Delftia spp as Opportunistic Pathogens: a narrative review
Michael P. Ryan, J. Tony Pembroke

TL;DR
This paper reviews Delftia species as opportunistic pathogens, highlighting their increasing clinical relevance and treatment considerations.
Contribution
The study compiles 175 reported cases of Delftia infections, emphasizing D. acidovorans and treatment antibiotic efficacy.
Findings
Delftia acidovorans accounts for 87.4% of reported Delftia infections.
Ceftazidime, ciprofloxacin, and imipenem are effective antibiotics for treating Delftia infections.
Gentamicin should be avoided in treating these infections.
Abstract
Non-fermenting Gram-negative bacteria pose a considerable challenge in medical settings and are increasingly implicated in infections in these settings. Many are opportunistic pathogens that primarily affect patients with other acute or chronic health conditions. Among them, Delftia species—particularly Delftia acidovorans - have traditionally been regarded as of limited clinical relevance. However, a comprehensive literature review has identified 175 reported cases of Delftia infections, with D. acidovorans accounting the majority cases (87.4 %). Bacteraemia was the most commonly associated condition, reported in 23 cases (13.1 %) with other infections such as pneumonia (9.8 %), sepsis (3.4 %) and peritonitis (2.9 %) also being prominent. The findings suggested that the antibiotics ceftazidime, ciprofloxacin and imipenem are usually effective in treating Delftia infections, but that…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
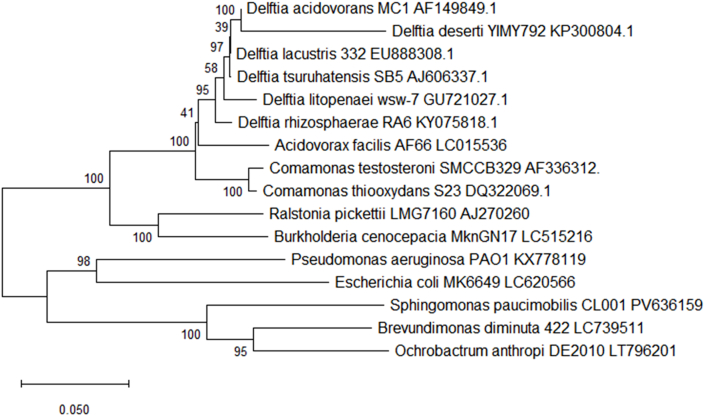 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfections and bacterial resistance · Cerebrospinal fluid and hydrocephalus · Otolaryngology and Infectious Diseases
Introduction
1
The emergence of Gram-negative, non-fermenting bacteria as a common cause of infections in immunocompromised patients has become a major issue in clinical settings. These organisms are ubiquitous in natural environment being found in many different niches [1]. These niches include soil, plants and animals [2] and various water sources (including hospital water, aircraft water, bottled drinking water, purified water) [[3], [4], [5], [6]].
These bacteria are frequently resistant to many different antimicrobials. Examples include resistance to penicillin's, aminoglycosides and monobactam's in R. pickettii [7] and β -lactams in Ochrobactrum spp [8].
While the major pathogenic bacteria of this heterogeneous group (Pseudomonas aeruginosa [9], the Burkholderia cepacian complex [10], Acinetobacter baumannii [11]) are well known other lesser-known bacteria are also emerging as pathogenic organisms. These include bacterial species such as*, Ralstonia pickettii* [12], Sphingomonas paucimobilis [13], Ochrobactrum spp [14], Comanonas spp [15] and Brevundimonas spp [16].
Delftia spp. are one of these emerging genera. They have been isolated from many different environmental niches, including water sources [17], aircraft water [4], wastewater [18], soil, plants [19], and animals [20]. Delftia spp. have been shown to degrade xenobiotic pollutants [21,22] and to detoxify heavy metals [23,24] this includes the biomineralize of gold. Delftia spp. are believed to be of low virulence and routine surveillance systems rarely track Delftia explicitly. Despite this Delftia spp have caused infections, including serious infection such as endocarditis [25], sepsis [26] and pneumonia [27] in immunocompetent hosts.
Examination of literature sources (both scientific and medical) established that Delftia spp give rise to a multitude of different infections potentially indicating a stronger pathogenic potential than was supposed. The overall aim of this study was to support the thesis that Delftia spp are important pathogens needing more attention.
