Venous Thromboembolism in Aggressive B‐Cell Lymphoma Patients Treated with CD19 CAR‐T Therapy: Single‐Institution Study
Neha Venkatesh, Kevin Milligan, Julia Parrish, Yun Qing, Ryan Sun, Paolo Strati, Jeremy Ramdial, Amy Ayers, Sairah Ahmed, Cristhiam Rojas Hernandez

TL;DR
This study finds that patients with aggressive B-cell lymphoma treated with CAR-T therapy face a notable risk of venous blood clots, especially in the first month.
Contribution
The study reports the incidence and risk factors for VTE in LBCL patients undergoing CAR-T therapy, emphasizing PMBCL and ICANS as key factors.
Findings
The 6-month VTE incidence was 7.6%, mostly linked to central venous catheters in the upper extremities.
PMBCL patients had a 30% VTE incidence, significantly higher than DLBCL and TFL patients.
High-grade ICANS was strongly associated with VTE occurrence (p = 0.013).
Abstract
Large B‐cell lymphomas (LBCLs) are a common subtype of non‐Hodgkin lymphomas. CD19 chimeric antigen receptor T‐cell (CAR‐T) therapy has revolutionized LBCL treatment, with high remission rates but also significant toxicities, including cytokine release syndrome (CRS) and immune effector cell‐associated neurotoxicity syndrome (ICANS). Venous thromboembolism (VTE) in CAR‐T therapy patients is understudied. This study aims to determine the incidence and characteristics of acute VTE in LBCL patients treated with CAR‐T therapy and identify baseline clinical features associated with VTE. Methods: We retrospectively reviewed 172 adult LBCL patients treated with CAR‐T therapy from January 2018 to November 2019 at MD Anderson Cancer Center. Data on demographics, clinical characteristics, and adverse events were collected. VTE events within 6 months post‐CAR‐T therapy were confirmed by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
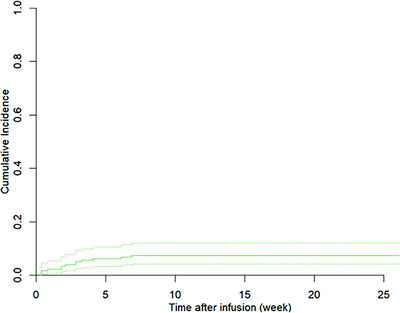 FIGURE 1
FIGURE 1| Characteristic and categories |
|
|---|---|
| Age (years) | |
| Median, (IQR) | 59, (49–67) |
| Sex | |
| Female | 51 (29.65) |
| Male | 121 (70.35) |
| Diagnosis | |
| DLBCL | 133 (77.33) |
| PMBCL | 10 (5.81) |
| TFL | 29 (16.86) |
| Stage | |
| I | 4 (2.33) |
| I/II | 16 (9.30) |
| II | 11 (6.40) |
| III | 10 (5.81) |
| III/IV | 63 (36.63) |
| IV | 68 (39.53) |
| ECOG | |
| 0 | 49 (28.49) |
| 1 | 103 (59.88) |
| 2 | 12 (6.98) |
| 3 | 7 (4.07) |
| 4 | 1 (0.58) |
| IPI score | |
| 0 | 6 (3.49) |
| 1 | 21 (12.21) |
| 2 | 49 (28.49) |
| 3 | 50 (29.07) |
| 4 | 44 (25.58) |
| 5 | 2 (1.16) |
| Previous therapies > 2 | |
| No | 36 (20.93) |
| Yes | 136 (79.07) |
| Received bridging therapy | |
| No | 85 (49.42) |
| Yes | 87 (50.58) |
| Received bridging chemotherapy | |
| No | 119 (69.19) |
| Yes | 53 (30.81) |
| Received autologous HSCT | |
| No | 127 (73.84) |
| Yes | 45 (26.16) |
| Received allogeneic HSCT | |
| No | 169 (98.26) |
| Yes | 3 (1.74) |
| Baseline ferritin without and with DVT | |
| No | 1704 (1364) |
| Yes | 890 (1373) |
| Prior history of VTE | |
| No | 121 (70.35) |
