 16,328 | 12.4 | 12,373 | 12.4 | 3955 | 12.5 | |
| VA and Medicare | 97,818 | 74.5 | 74,695 | 75.0 | 23,123 | 73.1 | |
| VA and multiple | 17,102 | 13.0 | 12,566 | 12.6 | 4536 | 14.4 | |
| VA priority group, no. (%) | 0.05 | ||||||
| Group 1 | 54,649 | 41.6 | 41,821 | 42.0 | 12,828 | 40.6 | |
| Group 2 | 6817 | 5.2 | 5181 | 5.2 | 1636 | 5.2 | |
| Group 3 | 12,322 | 9.4 | 9441 | 9.5 | 2881 | 9.1 | |
| Group 4 | 4676 | 3.6 | 3414 | 3.4 | 1262 | 4.0 | |
| Group 5 | 38,772 | 29.5 | 29,020 | 29.1 | 9752 | 30.9 | |
| Group 6 | 1579 | 1.2 | 1215 | 1.2 | 364 | 1.2 | |
| Group 7 | 3510 | 2.7 | 2652 | 2.7 | 858 | 2.7 | |
| Group 8 | 8923 | 6.8 | 6890 | 6.9 | 2033 | 6.4 | |
| Psychoses, no. (%) | 27,645 | 21.1 | 20,333 | 20.4 | 7312 | 23.1 | 0.07 |
| Depression, no. (%) | 58,821 | 44.8 | 44,151 | 44.3 | 14,670 | 46.4 | 0.04 |
| Alcohol use disorder, no. (%) | 32,497 | 24.8 | 24,150 | 24.2 | 8347 | 26.4 | 0.05 |
| Substance use disorder, no. (%) | 23,126 | 17.6 | 17,024 | 17.1 | 6102 | 19.3 | 0.06 |
| Elixhauser score, readmission, mean (SD) | 43.64 | 26.2 | 43.4 | 26.1 | 44.42 | 26.5 | 0.04 |
| COVID‐19 infection 1‐year pre‐hospitalization, no. (%) | 9395 | 7.2 | 7144 | 7.2 | 2251 | 7.1 | 0.00 |
| COVID‐19 vaccination status, no. (%) | 0.02 | ||||||
| Fully vaccinated | 42,602 | 32.5 | 32,597 | 32.7 | 10,005 | 31.7 | |
| Not fully vaccinated | 88,646 | 67.5 | 67,037 | 67.3 | 21,609 | 68.4 | |
| VA hospitalization count 1‐year pre‐hospitalization, mean (SD) | 0.5 | 1.0 | 0.5 | 1.0 | 0.5 | 1.1 | 0.03 |
| Medicare FFS hospitalization count 1‐year pre‐hospitalization, mean (SD) | 0.1 | 0.3 | 0.1 | 0.3 | 0.1 | 0.3 | < 0.01 |
| VA‐purchased hospitalization count 1‐year pre‐hospitalization, mean (SD) | 0.1 | 0.5 | 0.1 | 0.5 | 0.1 | 0.5 | 0.01 |
| All setting hospitalization count 1‐year pre‐hospitalization, mean (SD) | 0.6 | 1.3 | 0.6 | 1.3 | 0.7 | 1.3 | 0.02 |
| VA primary care visit count 1‐year pre‐hospitalization, mean (SD) | 11.3 | 9.2 | 11.3 | 9.0 | 11.3 | 9.7 | < 0.01 |
| VA mental health care visit count 1‐year pre‐hospitalization, mean (SD) | 8.3 | 19.9 | 7.5 | 18.3 | 10.8 | 23.9 | 0.15 |
| VA specialty care visit count 1‐year pre‐hospitalization, mean (SD) | 25.8 | 17.3 | 25.7 | 17.0 | 26.0 | 18.2 | 0.01 |
| VA reliance, mean (SD) | 0.9 | 0.2 | 0.9 | 0.2 | 0.9 | 0.2 | 0.01 |
| Urban or rural residence, no. (%) | 0.03 | ||||||
| Urban | 94,859 | 72.3 | 71,699 | 72.0 | 23,160 | 73.3 | |
| Rural/highly rural | 36,389 | 27.7 | 27,935 | 28.0 | 8454 | 26.7 | |
| Residence in PC‐HPSA, no. (%) | 34,378 | 26.2 | 26,737 | 26.8 | 7641 | 24.2 | 0.06 |
| Residence in MH‐HPSA, no. (%) | 41,961 | 32.0 | 32,955 | 33.1 | 9006 | 28.5 | 0.10 |
| Drive time to nearest VA (minutes), no. (%) | 0.04 | ||||||
| 0–10 | 40,337 | 30.7 | 30,290 | 30.4 | 10,047 | 31.8 | |
| 11–20 | 49,822 | 38.0 | 37,773 | 37.9 | 12,049 | 38.1 | |
| 21–30 | 21,589 | 16.5 | 16,542 | 16.6 | 5047 | 16.0 | |
| > 30 | 19,500 | 14.9 | 15,029 | 15.1 | 4471 | 14.1 | |
| Drive distance to VA (miles), no. (%) | 0.05 | ||||||
| 0–5 | 38,715 | 29.5 | 28,960 | 29.1 | 9755 | 30.9 | |
| 6–10 | 33,205 | 25.3 | 25,144 | 25.2 | 8061 | 25.5 | |
| 11–20 | 32,833 | 25.0 | 25,025 | 25.1 | 7808 | 24.7 | |
| 21–40 | 20,561 | 15.7 | 15,899 | 16.0 | 4662 | 14.8 | |
| > 40 | 5934 | 4.52 | 4606 | 4.6 | 1328 | 4.2 | |
| SVI, socioeconomic status, mean (SD) | 0.6 | 0.3 | 0.6 | 0.3 | 0.6 | 0.3 | 0.06 |