Genus Delftia
1.1
The Delftia genus was first described in 1999 with the reassignment of Comamonas acidovorans to Delftia [28]. Five further species were added to the genus over the next 20 years: Delftia tsuruhatensis in 2003 [29], Delftia lacustris in 2009 [30], Delftia litopenaei in 2012 [31], Delftia deserti in 2015 [32] and Delftia rhizosphaerae in 2017 [33] (see Fig. 1). Delftia is a betaproteobacterial genus widely spread in the environment, these niches include soil, water sources, plants, and both healthy and diseased animal. The genus has a wide array of potential applications both in agriculture and in industry. These applications include immobilization of heavy metals including lead [34]and zinc [35], enhancement of plant growth [36] and microbial treatment of hydrocarbon-polluted soils [37]. Delftia acidovorans is the type species of the genus with the type strain being ATCC 15668.Fig. 1. Phylogenetic tree of the genus Delftia built with 16S rDNA genes (partial sequences of ∼1400 bp) (gene accession numbers are given along with the species name) with the other Pseudomonadota species. The tree was built with neighbour-joining (Tajma-Nei method) using the MEGA 11 software package. Bootstrap values are represented by numbers at nodes. These are based on 500 resamplings. Bar, 0.0050 substitutions per site [59]. It should be noted that the above tree is based upon 16S rDNA and, as such, is suggestive only.Fig. 1
Genomics of Delftia
1.2
Bhat et al. carried out a pangenomic analysis of 61 Delftia species genomes. The genomes studied represented three of the described Delftia species, D. acidovorans, D. tsuruhatensis and D. lacustris with an additional 27 unassigned Delftia species (D. litopenaei, D. rhizosphaerae and D. deserti have no genome data) [38].
Median genome size for these 61 strains was 6.6 Mbp, with the largest size being 7.3Mbp [38]. These results agree with the multiple genome analysis of D. tsuruhatensis [39]. Phylogenomic comparison of these 61 Delftia genomes indicated that the genus can be split into two clades, the first named the Delftia acidovorans clade contains isolates from soil and plant rhizospheres, while the second named the Delftia lacustris/Delftia tsuruhatensis clade contains isolates from humans and sludge [38]. The ecological versatility of the genus was supported by the high pan-genome size observed, ranging from 17 986 genes for D acidovorans clade and 18 987 genes for clade D. lacustris/D. tsuruhatensis clade [38]. Although both clade members showed ecological specialism the proteomes were quite similar with only 27 protein differences present in the D acidovorans clade and 12 proteins present in the D. lacustris/D. tsuruhatensis clade not in the first clade [38]. Yin et al. (2022) also carried out gene synteny analysis amongst 2 key species of D. tsuruhatensis, strains CM13 and TR1180. This showed a high level of synteny with many rearrangements and inversions amongst the comparison and some 37 synteny blocks recognised, ranging from 6,735,844 bp (93.6 %) in CM13 and 6,606,877 bp (98.4 %) in TR1180 suggestive of rearrangements and inversions occurred during the genomic evolution of D. tsuruhatensis [39].
Mobile genetic elements
1.3
Genome analysis within the comparison revealed many types of mobile elements associated with D. tsuruhatensis, including insertion sequenced, genomic islands and prophage with multiple types observed of each element and in some instances, calculations suggesting they composed up to 10 % of the larger species genome. CRISPR loci, that defend the species against mobile element and prophage invasion, were also reported. Yin et al. concluded that such mobile elements contributed to the genomic diversity of D. tsuruhatensis [39].
Virulence factors
1.4
Macromolecular secretion systems, capable of DNA and protein secretion and often associated with virulence were also discovered during the pan genome analysis including type I (T1SS), II (T2SS), IV (T4SS), VI (T6SS), IV (T4P), flagellum and Tad pilus secretion systems. Although their roles in D. tsuruhatensis have yet to be identified, many may play a role in pathogenicity [39]. Analysis of putative virulence genes amongst the genome comparison revealed 112 gene families, matched with virulence genes in the PHI-base database, some 80 of which were present in most of the genomes. The genes identified were predicted to be related with determining nosocomial infections, such as urinary tract infection, meningococcal infection, gastric infections, bloodstream infection, skin infection, and prosthetic joint infection, supporting the proposition of D. tsuruhatensis as an emerging opportunistic pathogen particularly in immunocompromised hosts [39]. Another study undertaken out by Andriyanov et al., identified multiple virulence factors homologs in the genomes of Delftia spp. Each strain was found to have 24 to 31 putative virulence factors genes. These genes were involved in motility, adherence, immune modulation, stress survival, secretion systems, siderophores and general cellular fitness [40]. Delftia acidovorans has been found to form biofilm that are resistance to Chlorhexidine [41,42].