| Yes | 51 (29.65) |
| Prior anticoagulation use | |
| No | 116 (67.44) |
| Yes | 56 (32.56) |
| Prior antiplatelet use | |
| No | 126 (73.26) |
| Yes | 46 (26.74) |
| ICANS Grade 3 or 4 | |
| No | 111 (64.53) |
| Yes | 61 (35.47) |
| CRS Grade 3 or higher | |
| No | 159 (92.44) |
| Yes | 13 (7.56) |
| Characteristic and categories | No VTE ( | Developed VTE ( | Total ( |
|
|---|---|---|---|---|
| Age | 0.572 | |||
| Under 60 | 88 (93.62) | 6 (6.38) | 94 (100.00) | |
| Over 60 | 71 (91.03) | 7 (8.97) | 78 (100.00) | |
| Sex | 1 | |||
| Female | 47 (92.16) | 4 (7.84) | 51 (100.00) | |
| Male | 112 (92.56) | 9 (7.44) | 121 (100.00) | |
| Diagnosis | 0.033 | |||
| DLBCL | 124 (93.23) | 9 (6.77) | 133 (100.00) | |
| PMBCL | 7 (70.00) | 3 (30.00) | 10 (100.00) | |
| TFL | 28 (96.55) | 1 (3.45) | 29 (100.00) | |
| Stage | 0.737 | |||
| I | 4 (100.00) | 0 (0.00) | 4 (100.00) | |
| I/II | 14 (87.50) | 2 (12.50) | 16 (100.00) | |
| II | 11 (100.00) | 0 (0.00) | 11 (100.00) | |
| III | 9 (90.00) | 1 (10.00) | 10 (100.00) | |
| III/IV | 57 (90.48) | 6 (9.52) | 63 (100.00) | |
| IV | 64 (94.12) | 4 (5.88) | 68 (100.00) | |
| ECOG | 0.395 | |||
| 0 | 47 (95.92) | 2 (4.08) | 49 (100.00) | |
| 1 | 94 (91.26) | 9 (8.74) | 103 (100.00) | |
| 2 | 10 (83.33) | 2 (16.67) | 12 (100.00) | |
| 3 | 7 (100.00) | 0 (0.00) | 7 (100.00) | |
| 4 | 1 (100.00) | 0 (0.00) | 1 (100.00) | |
| IPI score | 0.901 | |||
| 0 | 6 (100.00) | 0 (0.00) | 6 (100.00) | |
| 1 | 20 (95.24) | 1 (4.76) | 21 (100.00) | |
| 2 | 46 (93.88) | 3 (6.12) | 49 (100.00) | |
| 3 | 46 (92.00) | 4 (8.00) | 50 (100.00) | |
| 4 | 39 (88.64) | 5 (11.36) | 44 (100.00) | |
| 5 | 2 (100.00) | 0 (0.00) | 2 (100.00) | |
| Previous therapies > 2 | 1 | |||
| No | 34 (94.44) | 2 (5.56) | 36 (100.00) | |
| Yes | 125 (91.91) | 11 (8.09) | 136 (100.00) | |
| Received bridging therapy | 0.248 | |||
| No | 81 (95.29) | 4 (4.71) | 85 (100.00) | |
| Yes | 78 (89.66) | 9 (10.34) | 87 (100.00) | |
| Received bridging chemotherapy | 1 | |||
| No | 110 (92.44) | 9 (7.56) | 119 (100.00) | |
| Yes | 49 (92.45) | 4 (7.55) | 53 (100.00) | |
| Received autologous HSCT | 1 | |||
| No | 117 (92.13) | 10 (7.87) | 127 (100.00) | |
| Yes | 42 (93.33) | 3 (6.67) | 45 (100.00) | |
| Received Allogeneic HSCT | 0.211 | |||
| No | 157 (92.90) | 12 (7.10) | 169 (100.00) | |
| Yes | 2 (66.67) | 1 (33.33) | 3 (100.00) | |
| Prior history of VTE | 0.531 | |||
| No | 113 (93.39) | 8 (6.61) | 121 (100.00) | |
| Yes | 46 (90.20) | 5 (9.80) | 51 (100.00) | |
| Prior anticoagulation use | 1 | |||
| No | 107 (92.24) | 9 (7.76) | 116 (100.00) | |
| Yes | 52 (92.86) | 4 (7.14) | 56 (100.00) | |
| Prior antiplatelet use | 1 | |||
| No | 116 (92.06) | 10 (7.94) | 126 (100.00) | |
| Yes | 43 (93.48) | 3 (6.52) | 46 (100.00) | |
| ICANS Grade 3 or 4 | 0.013 | |||
| No | 107 (96.40) | 4 (3.60) | 111 (100.00) | |
| Yes | 52 (85.25) | 9 (14.75) | 61 (100.00) | |
| CRS Grade 3 or 4 | 0.256 | |||
| No | 148 (93.08) | 11 (6.92) | 159 (100.00) | |