| SVI, household characteristics, mean (SD) | 0.5 | 0.3 | 0.5 | 0.3 | 0.5 | 0.3 | 0.04 |
| SVI, racial and ethnic minority status, mean (SD) | 0.7 | 0.3 | 0.7 | 0.2 | 0.7 | 0.3 | 0.03 |
| SVI, housing type and transportation, mean (SD) | 0.6 | 0.2 | 0.6 | 0.2 | 0.6 | 0.2 | 0.01 |
| County long‐term care bed count, mean (SD) | 4740.6 | 7913.7 | 4756.7 | 7999.3 | 4689.8 | 7637.5 | 0.01 |
| County hospital bed count, mean (SD) | 2841.5 | 4367.8 | 2853.1 | 4370.9 | 2805.2 | 4357.9 | 0.01 |
| Length of initial hospitalization (days), no. (%) | 0.14 | ||||||
| 1 | 31,907 | 24.3 | 24,844 | 24.9 | 7063 | 22.3 | |
| 2 | 24,190 | 18.4 | 18,839 | 18.9 | 5351 | 16.9 | |
| 3–7 | 53,622 | 40.9 | 40,790 | 40.9 | 12,832 | 40.6 | |
| 8–14 | 14,902 | 11.4 | 10,671 | 10.7 | 4231 | 13.4 | |
| 15+ | 6627 | 5.1 | 4490 | 4.5 | 2137 | 6.8 | |
| Primary diagnosis of COVID‐19 for initial hospitalization, no. (%) | 9988 | 7.6 | 7596 | 7.6 | 2392 | 7.6 | < 0.01 |
| Outcome | Cumulative incidence | ||||||
|---|---|---|---|---|---|---|---|
| Overall | Post‐hospitalization care coordination status | Unadjusted percentage point difference | Adjusted subhazard ratio (aSHR) | ||||
|
| Yes | No | Estimate | 95% CI | Estimate | 95% CI | |
| All‐cause readmission | 14.1% | 15.9% | 13.5% | 2.36 | 1.91, 2.82 | 1.03 | 1.00, 1.07 |
| ACSC readmission | 2.1% | 2.3% | 2.1% | 0.17 | −0.02, 0.36 | 0.97 | 0.89, 1.05 |
| Death | 2.4% | 3.7% | 1.9% | 1.76 | 1.53, 1.98 | 1.85 | 1.72, 2.00 |
| Subgroup & Outcome | Cumulative incidence | ||||||
|---|---|---|---|---|---|---|---|
| Overall | Post‐hospitalization care coordination status | Unadjusted percentage point difference | Adjusted subhazard ratio (aSHR) | ||||
| VA‐delivered |
| Yes | No | Estimate | 95% CI | Estimate | 95% CI |
|
|
| ||||||
| All‐cause readmission | 13.8% | 15.8% | 13.2% | 2.58 | 2.10, 3.06 | 1.04 | 1.01, 1.08 |
| ACSC readmission | 2.1% | 2.3% | 2.0% | 0.29 | 0.09, 0.48 | 0.99 | 0.91, 1.09 |
| Death | 2.2% | 3.6% | 1.8% | 1.89 | 1.65, 2.12 | 1.90 | 1.75, 2.07 |
- —U.S. Department of Veterans Affairs10.13039/100000738
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHealthcare Policy and Management · Geriatric Care and Nursing Homes · Primary Care and Health Outcomes
Summary
- What is known on this topic?
- ○Veterans enrolled in the Veterans Health Administration (VA) frequently experience hospital readmissions, which are costly and can lead to poor care experiences and health outcomes.
- ○Evidence from other patient populations suggests post‐hospitalization care coordination can reduce hospital readmissions; yet, VA has no standard post‐hospitalization care coordination practice for Veterans transitioning home from the hospital.
- ○Existing VA interventions, which tend to emphasize enhanced primary care models and services, have had little to no effect on hospital readmissions and may or may not include care coordination.
- What this study found?
- ○Among Veterans at high risk for hospitalization or mortality (“high‐risk Veterans”), receipt of post‐hospitalization care coordination was associated with no difference in the risk of 30‐day all‐cause hospital readmission.
- ○There was also no difference in the risk of 30‐day ambulatory care sensitive‐condition (ACSC; i.e., potentially avoidable) hospital readmission between high‐risk Veterans who did and did not receive post‐hospitalization care coordination.