Methodology
2
All accessible publications (journal articles, medical case reports and conference proceedings) discussing Delftia spp infections were recovered using PubMed, Web of Knowledge and Google Scholar. The terms ‘Delftia’, ‘Delftia’ spp.’ ‘Comamonas acidovorans’, ‘Pseudomonas acidovorans’ (previous names of Delftia acidovorans) and Delftia species recorded in Table 1 were all investigated from January 1976 until January 2026. Any publications that examined human infection were reviewed and the desired information extracted from them. The information (where available) obtained included year, geographic location, patient information (age, sex, any underlying medical condition[s]), antimicrobial susceptibility, treatment (antibiotics, catheter removal, etc) and patient outcomes (recovery, death, etc.). This was used to populate Table 2, Table 3, Table 4, Table 5. The references cited in these publications were also checked for any infection reports that were not found in the database searches.Table 1. Listing of validly published Delftia species.Table 1. SpeciesIsolation siteOriginGenome sequencesReferenceDelftia acidovoransThe NetherlandsSoil enriched with acetamideStrain: SPH-1,Wen et al., 1999 [28]Size: 6.767 MbRef Genome: CP000884.1 (47 genomes)Delftia desertiChinaDesert soil sampleStrain: KCTC42377,Li et al., 2015 [32]Size: 7 MbRef Genome: JBHUIG000000000Delftia lacustrisDenmarkFresh water lakeStrain: LZ-CJørgensen et al., 2009 [30]Size: 7 MbRef Genome: GCF_001017795.1 (9 genomes)Delftia litopenaeiTaiwan/Fresh water shrimp pondN/AChen et al., 2012 [31]Delftia rhizosphaeraeSpainRhizosphere of Cistus ladanifer plantN/ACarro et al., 2017 [33]Delftia tsuruhatensisJapanActivated.Strain: 391Shigematsu et al., 2003 [29]Size: 6.7 MbRef Genome: GCF_001017795.1 (9 genomes)Table 2. Incidences of D. acidovorans infection from 1976 to 2025– Main characteristics of the case reports.Table 2. Author (Ref)YearLocationAge/SexCo-morbidityType of infectionAntibiotic ResistanceAntibiotic SusceptibilityTreatmentPatient outcomeWeinstein et al., [53]1976USAN/AN/ABacteremiaN/AN/AN/AComplete recoveryBrinser and Torczynski [60]1977USA60/FNoneCorneal ulcersAmpicillin, Bacitracin, Carbenicillin Cephalothin, PenicillinColistin, Gentamicin, Neomycin, Polymyxin B Tetracycline sulfonamide,Carbenicillin Gentamicin Along with topically applied gentamicin, colymycin, and 1 % atropine.Complete recoveryHorowitz, et al., [25]1989USA42/FIntravenous drug user and alcohol abuseEndocarditisAmikacin, Ampicillin, Cefazolin, Cefuroxime, Gentamicin, Ticarcillin, Tobramycin,Aztreonam, Cefoxitin, Cefoperazon, Ceftazidime, Cefotaxime, Ceftriaxone, Chloramphenicol, Ciprofloxacin Mezlocillin, Piperacillin, SXTPenicillin, Ceftazidime, oral ciprofloxacin, Vancomycin and amphotericin BDeathReina et al., [61]1991Spain7/MNoneSuppurative OtitisAmpicillin, Cefazolin, Cefuroxime, Carbenicillin, GentamicinAmikacin, Aztreonam Cefotaxime, Ceftazidime, Ceftriaxone, Chloramphenicol, Ciprofloxacin, Imipenem, Tobramycin, SXTCeftazidimeComplete recoveryStonecipher et al., [62]1991USA48/FNoneOcular InfectionAmpicillin, Cefazolin, GentamicinTobramycinGentamicin Followed by TobramycinComplete recoveryStonecipher et al., [62]1991USA57/FNoneOcular InfectionN/AN/Aprednisolone acetate eyedropsComplete recoveryStonecipher et al., [62]1991USA76/FNoneOcular InfectionN/AN/AOral doxycycline and topical erythromycin Followed by Polymixin BComplete recoveryStonecipher et al., [62]1991USA16/FNone Acinetobacter calcoaceticusOcular InfectionN/AGentamicin sulfateGentamicin sulfateComplete recoveryStonecipher et al., [62]1991USA32/MNone Bacillus cereus, Flavobacterium spp*. Acanthamoeba*Ocular InfectionN/AN/APropamidine, gramicidin, Scopolamine hydrobromideComplete recoveryStonecipher et al., [62]1991USA26/WNone AcanthamoebaOcular InfectionN/AN/AN/AComplete recoveryCastagnola, et al., [63]1994Italy9/MNon-Hodgkin's LymphomaCentral venous catheter related infectionBroad spectrum penicillin's, GentamicinArninoglycosides, Carbapencrns, Cephalosporins, Monobactam, Quinolones, SXT,Ceftazidime, Vancomycin. Changed to Amikacin. Removal of catheter.Complete recoveryEnder, et al., [64]1994unknown4/FMetastatic neuroblastomaVascular