| Yes | 11 (84.62) | 2 (15.38) | 13 (100.00) |
| Variable | Categories | Number of patients | Number of VTE | OR (95% confidence limits) |
|
|---|---|---|---|---|---|
| Diagnosis | All patients | 172 | 13 | ||
| DLBCL | 133 | 9 | Reference group | ||
| PMBCL | 10 | 3 | 6.546 (1.169, 32.36) | 0.022 | |
| TFL | 29 | 1 | 0.612 (0.032, 3.640) | 0.7 | |
| ICANS Grade 3 or 4 | No | 111 | 4 | Reference group | |
| Yes | 61 | 9 | 4.672 (1.398, 18.65) | 0.017 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCAR-T cell therapy research · Lymphoma Diagnosis and Treatment · Cutaneous lymphoproliferative disorders research
Introduction
1
Large B‐cell lymphomas (LBCLs) are a common subtype of NHLs, comprising up to 40% of cases globally, with an estimated incidence of 7 per 100,000 in the United States [1, 2].
CD19 chimeric antigen receptor T‐cell (CAR‐T) therapy has revolutionized LBCL treatment, with studies reporting complete remission rates as high as 63.6% in a refractory disease setting [3]. CAR‐T cells target specific tumor antigens, effectively killing tumor cells expressing the CD19 antigen, which is present in 95% of LBCL cases [3]. Despite its success, CAR‐T therapy comes with a unique toxicity profile, including most commonly cytokine release syndrome (CRS) and with neurologic toxicity termed immune effector cell‐associated neurotoxicity syndrome (ICANS). CRS can lead to multi‐organ toxicities, including hematological complications [4]. Among hematological complications, venous thromboembolism (VTE) has not yet been characterized in recipients of CAR‐T.
Although VTE is a significant cause of morbidity and mortality in hematological malignancies, data on thrombotic complications in patients receiving CAR‐T therapy are limited. Preliminary evidence suggests that CAR‐T therapy can cause immune‐mediated endothelial activation and suppressed fibrinolysis, potentially leading to thrombosis [5]. Patients receiving CAR‐T therapy often have advanced‐stage disease and undergo invasive procedures, further increasing their thrombosis risk [6]. In addition, high levels of interleukin‐6 (IL‐6) and specific genetic polymorphisms such as the IL‐6 promoter polymorphism (−57 C/G) seen in patients receiving CAR‐T therapy may contribute to this risk [7].
Existing studies indicate that VTE in CAR‐T therapy patients can manifest as pulmonary embolism, or upper or lower extremity deep vein thrombosis [8]. Risk factors include a history of recent VTE, a body mass index (BMI) ≥ 30, recent procedures like central venous catheter (CVC) insertion (especially in upper extremities), intensive care unit (ICU) stays, and recent infections [8, 9]. Managing anticoagulation is challenging due to post‐therapy thrombocytopenia [5, 8].
Given the limited data on VTE in CAR‐T therapy patients, our study aims to determine the incidence and characteristics of acute VTE in LBCL patients treated with CAR‐T therapy, and to identify baseline clinical features associated with VTE.