- ○Efforts to enhance care coordination data and measurement are needed to more fully understand its effects on hospital readmissions, as are approaches for reducing avoidable readmissions among high‐risk Veterans.
Introduction
1
Hospital readmissions account for a disproportionate share of hospital stays and costs in the US [1]. Strategies to improve timely access to high‐quality post‐hospitalization care have been a focus of US health care reform. In 2013, the Centers for Medicare and Medicaid Services expanded payment for transitional care management services if they occur within seven (for highly complex patients) or 14 (for moderately complex patients) days after discharge [2]. From 2013 to 2018, Medicare spent nearly $1 billion on such post‐hospitalization services [3], a payment change that was associated with increased timely follow‐up after discharge among Medicare fee‐for‐service (FFS) beneficiaries [4]. Receipt of transitional care management services within 30 days of discharge has also been associated with lower total health care costs and mortality at 60 days among Medicare FFS beneficiaries [5].
The Veterans Health Administration (VA) is the largest national integrated health system in the US and serves Veterans with a variety of medical and psychiatric illnesses that place them at risk for hospitalization and readmission [6, 7]. Indeed, approximately 15%–20% of Veterans who are initially hospitalized with high‐risk medical conditions and nearly 25% who are initially hospitalized with chronic psychiatric conditions experience readmission within 30 days [8]. The cost of such readmissions to the VA was $1.2 billion in 2011 [8]. As such, VA has undertaken efforts to integrate care coordination and management into service delivery, with a focus on Veterans with clinical and social factors that place them at risk for hospitalization [9]. Despite this, there is no standard care coordination practice for high‐risk Veterans transitioning home from the hospital [10] and existing VA interventions, which largely emphasize primary care, have had little to no effect on hospital readmissions [11, 12, 13, 14].
Primary care services may or may not include care coordination. Comprehensive care coordination includes patient risk and needs assessment, care planning and education, and communication between patients, care partners, and providers; ideally, care coordination also facilitates integration across the continuum of care and linkages between health system and community resources [15, 16]. Care coordination, broadly, has proven effective for improving clinical outcomes [17, 18, 19] and experiences of care [18, 20, 21, 22], and decreasing or maintaining health care costs [22, 23], including among Veterans at VA facilities [20, 22, 24]. Yet, the value of delivering care coordination services to high‐risk Veterans during or soon after hospital discharge remains largely unknown. Understanding the association between post‐hospitalization care coordination and hospital readmission may help VA to design more effective hospital transition practices for high‐risk Veterans. In this study, we compared the risk of 30‐day all‐cause and ambulatory care‐sensitive condition (ACSC) hospital readmissions in VA‐delivered, VA‐purchased, and Medicare FFS settings among matched cohorts of high‐risk Veterans who did and did not receive VA care coordination services within one day after hospital discharge.
Methods
2
Overview
2.1
This was an observational retrospective cohort study. Veterans who received care coordination within one day after hospital discharge (“treated”) were matched with up to 5 Veterans who did not receive care coordination during this period (“comparators”) across a variety of variables that may be associated with receipt of care coordination and hospital readmission. Among treated Veterans, only the first instance of post‐hospitalization care coordination was considered. Matched treated Veterans and comparators were then followed for 30 days to compare their risks of all‐cause and ACSC readmission. The VA Portland Health Care System Institutional Review Board approved this study.
Role of the Funding Source
2.2
The U.S. Department of Veterans Affairs had no role in the design or conduct of the study; collection, management, analysis, or interpretation of the data; preparation, review, or approval of the manuscript; or the decision to submit the manuscript for publication.
Data and Participants
2.3
Data for this study came from the VA Corporate Data Warehouse, which contains information on hospitalizations in VA‐delivered and VA‐purchased care settings, as well as data on Veterans' demographic, geographic, and clinical characteristics, and their health care use. Data on Medicare FFS hospitalizations, and Medicare FFS and Medicare Advantage enrollment, came from the VA‐linked Centers for Medicare and Medicaid Services (CMS) enrollment files and Medicare FFS claims files [25, 26]. Information on Veterans' dates of death came from the VA Vital Status File, VA Corporate Data Warehouse, and CMS files.
The study population included Veterans who were enrolled in VA care during fiscal year (FY) 2021 (October 2020–September 2021) who were categorized as being at high risk for hospitalization and/or mortality and who were discharged alive from a hospital admission during FY2021 (N = 379,091). Veterans' high‐risk status was ascertained using the Care Assessment of Need (CAN) score. The CAN score is a VA‐derived measure of a Veteran's percentile risk for hospitalization or death within the next year, based on a variety of clinical diagnoses, health care use metrics, medications, laboratory test values, and vital sign measurements [27]. Veterans with a score of 85 or higher during the year prior to their initial hospitalization were considered high risk. Veterans were excluded from the study for: residence outside the continental US, residing more than 180 days in an inpatient setting or skilled nursing facility during the year prior to initial hospitalization, residing 30 days or more in a skilled nursing facility during the 6 months prior to initial hospitalization, discharge from initial hospitalization to a skilled nursing facility, death prior to discharge from initial hospitalization, and missing covariates used in matching (see ‘Matching’). A total of 52,103 Veterans were excluded, resulting in a pre‐match cohort of 326,988 high‐risk Veterans (33,993 who received care coordination and 292,995 who did not).