Catheter related BactereamiaAll aminoglycosidesAztreonam, Cephalosporins, Ciprofloxacin, Piperacillin, TicarcillanCeftazidime therapy, intravenous ciprofloxacin, ceftriaxone, cephalosporin and the catheter was removedComplete recoveryLair, et al., [65]1996France27/MHIV/AIDS Oerskovia turbataBactereamia associated with a central venous catheterAmikacin, Cefsulodin, Colimycin, Gentamicin, TicarcillinCeftazidime, Imipenem Piperacillin, PefloxacinCatheter removed, Imipenem (500 mg twice daily) and Amikacin (400 mg)Complete recoveryLópez-Menchero, et al., [66]1998Spain35/FEnd-stage renal disease secondary to chronic glomerulonephritis, with a single kidney, was included in the CAPDPeritonitsN/AN/AOral ciprofloxacin (750 mg/12 h for 14 days), 1 g ceftazidime IP daily. piperacillin to the treatment (4 g/12 h, intravenous). Peritoneal catheter was removed.Complete recoveryOjeda-Vargas, et al., [67]1999Gran Canaria61/MHemiplegiaUrinary tract infectionAmikacin, Ampicillim, Fosfomicin, TobramycinAztreonam, Cefotaxime, Ciprofloxacin, Imipenem, Norfloxacin, Ticarcillin, SXTTwo-week course of Norfloxacin (400 mg orally twice daily)Complete recoveryPerla & Knutson [68],2005USA35/MIntravenous drug abuserBactereamia associated with a contaminated needleGentamicinCeftazidime, Cefotaxime, Ceftriaxone, Imipenem, Levofloxacin, Piperacillin -Tazobactum, SXT10 days of LevofloxacinComplete recoveryOliver, et al., [69]2005USA30/MHealthy male went to hospital after receiving a gunshot wound Ochrabactrum anthropiBactereamiaTobramycinAztreonam, Cefepime, Cefotaxime, Ceftazidime, Ceftriaxone, Ciprofloxacin Piperacillin and Piperaciliin-Tazobactum, SXTMetronidazole 500 mg IV QI, Piperacillin- Tazobactam 3.375/0.375 g IV QID Followed by Cefepime (2 g IV BID for 3 days) Ciprofloxacin (400 mg IV BID for 8 days) Imipenem (1 g IV for 7 days).Complete recoveryChun, et al., [70]2009Seoul, South Korea53/MSmoker. Previous injury that resulted in developing Pleural effusion. Chronic Empyema in lungs.Bacteraemia (Cathether related)Amikacin, Gentamicin, TobramycinCefotaxime, Ceftazidime, Cefepime, Imipenem Piperacillin-Tazobactam, SXTIV Moxifloxacin started. Changed to Imipenem -Cilastin (500 mg 6 h) and both catheters were removed.Complete recoveryKawamura, et al., [71]2010Japan11/FMetastatic neuroblastomaBacteraemia (Cathether related)Amikacin, Cefepime, Cefozopran, Gentamicin, Piperacillin, TobramycinCeftazidime, Ciprofloxaicn, Imipenem, Merpenem, Minocycline, SXTeftazidime, removal of the catheterComplete recoveryMahmood, et al., [72]2010Kentucky, USA30/MIntravenous drug use, Hepatitis C, and posttraumatic stress disorder.Acute infective EndocarditisAminoglycosides, Colistin, Cefazolin, CefepimeCeftazidime, Carbapenems, Fluoroquinolones, Piperacillin-Tazobactam, Tetracycline, SXTVancomycin, piperacillin-tazobactam changed to ceftriaxone,Complete RecoveryChotikanatis et al., [73]2011New York USA10/FRenal cortical necrosis and end-stage renal diseaseBacteraemia (Cathether related)Aminoglycosides, Penicillin, Narrow-spectrum cephalosporinsExpanded-spectrum and broad-spectrum Cephalosporins, Aztreonam, Carbapenems, Piperacillin-Tazobactam, Quinolones Ticarcillin-Clavulanate,14-day course of cefepime. 14-day course of Ceftazidime for second episodeComplete recoveryKam et al. [74]2011Taiwan93/MBenign prostate hyperplasia with obstructive uropathyBactereamia associated with an ascending Urinary tract infection.Cefepime, Cefoxitin, Cefuroxime, Cefoperazone, Ceftriaxone, Ciprofloxacin, Gentamicin, Levofloxacin, Netilmicin, Norfloxacin, Ofloxacin, Piperacillin, Piperacillin -Tazobactam, SXT, Tigecycline, Ticarcillin, TobramycinCefoperazone – Sulbactam, Imipenem, Merpenem,Cefoperazone/Sulbactam (1g/1g) for 6 h through IV. Followed by Imipenem 500 mg through IV for 6 hComplete RecoveryLang, et al., [26]2011India65/MNK cell lymphoma CorynebacteriumLine related sepsisAminoglycosidesCarbapenems, Cefatzidime, Ciprofloxacin, Piperacillin-Tazobactam, TrimethoprimPiperacillin-Tazobactam, Gentamicin Patient had Hickman line removed Followed by Imipenem- Cilastatin, TeicoplaninComplete recoveryKhan, et al., [75]2012India4/FNoneEmpyemaGentamicin, Ceftazidime, Tetracycline, MeropenemCefoperazone-SulbactamCefoperazone-sulbactamDeath (Septic Shock)Hagiya, et al., [76]2013Japan46/FOrganophosphorus poisoningBactereamia caused by bacterial translocation after organophosphorus poisoningCefepime, Gentamicin, PiperacillinAmikacin, Aztreonam, Ceftazidime, Ciprofloxacin, Imipenem, Levofloxacin Meropenem, Minocycline, Ppiperacillin -Tazobactam, SXTAmpicillin - Sulbactam Followed by Ppiperacillin -TazobactamComplete recoveryRay & Lim [77],2013Singapore14/FNo pre-existing medical condition Chryseobacterium meningosepticumKeratitis associated with a Cosmetic contact lenses which caused a para-central corneal ulcerAmpicillin, Ceftazidime, Ceftriaxone, Piperacillin.Ciprofloxacin, GentamicinCefazolin (50 mg/mL) and gentamicin (14 mg/mL) eyedrops Followed by CiprofloxacinComplete recoveryCamargo et al., [78]2014BrazilMultiple (21 Cases)N/ALung problemsAmikacin, Gentamicin TobramycinCefotaxime, Cefepime, Imipenem, LevofloxacinN/AN/AKhan and Krishnan [79]2014Australia70/MType II Diabetes mellitus, Heart failure, COPDSkin InfectionAmikacin, Amoxicillin, Gentamicin TobramycinCiprofloxacin, SXTOral ciprofloxacinComplete recoveryLu and Huang [44]2014–2022Taiwan60/M2PneumoniaAmikacin, GentamicinCeftazidime, Ciprofloxacin, Imipenem, Meropenem, Piperacillin- TazobactamPiperacillin- TazobactamComplete recoveryLu and Huang [44]2014–2022Taiwan80/F3PneumoniaAmikacin, Cefepime, Ciprofloxacin GentamicinCeftazidime, Imipenem, Meropenem, Piperacillin- TazobactamCefepimeComplete recoveryLu and Huang [44]2014–2022Taiwan73/M2PneumoniaAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCefepimeComplete recoveryLu and Huang [44]2014–2022Taiwan84/F3PneumoniaAmikacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan88/M2PneumoniaAmikacin, GentamicinCeftazidime, CefepimeImipenemComplete recoveryLu and Huang [44]2014–2022Taiwan58/M0PneumoniaAmikacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan80/M2PneumoniaAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan84/F2PneumoniaAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamImipenemComplete recoveryLu and Huang [44]2014–2022Taiwan90/F4PneumoniaN/AN/ACefepimeDeathLu and Huang [44]2014–2022Taiwan37/F2PneumoniaAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan87/F2PeritonitisAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftibutenComplete recoveryLu and Huang [44]2014–2022Taiwan55/M3PeritonitisAmikacin, Cefepime, GentamicinCeftazidime, Imipenem, MeropenemCefepimeComplete recoveryLu and Huang [44]2014–2022Taiwan89/F2BacteraemiaAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamAmpicillin - SulbactamComplete recoveryLu and Huang [44]2014–2022Taiwan51/M3BacteraemiaAmikacin, Ceftazidime, Cefepime, Gentamicin, Imipenem, Meropenem, Piperacillin- TazobactamCiprofloxacinAmoxicillin -Clavulanic acidComplete recoveryLu and Huang [44]2014–2022Taiwan78/M2BacteraemiaAmikacin, Cefepime, Ciprofloxacin, GentamicinCeftazidime, Imipenem, Meropenem, Piperacillin- TazobactamImipenemComplete recoveryLu and Huang [44]2014–2022Taiwan89/M1BacteraemiaCeftazidime, Cefepime, Piperacillin- TazobactamAmikacin, Ciprofloxacin, GentamicinCiprofloxacinDeathLu and Huang [44]2014–2022Taiwan70/M3Liver abscessAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamImipenemComplete recoveryLu and Huang [44]2014–2022Taiwan72/M4Urinary Tract InfectionAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamAmpicillin-SulbactamComplete recoveryLu and Huang [44]2014–2022Taiwan83/M2Urinary Tract InfectionAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan77/M3Urinary Tract InfectionAmikacin, Ceftazidime, Cefepime, Ciprofloxacin, Gentamicin, Meropenem, Piperacillin- TazobactamImipenemNoneComplete recoveryLu and Huang [44]2014–2022Taiwan56/F1Urinary Tract InfectionAmikacin, GentamicinCeftazidime, Cefepime, Ciprofloxacin, Imipenem, Meropenem, Piperacillin- TazobactamNoneComplete recoveryLu and Huang [44]2014–2022Taiwan67/M3Urinary Tract InfectionAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan83/F3Urinary Tract InfectionAmikacin, GentamicinCeftazidime, Cefepime, Ciprofloxacin, Imipenem, Meropenem, Piperacillin- TazobactamNoneComplete recoveryLu and Huang [44]2014–2022Taiwan79/M2Urinary Tract