Methods
2
Study Design and Population
2.1
The study included consecutive adult patients who had ever received autologous anti‐CD19 axicabtagene ciloleucel CAR‐T therapy for aggressive B‐cell lymphoma at our institution from January 1, 2018, to November 9, 2019.
Patients were identified through an institutional database and the study was approved by The University of Texas MD Anderson Cancer Center Institutional Review Board and was conducted in accordance with the institutional guidelines and principles of the Declaration of Helsinki. The clinical characteristics and laboratory features were collected before the initiation of lymphodepleting chemotherapy.
Demographic and clinical characteristics were collected at the time of CAR‐T cell therapy. CRS and ICANS were prospectively graded and managed according to the ASTCT guidelines [10]. Response status was determined by the Lugano 2014 classification. Incidence and date of relevant adverse events, such as infections and cytopenia, were collected. VTE‐related data, such as history of VTE, presence of CVCs, and other comorbidities using the Carlson index, were collected within the following 6 months from CAR‐T.
Outcome Definition
2.2
Individual medical records of identified patients were manually screened for acute VTE complications within 6 months of CAR‐T cell therapy infusion. All events were confirmed by diagnostic imaging modalities.
Statistical Analysis
2.3
Summary statistics were provided for patient demographics as well as clinical and biological variables. Continuous variables were presented as mean ± SD or median (interquartile range [IQR]), as appropriate based on normality, and categorical variables were presented as percentages. Continuous data were compared using the unpaired Student's t‐tests or Wilcoxon rank‐sum tests, as appropriate. Categorical data was compared using the Fisher's exact test. Univariate analyses were performed. Statistical significance was defined using a 2‐tailed p value ≤ 0.05. To quantify the risk of VTE, we used the cumulative incidence function. To compare cumulative incidence functions of VTE and death, we use Gray's test.
Results
3
Baseline Characteristics
3.1
A total of 172 patients were included in the study. Patients were predominantly male (70%) with a median age of 59 years. Tumor histology categories were diffuse large B cell lymphoma (DLBCL), primary mediastinal large B cell lymphoma (PMBCL), or transformed follicular lymphoma (TFL), and 76.16% had Stage III or IV disease. Patients had received more than 2 lines of cancer therapy (79.07%) before receiving CAR‐T cell treatment. Most patients had a performance status of ECOG of 0 or 1 (88.37%).
A minority of patients had prior history of VTE (29.65%), prior anticoagulation use (32.56%), or prior antiplatelet use (26.74%). All patients were on pharmacological VTE prophylaxis unless there was a bleeding contraindication or platelet counts were < 50 K/µL, at which time for patients without prior VTE, prophylaxis would be held. For patients who were on anticoagulation for a previous thrombosis, dosing would be therapeutic and held when platelet counts were < 50/µL. We did not reliably capture the frequency and compliance use of mechanical VTE prophylaxis (i.e., pneumatic compression devices) when pharmacological VTE prophylaxis was contraindicated. Patients were not routinely prescribed outpatient VTE prophylaxis after hospital discharge from CART infusion.
After CAR‐T cell treatment, a small subset of patients had severe toxicities such as ICANS Grade 3 or 4 (35.47%) or CRS Grade 3 or higher (7.56%) from CAR‐T cell therapy (Table 1).
Venous Thromboembolic Complications
3.2
The incidence of deep VTE at 6 months from CAR‐T cell therapy was 7.6%, and the cumulative incidence estimate, counting death as a competing risk estimate was similar (Figure 1). Out of those events, 10/13 events were in the upper extremity (UE) and related to CVCs. Of these, 12/13 events were proximal DVTs in the axillary or femoral veins. In addition, 11/13 patients with DVT had peripherally inserted central catheters (PICC). Seven of the UE events were symptomatic, while two events were found incidentally in other imaging modalities. The rest of VTE events were occurred in lower extremities and were all symptomatic. No events of pulmonary embolism were observed. No fatality was observed due to VTE.