Matching
2.4
Despite VA care coordination initiatives underway, little is known about how providers determine which high‐risk Veterans should receive care coordination services. However, a recent study identified factors associated with receipt of care coordination services among high‐risk Veterans [28]. With this information, high‐risk Veterans were matched on 40 variables, including eight exact match and 32 propensity score match variables associated with high‐risk Veterans' likelihood of receiving care coordination and which may be associated with Veterans' risk for readmission. Exact match variables included fiscal year‐quarter of initial hospital discharge; sex (male, female); age category (< 45, 45–64, 65–74, 75–84, 85+); Veterans Integrated Service Network (VISN) of residence (VISNs are regional systems of VA care for Veterans in the US, divided into 18 regions); setting of initial hospitalization (VA‐delivered, VA‐purchased, Medicare FFS); Care Coordination and Integrated Case Management (CCICM) early adopter status (yes, no) of the VA facility where the plurality of a Veteran's outpatient care was received during the year prior to initial hospitalization (CCICM is a VA practice framework with the primary focus of improving care coordination, collaboration, communication, and integration at VA facilities; early adopter sites were those that had completed implementation of the CCICM practice framework prior to the study period) [29, 30]; CAN score quartile based on a Veteran's mean CAN score during the year prior to initial hospitalization; and receipt of care coordination services during the year prior to initial hospitalization (yes/no). See Figure 1 footnote for the full set of propensity score matched variables. Propensity scores were estimated based on a model with a 0.1 propensity score caliper. Matching without replacement of treated and comparators was performed on a 1:5 ratio.
Study flow diagram. Exact match variables: Fiscal year‐quarter of initial hospital discharge; sex; age category; Veterans Integrated Service Network (VISN) of residence; setting of initial hospitalization (VA‐delivered, VA‐purchased, Medicare FFS); Care Coordination and Integrated Case Management early adopter status of the VA facility where the plurality of a Veteran's outpatient care was received during the year prior to initial hospitalization; CAN score quartile based on a Veteran's mean CAN score during the year prior to initial hospitalization; and receipt of care coordination services during the year prior to initial hospitalization. Propensity score match variables: Race; Hispanic/Latino/a/−x ethnicity; insurance status; VA priority group; psychoses diagnosis; depression diagnosis; alcohol use disorder diagnosis; substance use disorder diagnosis; Elixhauser readmission risk score; COVID‐19 infection status during the year prior to initial hospitalization; COVID‐19 vaccination status; VA‐delivered hospitalization count in the year prior to initial hospitalization; Medicare FFS hospitalization count in the year prior to initial hospitalization; VA‐purchased hospitalization count in the year prior to initial hospitalization; total hospitalization count in the year prior to initial hospitalization; VA primary care visit count in the year prior to initial hospitalization; VA mental health care visit count in the year prior to initial hospitalization; VA specialty care visit count in the year prior to initial hospitalization; VA reliance in the year prior to initial hospitalization; urban or rural residence; residence in a primary care health professional shortage area; residence in a mental health care health professional shortage area; drive time in minutes to nearest VA facility; drive distance in miles to nearest VA facility; SVI indicators for socioeconomic status, household composition, racial and ethnic minority status, housing type and transportation; county long‐term bed supply; county hospital bed supply; length of stay of initial hospitalization; primary diagnosis of COVID‐19 for initial hospitalization. Abbreviations: CAN, care assessment of need; FFS, Fee‐for‐service; SVI, Social Vulnerability Index; VA, Veterans Health Administration.
Measures
2.5
Our main independent variable was a binary indicator for receipt of VA care coordination within 1 day after hospital discharge, which was defined by the presence of a Current Procedural Terminology (CPT)/Healthcare Common Procedure Coding System (HCPCS) code for transitional care management (99495, 99496), care management (99366–99368), chronic care management (G0506, T1016, T1017, 99491), complex chronic care management (99487, 99489, 99490), or behavioral health care management (G0511, G0512, G2214, 99484, 99492–99494) in the VA Corporate Data Warehouse. Only the first instance of post‐hospitalization care coordination was considered; post‐hospitalization care coordination services that were delivered outside of the VA were not considered. Of note, nearly 80% of the care coordination encounters that we identified were documented with code T1016.
Because we were interested in examining the risk of all‐cause and also more specifically ACSC readmissions, two sets of competing risks outcomes were created for the first post‐hospitalization event in the 30 days following the match date. The first outcome was post‐hospitalization all‐cause readmission with death as a competing risk. The second outcome was post‐hospitalization ACSC readmission, with non‐ACSC readmission and death as competing risks. All‐cause readmissions were defined as any VA‐delivered, VA‐purchased, or Medicare FFS hospital readmission to an acute‐care bed unit [31, 32, 33]. ACSC readmissions were defined as all‐cause readmissions that were potentially preventable based on the Agency for Healthcare Research & Quality Prevention Quality Indicators, which are defined based on the principal diagnosis of a hospital stay and have been validated for identifying hospitalizations for ACSCs [34, 35]. Non‐ACSC readmissions were those not considered ACSC based on the Prevention Quality Indicators.