InfectionAmikacin, GentamicinCeftazidime, Cefepime, Ciprofloxacin, Imipenem, Meropenem, Piperacillin- TazobactamMeropenemDeathLu and Huang [44]2014–2022Taiwan62/M3Urinary Tract InfectionAmikacin, GentamicinCeftazidime, Cefepime, Ciprofloxacin Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryLu and Huang [44]2014–2022Taiwan71/F2Urinary Tract InfectionAmikacin, Ciprofloxacin, GentamicinCeftazidime, Cefepime, Imipenem, Meropenem, Piperacillin- TazobactamCeftazidimeComplete recoveryBilgin, et al., [80]2015Canada68/FB cell acute lymphocytic leukaemiaBactereamia associated with pneumoniaAmikacin, Ampicillin-Sulbactam, Gentamicin, Ciprofloxacin, ColistinExpanded- and broad-spectrum Cephalosporins, Carbapenems, Piperacillin-TazobactamPiperacillin-Tazobactam −4.5 g/6 h, Ciprofloxacin, 400 mg/12 hComplete recoverySharma et al. [81]2015IndiaNeonate/MNeonateUmbilical infectionCeftazidime, Piperacillin -Tazobactum, SXTAmikacin, Gentamicin, Imipenem, Meropenem, Piperacillin -Tazobactum, TobramycinMeropenem, Reicoplanin and FluconazoleComplete RecoveryPatel, et al., [82]2019USA49/FIntravenous drug abuse Vertebral osteomyelitisSeptic pulmonary embolism (catheter-related infection)All aminoglycosidesPpiperacillin-TazobactamIV Piperacillin- Tazobactam. Catheter removal.Complete RecoveryYildiz, et al., [83]2019Turkey52/FThrombocytopenic purpura (immuno-suppressive therap), Diabetes mellitus.Pneumonia with lung cavities formationAmikacin, Cefepime, Ciprofloxacin, Colistin, Gentamicin, Netilmicin.Ceftazidime, Imipenem, Ppiperacillin Ppiperacillin-TazobactamIV piperacillin-tazobactam (4.5 g does 3 times/day) and oral clarithromycin (500 mg 2 times/day)Complete recovery.Smits, et al., [84]2020Germany60/FNoneInfection of the orbital after a cat scratch 34 months earlierN/AN/APpiperacillin - Tazobactam 3 × 4.5 g/d IV for 10 days.Complete recoveryDeb, et al. [85]2020India67/MNone Post cataract surgeryPost-operative EndophthalmitisN/ACeftazidime, Ceftriaxone, Cefoperazone -Sulbactam, Chloramphenicol, Levofloxacin, Meropenem.Started on intravitreal vancomycin (1 mg/0.1 mL) and ceftazidime (2.25 mg/0.1 mL). Followed by IV Cciprofloxacin 200 mg twice a day, topical moxifloxacin drops hourly, Followed by Ceftazidime (2.25 mg/0.1 mL) injectionComplete recoveryArtan et al., [86]2020Turkey60/Mend-stage kidney disease, DiabetiesPeritonitisAminoglycosides, Colymicin aQuinolones, Ceftazidime, SXT1 g of cefazol and 1 g of ceftazidim daily Added Oral Ciprofloxacin 500 mg/dayComplete recoveryErtan and Yılmaz [87]2020Turkey4 month old/FCongenital Heart Disease Klebsiella pneumoniaeSepsisN/AN/ACefepimeDeathPerumal et al., [88]2020India57/MHIV Positive Enterococcus faeciumPleural EffusionAminoglycosides, FluroquinolnesCefaperazone-Sulbactam, Doripenem, Imipenem, Meropenem Piperacillin-TazobactamIV Cefoperazone-sulbactamComplete recoveryPeters et al., [89]Stenotrophomonas maltophilia2020USA62/FHypertension, COPDNecrotizing pneumoniaN/ALevofloxacin, SXTCefepime and Vancomycin Followed by Ampicillin-SulbactamComplete recoveryHøjgaard et al. [43]2002–2022DemarkMultiple (59 Cases – 35 Male/24 Fenale)Multiple (bone marrow transplant recipient; cardiovascular diseases, chronic obstructive pulmonary disease; congenital syndromes; connective tissue disease; cystic fibrosis; Diabetes mellitus; hematologic malignancies; interstitial lung disease; liver disease; neuromuscular disease; primary ciliary dyskinesia; renal dysfunction; solid cancer; solid organ transplant recipient)InfectionsColistin, Gentamicin, TobramycinCeftazidime, Ciprofloxacin Imipenem, Meropenem, Piperacillin-TazobactamFluoroquinolones MeropenemNot determinedSingh et al., [90]2022India29/FBreast CancerSepsisAmikacin, ColistinAztreonam, Ceftazidime, Ciprofloxacin, Meropenem, Levofloxacin, Piperacillin -TazobactumMeropenem, Amphotericin B, TeicoplaniDeathLall et al. [91]2023India35/MAdenocarcinomaPleural EffusionGentamicinCeftazidime, Cefoperazone Sulbactam, Ciprofloxacin, Levofloxacin, Piperacillin- TazobactamCiprofloxacin 500 mgComplete recoveryAgarwal et al. [46]2023IndiaNew Born/MNoneBacteraemiaAmikacin, Ciprofloxacin, Colistin, Gentamicin,Carbepenems, Cephalosporins, Piperacillin–TazobactamAmpicillin and GentamcinDeathAlam et