Time to VTE counting death as competing risk.
Univariate analysis for demographics, clinical characteristics, and VTE development showed a significant relationship between histology of disease (p value 0.033), and high‐grade ICANS (grade ≥ 3) (p value 0.013). Patients with PMBCL developed VTE (30%, n = 3) almost five times as much as patients with DLBCL (6.77%, n = 9) and almost 10 times more than patients with TFL (3.45%, n = 1) (Table 2).
Overall survival analysis in this cohort showed a significantly reduced OS association in PMBCL patients with VTE, and if ICANS Grade 3 or 4 toxicity was observed in those with VTE (Table 3). The covariates that were controlled for are diagnosis (all, DLBCL, PMBCL, or TFL) and whether ICANS Grade 3 or 4 was present or not. Time to event analysis of VTE with death as competing risk showed that out of 172 patients, 64 patients died, and of those, 43 died without VTE while 15 died with unknown VTE status. Out of all patients who died, six patients presented with VTE within 6 months of CAR‐T therapy. For patients with PMBCL, the 6 month incidence of acute VTE was 30%, and for those who developed ICANS Grade 3 or 4, it was 15%. For all patients, 4‐week cumulative incidence of VTE was 5.81% and, 8‐week cumulative incidence of VTE was 7.56%, showing us that most thrombotic events took place in the first month of CAR‐T therapy initiation.
Discussion
4
The incidence of VTE at 6 months after axicabtagene ciloleucel infusions of CAR‐T cell therapy was 7.6% in our cohort, in which all patients had central venous access. Comparatively, the incidence of thrombosis after conventional chemotherapy traditionally varies across studies due to different patient populations, types of lymphoma, chemotherapy regimens, and study designs. The overall global incidence rate of thrombosis in lymphoma patients, including both venous and arterial events, is reported at 6.4% [11]. These events are more frequent in the initial cycles of chemotherapy, particularly by the third cycle [12]. Key risk factors include the use of specific chemotherapeutic agents like doxorubicin or methotrexate, elevated hemoglobin or creatinine levels, and patient characteristics such as female sex [12].
In NHL, the incidence of thrombosis is approximately 6.5%, with high‐grade NHL showing a higher incidence (8.3%) compared to low‐grade NHL (6.3%) [11]. This is similar to the rate of VTE in our patients with LBCLs. For patients with Hodgkin lymphoma (HL), the incidence is lower, around 3.3%, with a higher incidence noted in advanced stages and those treated with dose‐dense regimens such as BEACOPP‐14 [13]. For patients undergoing allogeneic HSCT, the incidence of catheter‐related DVT and PE/ lower extremity DVT at 12 months was 4.2% and 4.8%, respectively. Hospitalization inpatient status was a strong predictor for the onset of these thrombotic events [14]. Therefore, the incidence of VTE observed in our CAR‐T treated population is similar to that seen in the general lymphoma population.
A retrospective, single‐center study of 148 patients with LBCL undergoing CAR‐T therapy reported an 11% incidence of new VTE events. Patients with Grade 3 or higher CRS, severe neurotoxicity, poor baseline performance status, and large tumor burden were identified as having a higher risk of developing VTE following CAR‐T therapy [15]. We observed similar findings in our study as well. Another meta‐analysis by Chitkara et al. [16], published in Current Oncology, reviewed Phase 2 and Phase 3 clinical trials and found a very low incidence of VTE, with only 3 out of 1017 patients experiencing VTE. Their study did not find a statistically significant association between increased VTE incidence and CRS or ICANS. There may be a variety of factors to account for the lack of consistency in our findings. Heterogeneity in the type of CAR‐T product (as this study used five different types of CAR‐T products as opposed to our study, which used one CAR‐T product), differences in thromboprophylaxis strategies, and the type of central venous access can be explored in future studies. A multi‐institutional study accounted for similar risk factors for VTE that we found in our study while creating a risk assessment model to predict VTE risk in lymphoma patients, including lymphoma histology and grade, in addition to therapy type, recent hospitalization, BMI, etc. [17].