Variables used to describe our cohort included demographic, geographic, VA facility, and clinical characteristics, and health care use variables collected for a baseline period prior to a Veteran's initial hospitalization, as well as characteristics of Veterans' initial hospitalizations. Sociodemographic variables were ascertained in the year prior to initial hospitalization and included sex, age group, VA priority group (a numeric category from 1 to 8 assigned to a Veteran based on their military service history, VA disability rating, income level, Medicaid eligibility, and receipt of other VA benefits), and race and ethnicity (as social constructs and not biological constructs). Race and ethnicity were self‐reported by Veterans and collected in the electronic health record. Although race and ethnicity were not the primary focus of this study, they were included because health care use and mortality are known to vary by race and ethnicity. VA facility and geographic variables were also ascertained in the year prior to initial hospitalization and included whether a VA facility was an early adopter of the CCICM practice framework (practice framework for standardizing and integrating care coordination) [29, 30], rurality of residence, residence in a primary care health professional shortage area, residence in a mental health professional shortage area, drive time and distance to the nearest VA facility, county‐level skilled nursing facility and inpatient bed supply, and four social vulnerability indicators based on the Center for Disease Control and Prevention's Social Vulnerability Index (i.e., socioeconomic status, household characteristics, racial and ethnic minority status, and housing type and transportation) [36, 37]. Baseline clinical and health care use variables were ascertained in the one to 2 years prior to initial hospitalization and included mean CAN score (2 year), insurance status (one year), receipt of care coordination (1 year), alcohol use disorder diagnosis (2 years), depression diagnosis (2 years), substance (other than alcohol) use disorder diagnosis (2 years), psychoses diagnosis (2 years), Elixhauser readmission risk score (2 years), COVID‐19 infection (1 year), COVID‐19 vaccination status (2 year), VA reliance (1 year; a measure of the proportion of a Veterans' outpatient care that is delivered by VA) [38], and count of prior hospitalizations (1 year; VA‐delivered, VA‐purchased, Medicare FFS), VA primary care visits (1 year), VA specialty care visits (1 year), and VA mental health visits (2 year). Characteristics of initial hospitalizations included FY‐quarter of discharge, setting (VA‐delivered, VA‐purchased, Medicare FFS), length of stay, and whether the primary diagnosis for the hospitalization was COVID‐19.
Statistical Analyses
2.6
Patient characteristics and matching variables were summarized pre‐ and post‐matching using means and standard deviations for continuous variables and frequencies and percentages for categorical variables, and compared across treated and comparator groups using absolute standard mean differences (SMDs) [39, 40, 41]. Cumulative incidence plots were used to assess overall trends in time to first post‐hospitalization event, including all‐cause readmission, ACSC readmission, and death.
For our primary analysis, we used Fine‐Gray competing risk models [42] to estimate adjusted sub‐hazard ratios (aSHRs) and 95% confidence intervals (CIs) for each post‐hospitalization event among the matched cohort. Two separate models were estimated: one for all‐cause readmission and death, and another for ACSC readmission, non‐ACSC readmission, and death. Covariates with SMDs > 0.1 were used as adjustment variables in regression models. These included receipt of care coordination during the year prior to initial hospitalization (SMD 0.13), setting of initial hospitalization (SMD 0.11), count of mental health visits in the year prior to initial hospitalization (SMD −0.15), length of stay of the initial hospitalization (SMD 0.14), and state (SMD 0.32) and Veterans Integrated Service Network of Veteran residence (SMD 0.27). In accordance with a per‐protocol approach [43], assigned untreated Veterans who later received care coordination (i.e., untreated Veterans who experienced cross‐over to treatment during follow‐up) were censored, and outcomes that occurred among these Veterans after censoring were not analyzed.
Four sensitivity analyses were performed to evaluate the robustness of our results. First, we performed inverse probability of censoring weights [44], described in the Supplement, to account for censoring due to cross‐over to treatment among comparators during 30‐day follow‐up. Second, we performed an analysis with an enhanced set of exact match variables about initial hospitalizations. These included whether the initial hospitalization involved an intensive care unit (ICU) stay, quartiles of Diagnostic Related Group (DRG) weights [45], and whether the initial hospital discharge occurred on a weekday or weekend. Third, because we did not have Medicare Advantage encounter data, we performed an analysis that excluded treated Veterans and their matched comparators, as well as individual comparators who had Medicare Advantage coverage. Fourth, and in an attempt to further address endogeneity between receipt of care coordination and readmission, we performed an analysis that was limited to treated and matched comparators who had the same clinical indication for their initial admission, COVID‐19. We chose COVID‐19 because it was the most common reason for initial admission among our analytic cohort.