al., [92]2023IndiaNeonatePneumoniaSepsisAmikacin, Cefepime, Colistin, Piperacillin- TazobactamCeftazidime, Cefoperazone-Sulbactam, Ciprofloxacin, Levofloxacin MeropenemCiprofloxacin, MeropenemComplete recoveryBackman et al., [93]2023USAM/35Membrano-proliferative glomerulonephritisBacteraemiaN/AN/AN/AComplete recoveryBackman et al., [93]2023USAM/50DiabetiesBacteraemiaN/AN/AN/AComplete recoveryPeykov et al., [55]2024Bulgaria65/FNoneBronchitisColistin, GentamicinAmikacin Imipenem, Meropenem, Tobramycin.Oral Levofloxacin, starting 500 mg twice daily for five days, followed by 500 mg once daily for ten days.Complete recoveryJaya et al., [94]2025India16 month old/FEczemaAxillary AbscessCeftazidime, PiperacillinAmikacin, Cefoperazone, Ciprofloxacin, Gentamicin, Imipenem, Meropenem, Netilmicin, Tetracycline, SXTInintravenous (IV) cloxacillin 200 mg/kg/d and IV clindamycin 40 mg/kg/d Followed by IV clindamycin was ceased and IV ceftriaxone 100 mg/kg/d Followed by oral flucloxacillin Followed by oral ciprofloxacin 40 mg/kg/dComplete recoveryScaglione et al., [95]2025Italy61/MHypertension, Stroke, Epilepsy, End Stage Kidney DiseaseSeptic shock (cathether related)AminoglycosidesCephalosporins, Fluoroquinolones, Piperacillin–TazobactamMeropenem and Vancomycin Followed by Piperacillin–TazobactamComplete recoveryGordon and Marin [47]2025USA78/FSmoker, Stroke, Peripheral Artery Disease, Type 2 Diabetes mellitus, HypertensionPneumoniaGentamicinN/ALevofloxacin and MinocyclineDeathM − Male, F- Female, N/A – Not Available, Lu and Huang did not list Co-morbidities, only giving the number of them, however they say that they were a combination of “cardiovascular diseases, malignancies, diabetes mellitus, cerebrovascular diseases, chronic kidney disease or end-stage renal disease, chronic obstructive pulmonary disease, autoimmune rheumatic diseases, and hepatitis B or C”.Table 3. Incidences of D. lacustris infection from 2012 to 2024– Main characteristics of the case reports.Table 3. ReferenceYearLocationAge/sexPre-existing medical conditionType of infectionAntibiotic resistanceAntibiotic SusceptibilityTreatmentPatient outcomeShin, et al., [96]2012Germany66/MAlcoholic and chain smoker.EmpyemaGentamicinAmikacin, Aztreonam, Ceftriaxone, Cefepime, Ceftazidime, Imipenem, LevofloxacinImipenemComplete RecoveryShin, et al., [96]2012Germany70/MBenign prostate hypertrophy and Angina pectoris. Patient went to Hospital with a renal injury.UnknownGentamicinAmikacin, Aztreonam, Ceftriaxone, Cefepime, Ceftazidime, Imipenem, LevofloxacinNo antibiotic TreatmentComplete recoveryShin, et al., [96]2012Germany40/MHepatocellular carcinomaUnknownCeftriaxone, Cefepime, Ceftazidime, Amikacin, Aztreonam and GentamicinImipenem, LevofloxacinCefotaximeDischarged in a grave conditionShin, et al., [96]2012Germany67/MCOPD, Myocardial infarction.UnknownAmikacin, Cefepime, GentamicinAztreonam, Ceftriaxone, Ceftazidime, Imipenem, LevofloxacinNo antibiotic TreatmentComplete recoverySohn & Baek [97],2015South Korea67/MDiabetes mellitus, Hypertension. PheochromocytomaBactereamia caused by peripheral intravenous catheter which led to septicaemiaAminoglycosides, Ciprofloxacin, Ticarcillin,SXTAztreonam, Cefotaxime, Ceftazidime, Piperacillin CarbapenemsIv Cefazolin. Followed by Piperacillin -TazobactamComplete recoverySohn, et al., [98]2015South Korea70/MPatient was taking anti-hypertensive pills and anti-diabetic pills.KeratitisAmikacin, GentamicinAztreonam, Cefepime, Ceftazidime, Ciprofloxacin, Imipenem, Meropenem, Piperacillin -Tazobactam, Ticarcillin -Clavulanic acidFortified topical Ofloxacin, Voriconazole, Gentamicin Followed by topical Ciprofloxacin, systemic CeftazidimeEvisceration (Eye removal)Cousillas et al., [99]2024Spain78/MChronic Kidney Disease, Hypertension, Dyslipidemia, and Type 2 Diabetes MellitusPeritoneal infectionsN/AN/AIntraperitoneal Vancomycin 2 g and gentamicin 80 mg, Meropenem, Cathather RemovalComplete recoveryTable 4Incidences of D. tsuruhatensis infection from 2012 to 2024– Main characteristics of the case reports.Table 4. ReferencesYearLocationAge/SexPre-existing Medical ConditionType of infectionAntibiotic resistanceAntibiotic SusceptibilityTreatmentPatient outcomePreiswerk, et al., [100]2012Switzerland53/FIdiopathic