Univariate analysis showed a significant relationship between tumor histology and VTE, as well as high‐grade (3 or 4 toxicity) ICANS and VTE. Our patients with PMBCL developed VTE almost five times more frequently than those with DLBCL and almost 10 times more frequently than those with TFL. Interestingly, all VTE events in the PMBCL cases were CVC‐related. Due to the small number of patients with PMBCL in our cohort, it is difficult to draw hypotheses on the reason for the association. Others have described that the anatomical and physiological phenotype of PMBCL, especially the presence of bulky mediastinal masses that can compress major vessels, such as the superior vena cava, could predispose patients to venous thrombosis as well as elevated levels of fibrinogen and D‐dimer [18]. In a study focusing on PMBCL, it was found that a significant proportion of patients (35.7%) developed VTE, including DVT and PE, compared to only 6.4% general incidence of thrombosis across all lymphoma types, which is consistent with our findings [18].
The association between high‐grade (3 or 4 toxicity) ICANS and VTE we observed is highly understudied with one current study documented by Schorr et al. [19]. Their proposed mechanism included elevated d‐dimer level, endothelial activation, and vascular injury, causing elevated serum markers such as von Willebrand factor and angiopoietin‐2, leading to a prothrombotic state [19, 20].
While our study demonstrates increased risk of VTE associated with tumor histology and high‐grade ICANS toxicity, our study does not allow us to determine if the complication of thrombosis is intrinsically related to CAR‐T cell therapy or to the type of patients who received it, or both. However, we can more closely examine and compare the incidence and risk factors of thrombosis in our cohort who received CAR‐T cell therapy to other study cohorts who received traditional chemotherapy regimens and/or CAR‐T therapy in future studies to be able to better prevent and address this somewhat common adverse event.
The timing of thrombosis development after starting CAR‐T therapy is also something we analyzed. Most thrombotic events took place within 4 weeks of CAR‐T therapy initiation in our cohort. This aligns with a median time of 23.5 days post‐infusion for thrombotic events from another single‐center retrospective study in adults with B‐cell malignancies and a median time of 29 days for thrombosis after CAR‐T therapy in patients with LBCL, or B‐cell ALL [19, 21]. A large meta‐analysis including 47 studies with a total of 7040 patients found that the incidence of VTE was highest within the first 6 months following CAR‐T therapy as well, with a pooled incidence of 2.4% per patient month (95% CI, 1.4%–3.4%). For follow‐up periods longer than 6 months, the incidence dropped significantly to 0.1% per patient‐month (95% CI, 0%–0.1%) [22]. These findings indicate that the risk of thrombosis is especially heightened in the initial month after CAR‐T cell therapy, highlighting the need for careful monitoring during this critical period and a potential study of the role of thromboprophylaxis strategies.
This study has several limitations. The relatively small sample size from a single institution reduces the generalizability of our findings. In addition, the lack of a control group receiving alternative therapies impedes direct comparison of VTE incidence between different treatment modalities. Moreover, the study period only captures short‐term VTE incidence within 6 months, potentially overlooking late thrombotic events. Further prospective, multicenter studies are warranted to validate these findings and explore the underlying mechanisms of VTE in CAR‐T therapy patients.
Conclusions
5
Our study demonstrates that there is a comparable risk for VTE in patients receiving CAR‐T cell therapy for a diagnosis of LBCL as in patients who have a diagnosis of lymphoma receiving chemotherapy. Interestingly, the incidence of VTE is higher in the first 4 weeks post CAR‐T, potentially due to the proximity of CAR‐T related toxicity. As these patients are constantly monitored during the first 4 weeks, and then only every 2–3 months after CAR‐T therapy, we may see these events of VTE early when patients are being monitored more closely. Further studies are needed to better understand the pathophysiology of VTE in patients who receive CART cell therapy, and the potential role of venous thromboprophylaxis within the first few weeks of CAR‐T.