Additionally, two sets of exploratory subgroup analyses were performed using the same methods as described for our primary analysis. The first subgroup analysis grouped Veterans by the setting of their initial hospitalization: VA‐delivered, VA‐purchased, or Medicare FFS. The second analysis grouped Veterans by the CCICM early adopter status (i.e., early adopter, non‐early adopter) of the VA facility at which they received the plurality of their outpatient care in the year prior to their initial hospitalization. Both the setting of initial hospitalization and CCICM early adopter status were exact‐match variables, resulting in balanced matches across treatment status in all subgroups.
Matching was performed using the PSMATCH procedure from SAS/STAT version 15.1 base SAS version 9.4_M6; all other analyses were performed using R version 4.4.1.
Results
3
Matching
3.1
A total of 326,988 high‐risk Veterans met our study inclusion criteria (Figure 1). Prior to matching, there were medium to large differences in characteristics between treated and comparators (Table S1).
Overall, 93% of treated Veterans were matched with at least one comparator, with 34% matched with five comparators. Matching resulted in an analytic sample of 131,248 Veterans who were discharged alive and matched, of whom 24% (n = 31,614) received care coordination on the day of or the first day after discharge (Figure 1, Table 1, Table S1).
Matched Participant Characteristics
3.2
Following matching, most characteristics were well‐balanced between treated and comparator groups (Table 1). For example, high‐risk Veterans were predominantly male (95.8% vs. 96.8%), non‐Hispanic/Latino/a/‐x ethnicity (95.3% vs. 94.8%), ≥ 65 years of age (69.52% vs. 69.95%), and had Medicare coverage in addition to their VA benefits (71.1% vs. 71.6%). Most resided in urban areas (73.3% vs. 72.0%) and had a ≤ 30‐min drive time from their residence to the nearest VA facility (85.9% vs. 84.9%). Regarding initial admissions, most occurred within VA facilities (91.7% vs. 88.4%). Regarding clinical characteristics, nearly half of high‐risk Veterans had a diagnosis of depression (46.4% vs. 44.3%), about one quarter had diagnoses of psychoses (23.1% vs. 20.4%) and alcohol use disorder (26.4% vs. 24.2%), and one in five had a diagnosis of substance use disorder (19.3% vs. 17.1%). Although differences were small, high‐risk Veterans who received post‐hospitalization care coordination were more likely to have received care coordination in the year prior to their initial hospitalization (50.5% vs. 44.0%, SMD 0.13) and to have had initial hospitalizations in VA facilities (91.7% vs. 88.4%, SMD 0.11); there were also small differences in initial hospitalization length of stay (SMD 0.14). Although high‐risk Veterans were balanced in their psychiatric and substance use diagnoses, those who received post‐hospitalization care coordination had somewhat greater mean count of VA mental health visits in the year prior to initial hospitalization than matched comparators (10.8, SD 23.9 visits vs. 7.5, SD 18.3 visits, SMD 0.15). In addition, state (SMD 0.32) and Veterans Integrated Service Network (SDM 0.27) of residence varied somewhat across treated and comparator groups.
Incidence of Hospital Readmissions by Post‐Hospitalization Care Coordination Status
3.3
The cumulative incidence of 30‐day all‐cause hospital readmission was greater among treated Veterans than among untreated matched comparators (15.9% vs. 13.5%), with a cumulative incidence difference of 2.36 percentage points (95% CI 1.91, 2.82) (Figure 2, Panel A, Table 2). The cumulative incidence of 30‐day ACSC readmission was similar among treated and comparators (2.3% vs. 2.1%), with a cumulative incidence difference of 0.17 percentage points (95% CI –0.36, 0.02) (Figure 2, Panel B, Table 2). After accounting for competing risks and adjusting for variables that remained imbalanced across groups after matching, receipt of post‐hospitalization care coordination was associated with no difference in all‐cause (aSHR 1.03, 95% CI 1.00, 1.07) or ACSC (aSHR 0.97, 95% CI 0.89, 1.05) readmission (Table 2), while the competing risk of death was greater among treated Veterans than among comparators (aSHR 1.85, 95% CI 1.72, 2.00) (Table 2).
Cumulative incidence of 30‐day hospital readmissions and death by post‐hospitalization care coordination status. Abbreviations: ACSC, ambulatory care‐sensitive condition.
Sensitivity Results
3.4
After implementing inverse probability of censoring weights to account for cross‐over among comparators and censoring of their outcomes (Table S2), and in a separate sensitivity analysis applying Medicare Advantage exclusions (Table S3), receipt of post‐hospitalization care coordination was associated with a slightly greater risk of all‐cause readmission and no difference in the risk of ACSC readmission. After including an enhanced set of matching variables (Table S4), and in a separate sensitivity analysis limited to treated and matched comparators who had the same clinical indication for their initial admission, COVID‐19 (Table S5), there were no significant differences in the risk of all‐cause or ACSC readmission. In all sensitivity analyses except for the COVID‐19 analysis, receipt of post‐hospitalization care coordination was associated with an increased (competing) risk of death (Tables S2–S5).