Author Contributions
Neha Venkatesh: conceptualization, writing – original draft, investigation. Kevin Milligan: data curation. Julia Parrish: data curation. Yun Qing: data analysis. Ryan Sun: data analysis. Paolo Strati: writing – review and editing. Jeremy Ramdial: writing – review and editing. Amy Ayers: writing – review and editing. Sairah Ahmed: writing – review and editing, supervision. Cristhiam Rojas Hernandez: conceptualization, writing – review and editing, supervision, data curation.
Funding
Support grants for statistical analysis: R35GM154843 and U54CA302435.
Conflicts of Interest
Paolo Strati is a consultant for Roche‐Genentech, AbbVie‐Genmab, Ipsen, Kite/Gilead, Hutchison MediPharma, AstraZeneca‐Acerta, ADC Therapeutics, Sobi, and TG Therapeutics; he has received research funds from Sobi, AstraZeneca‐Acerta, ALX Oncology, and ADC Therapeutics. Sairah Ahmed has research support to institution for clinical trials from Nektar, Merck, Xencor, Chimagen, Janssen, KITE and Genmab, has membership on Chimagen scientific advisory committee; she serves on Data Safety Monitoring Board for Myeloid Therapeutics; she is a consultant for ADC Therapeutics, KITE/Gilead. Cristhiam Rojas Hernandez has received research support from ANTHOS Therapeutics. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1M. Horvat , V. Zadnik , T. Južnič Šetina , et al., “Diffuse Large B‐Cell Lymphoma: 10 Years' Real‐World Clinical Experience with Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine and Prednisolone,” Oncology Letters 15, no. 3 (2018): 3602–3609, 10.3892/ol.2018.7774.29467881 PMC 5796369 · doi ↗ · pubmed ↗
- 2Y. Li , Y. Wang , Z. Wang , D. Yi , and S. Ma , “Racial Differences in Three Major NHL Subtypes: Descriptive Epidemiology,” Cancer Epidemiology 39, no. 1 (2015): 8–13, 10.1016/j.canep.2014.12.001.25560974 PMC 4323749 · doi ↗ · pubmed ↗
- 3C. Huang , L. Wu , R. Liu , et al., “Efficacy and Safety of CD 19 Chimeric Antigen Receptor T Cells in the Treatment of 11 Patients with Relapsed/Refractory B‐Cell Lymphoma: a Single‐Center Study,” Annals of Translational Medicine 8, no. 17 (2020): 1048, 10.21037/atm-20-4363.33145267 PMC 7575989 · doi ↗ · pubmed ↗
- 4C. Zhang , S. Durer , K. C. Thandra , and A. Kasi , Chimeric Antigen Receptor T‐Cell Therapy (Stat Pearls, 2024).30725979 · pubmed ↗
- 5C. T. Esmon , “Inflammation and Thrombosis,” Journal of Thrombosis and Haemostasis 1, no. 7 (2003): 1343–1348, 10.1046/j.1538-7836.2003.00261.x.12871267 · doi ↗ · pubmed ↗
- 6N. M. Hossain and M. I. Nishimura , “Late Events after CD‐19 CAR‐T Treatment,” Biology of Blood and Marrow Transplantation 26, no. 1 (2020): e 1–e 2, 10.1016/j.bbmt.2019.10.020.31669398 · doi ↗ · pubmed ↗
- 7H. Liu , Y. Yang , J. Jiang , et al., “Coexistence of a Huge Venous Thromboembolism and Bleeding Tendency in Cytokine Release Syndrome during CAR‐T Therapy,” Onco Targets and Therapy 12 (2019): 8955–8960, 10.2147/OTT.S 223697.31802905 PMC 6826178 · doi ↗ · pubmed ↗
- 8A. L. Parks , S. Kambhampati Thiruvengadam , B. Fakhri , et al., “Incidence, Management and Outcomes of Arterial and Venous Thrombosis after Chimeric Antigen Receptor Modified T Cells for B Cell Lymphoma and Multiple Myeloma,” Leukemia & Lymphoma 62, no. 4 (2021): 1003–1006, 10.1080/10428194.2020.1852474.33258699 PMC 8012226 · doi ↗ · pubmed ↗