Post Hoc Subgroup Results
3.5
Subgroup results based on the setting of the initial hospitalization were mostly similar to our primary results for all‐cause readmission but varied for ACSC readmission. For example, among Veterans whose initial hospitalizations occurred in VA facilities, receipt of post‐hospitalization care coordination was associated with a somewhat greater risk of all‐cause readmission (aSHR 1.04, 95% CI 1.01, 1.08) and no difference in ACSC readmission (aSHR 0.99, 95% CI 0.91, 1.09) (Table 3). In VA‐purchased and Medicare FFS settings, adjusted subhazard ratios were not statistically significantly different from 1.00 for all‐cause or ACSC readmission (Table 3). However, in CCICM subgroup analyses, Veterans who received the plurality of their outpatient care at VA facilities that were early adopters of the CCICM practice framework had a lower risk of ACSC readmission (0.81, 95% CI 0.67, 0.99) (Table 3). There was no difference in the risk of all‐cause readmission between treated and comparators at CCICM early adopter facilities (aSHR 1.01, 95% CI 0.94, 1.09) (Table 3). Among all subgroups we examined and similar to our primary analyses, receipt of post‐hospitalization care coordination was associated with a greater (competing) risk of death at 30 days (Table 3).
Discussion
4
Our analysis of a well‐matched cohort of high‐risk Veterans demonstrated that receipt of care coordination within 1 day after hospital discharge was associated with no difference in the risk of 30‐day all‐cause hospital readmission in primary and subgroup analyses, and either no difference or a small increased risk for readmission in sensitivity analyses. Regarding ACSC (i.e., potentially preventable) readmission, in primary and sensitivity analyses we also observed no difference in readmission risk between high‐risk Veterans who did and did not receive post‐hospitalization care coordination. However, we observed a significantly lower risk of ACSC readmission among the subgroup of Veterans who received post‐hospitalization care coordination and the plurality of their outpatient care at VA facilities that were early adopters of CCICM—a VA practice framework for standardizing and delivering enhanced care coordination to high‐risk Veterans.
Our null findings parallel certain existing literature. For example, in a meta‐analysis, receipt of brief post‐discharge contacts (e.g., phone calls) within 7 days of hospital discharge was associated with no difference in 30‐day readmissions [10], a finding supported by systematic reviews [10, 46, 47]. In addition, an early VA trial that assigned Veterans to a case manager at hospital discharge had no effect on readmissions [48], and a recent VA initiative to provide longitudinal care coordination to Veterans who use both VA and non‐VA hospitals was associated with no difference in readmissions [49]. On the other hand, a seminal randomized controlled trial conducted within the VA found that enhanced access to primary care shortly after hospital discharge was associated with increased readmissions which were thought to stem in part from providers identifying new/continuing needs for hospital care during post‐discharge visits [11]. This reasoning could explain the positive association we observed in certain analyses between receipt of post‐hospitalization care coordination and all‐cause readmission. However, inconsistencies between our primary and sensitivity analysis and the small magnitude of association should be considered when interpreting these results.
Our finding that treated Veterans had a lower risk of ACSC readmission than comparators if they received the plurality of their outpatient care at VA facilities that were early adopters of CCICM warrants further study. Prior to CCICM adoption, Veterans could have multiple coordinators who arranged different aspects of their care and who may or may not have communicated with each other—a strategy which some suggest led to siloing and fragmentation [50]. First launched in 2016 in partnership between the VA Offices of Nursing and Social Work and Nursing Services, CCICM brings together disparate care management services and providers under one framework with defined standards of practice that support delivery of care coordination, care management, and case management services, and involves assigning one Lead Coordinator to Veterans who need moderate to complex care coordination, with the goal of standardizing care coordination as a service across the VA system [51]. Program data indicate that Veterans enrolled in CCICM have 79% fewer hospitalizations and ED visits, and in 2025, CCICM implementation metrics were integrated into VA performance standards nationally [52]. Care coordination provided at CCICM early adopter VA facilities may have been different (e.g., more comprehensive) than that provided at other VA facilities. However, formal evaluations of CCICM are ongoing; whether CCICM adoption is causally linked with reduced readmissions among high‐risk Veterans requires further study.
Although it is difficult to identify the characteristics of strategies that lead to positive hospital‐to‐home transitions [53], there is some evidence that successful approaches address more components of the care transition, include mechanisms to assess and respond to individuals' peri‐discharge needs, and bridge pre‐ and post‐discharge settings [53, 54, 55, 56]. Supporting this, a recent VA study found that VA facilities that use a greater number of recommended transitional care management processes (e.g., use of a care transitions case manager; printed follow‐up instructions at discharge; post‐hospitalization follow‐up appointments made prior to discharge) have lower hospital readmission rates [57]. Nevertheless, care coordination interventions described in the literature, as well as those delivered across VA, are heterogeneous in their components and intensity [48, 54, 55, 56]. And, despite the array of CPT/HCPCS codes available for documenting care coordination, more than 80% of care coordination encounters among high‐risk Veterans are captured via HCPCS code T1016 [28]—a generic case management code. Further, CPT/HCPCS codes, even when used with specificity, do not detail the specific activities carried out during care coordination encounters. Given that both the intensity and components of care coordination can influence its effectiveness, efforts to enhance care coordination measurement and data are needed to more fully evaluate its impact on patient outcomes such as hospital readmissions, particularly for observational studies that rely on extant administrative data.
Limitations
4.1
This study has limitations. First and foremost, despite developing a well‐balanced cohort of Veterans who did and did not receive post‐hospitalization care coordination services based on an extensive list of factors that have been shown to be associated with receipt of care coordination among high‐risk Veterans [28], residual confounding may remain, and results should not be interpreted as causal. For example, care teams, family, and caregivers may have knowledge about Veterans that is not captured in extant data but may influence both receipt of care coordination and readmissions, such as information about social risks and needs, and the extent of informal care coordination from family and friends. In addition, Veterans may receive referrals for care coordination from family or caregivers and can refer themselves for care coordination. These referrals are not captured in extant VA data and may be related to unobserved factors associated with risks of readmissions and/or death. That we observed an increased (competing) risk of death among Veterans who received post‐hospitalization care coordination suggests such residual confounding may exist. Nonetheless, we believe these findings are useful for understanding the post‐hospitalization care coordination context and an important step in examining effectiveness. Next, we only considered the first instance of post‐hospitalization care coordination in treatment assignment. Although most Veterans (> 80%, data not shown) in our study had only one instance of post‐hospitalization care coordination, it is possible that the relationship between care coordination and hospital readmission may look different if more services are delivered and considered. Third, the sensitivity and specificity of CPT/HCPCS codes for identifying receipt of VA care coordination is unknown; it is possible that some Veterans received care coordination that was not documented by an included CPT/HCPCS code and were thus misclassified as untreated, which could bias our results. Last, this study was conducted among high‐risk Veterans who received care within the VA, who were predominantly male sex, non‐Hispanic/Latino/a/−x ethnicity, and with high levels of mental health comorbidity. Therefore, the generalizability of our findings to populations with different risk profiles may be affected.
Conclusion
5
In a retrospective cohort of matched high‐risk Veterans, we found that receipt of post‐hospitalization care coordination was associated with small or no differences in the risk of 30‐day all‐cause and ACSC readmissions. Care coordination services, including those delivered within the VA and soon after hospital discharge, can be varied and complex, and the effects of care coordination inputs are challenging to unpack using extant data. Efforts to enhance care coordination data and measurement, and future research to explore effective components or sets of components of post‐hospitalization care coordination are needed, as is identification of effective hospital‐to‐home care transition models for high‐risk Veterans.
Conflicts of Interest
The authors declare no conflicts of interest.
Supporting information
Data S1: hesr70044‐sup‐0001‐TableS1.docx.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Agency for Healthcare Research & Quality , “Hospital Admission Versus Readmission Costs,” 2020.
- 2US Department of Health and Human Services , “Medicare Program; Revisions to Payment Policies Under the Physician Fee Schedule, DME Face‐To‐Face Encounters, Elimination of the Requirement for Termination of Non‐Random Prepayment Complex Medical Review and Other Revisions to Part B for CY 2013. Final Rule With Comment Period,” 2012.23155552 · pubmed ↗
- 3L. M. Marcotte , A. Reddy , L. Zhou , S. C. Miller , C. Hudelson , and J. M. Liao , “Trends in Utilization of Transitional Care Management in the United States,” JAMA Network Open 3, no. 1 (2020): e 1919571, 10.1001/jamanetworkopen.2019.19571.31968111 PMC 6991271 · doi ↗ · pubmed ↗
- 4T. S. Anderson , S. J. Herzig , E. R. Marcantonio , R. W. Yeh , J. Souza , and B. E. Landon , “Medicare Transitional Care Management Program and Changes in Timely Postdischarge Follow‐Up,” JAMA Health Forum 5, no. 4 (2024): e 240417, 10.1001/jamahealthforum.2024.0417.38607641 PMC 11065163 · doi ↗ · pubmed ↗
- 5A. B. Bindman and D. F. Cox , “Changes in Health Care Costs and Mortality Associated With Transitional Care Management Services After a Discharge Among Medicare Beneficiaries,” JAMA Internal Medicine 178, no. 9 (2018): 1165–1171, 10.1001/jamainternmed.2018.2572.30073240 PMC 6583218 · doi ↗ · pubmed ↗
- 6P. Boersma , R. Cohen , C. Zelaya , and E. Moy , “Multiple Chronic Conditions Among Veterans and Nonveterans: United States,” Centers for Disease Control and Prevention 13 (2021): 1–12.33663648 · pubmed ↗
- 7M. Olenick , M. Flowers , and V. J. Diaz , “US Veterans and Their Unique Issues: Enhancing Health Care Professional Awareness,” Advances in Medical Education and Practice 6 (2015): 635–639, 10.2147/AMEP.S 89479.26664252 PMC 4671760 · doi ↗ · pubmed ↗
- 8K. Carey and T. Stefos , “The Cost of Hospital Readmissions: Evidence From the VA,” Health Care Management Science 19, no. 3 (2016): 241–248, 10.1007/s 10729-014-9316-9.25576391 · doi ↗ · pubmed ↗