pulmonary hypertensionBactereamia (Catheter-related)Amikacin, Ampicillin, Cephalothin, Cefuroxime, Colistin Gentamicin, TobramycinAmoxicillin–Clavulanate, Ceftriaxone, Ceftazidime, Cefotaxime, Cefepime, Ciprofloxacin, Ertapenem Levofloxacin, Imipenem, Meropenem, Piperacillin–Tazobactam,Oral CiprofloxacinComplete recoveryRanc, et al., [27]2008Marseille, France77/MLiver cancer, colic adenocarcinomaConsidered by physicians as colonizationN/AN/AN/AComplete recoveryRanc, et al., [27]2009Marseille, France70/FImmunocompromisedunknownN/AN/AN/AComplete recoveryRanc, et al., [27]2010Marseille, France59/FAlcoholism which led to chronic end-stage renal failureCatheter-related bloodstream infection; (Septicaemia)N/AN/AGentamicin Piperacillin-TazobactamComplete recoveryTabak, et al., [101]2010Turkey53/FMetastatic breast cancerBactereamia (Port-related)N/AThird generation cephalosporins, Cefepime, Quinolones, and beta-lactamase inhibitorsCeftriaxone 1 g/day for 14 daysComplete recoveryRanc, et al., [27]2010Marseille, France6/MCystic fibrosisunknownN/AN/AN/AComplete recoveryRanc, et al., [27]2013Marseille, France42/MChronic renal failure, alcoholic Hepatitis CunknownN/AN/AN/AComplete recoveryRanc, et al., [27]2014Marseille, France13/FLiver transplantPost-transplant fever;N/AN/APiperacillin -TazobactamComplete recoveryRanc, et al., [27]2015Marseille, France82/MHaemodialysis, vascular dementiaCatheter-related bloodstream infection; (Septicaemia)N/AN/ACeftazidimeComplete recoveryRanc, et al., [27]2015Marseille, France47/MKidney transplantFever (Bactereamia)N/AN/AN/AComplete recoveryRanc, et al., [27]2015Marseille, France6 months/FPreterm birthVentilator-associated pneumonia;Amoxicillin, Amoxicillin- ClavulanateCeftriaxone, Ertapenem, Imipenem, OfloxacinCeftazidime, Followed by Imipenem, Vancomycin Amikacin Followed by TobramycinDeathCheng et al., [49]2019China91/MN/ARrespiratory failureAmpicillin, Cefazolin, Amikacin, Ampicillin, Cefazolin,Gentamicin, Netilmicin, Streptomycin, Tetracycline, SXT, TobramycinAzithromycin, Aztreonam, Cefoxitin, Ceftriaxone, Ceftazidime, Cefepime, Chloramphenicol, Ciprofloxacin, Florfenicol, Levofloxacin, ImipenemN/AN/ACho et al., [48]2019Korea65/MStomach cancer (Total gastrectomy)FeverAmikacin, Ceftazidime, Cefepime, Ceftriaxone, Levofloxacin, MeropenemMinocycline, Piperacillin-TazobactamCiprofloxacin Followed by Piperacillin-TazobactamComplete recoveryTable 5Incidences of Delftia sp infection from 2015 to 2024– Main characteristics of the case reports.Table 5. ReferencesYearLocationAge/SexPre-existing Medical ConditionType of infectionAntibiotic resistanceAntibiotic SusceptibilityTreatmentPatient outcomeKang, et al., [48] Delftia sp. 6702015China33/MHIV, Pulmonary infection, respiratory failure and a spinal deformityBactereamia associated with pneumoniaAmikacin, Ampicilin, Cefuroxime-sodium, CefazolinAztreonam, Cefepime, Cefotetan, Ceftazidime, Ceftriaxone, Ciprofloxacin, Levofloxacin, Imipenem, Meropenem, PiperacillinN/ADeath after 10 days(Böttger, et al., [102])2020Germany23/FNoneChronic Wound Infection after Wisdom Tooth Extraction 6 months earlierN/AN/AN/AComplete recovery
Delftia Infections
3
Delftia spp instances of infection
3.1
All recorded instances of infection with Delftia spp in humans from the scientific and medical literature can be found in Table 2 (D. acidovorans), 3 (D. lacustris), 4 (D. tsuruhatensis) and 5 (unidentified Delftia sp.). No instances of infection have been reported with the other three recognised Delftia species. These tables show the date (year) of infection (if unavailable publication year was used instead), geographic location (country was used as in most cases no smaller geographic information was given) of infection, information on the patient(s) [age, gender, prior health conditions], infection type (bacteraemia, meningitis, etc) caused by the Delftia sp infection, antibiotic susceptibility testing undertaken (both susceptibility and resistance were recorded where available), handling of infection (this focused primarily on the antibiotic treatments used and removal of any indwelling devices) and patient outcome (recovery, death, etc.).
Table 2, Table 3, Table 4, Table 5 show 175 separate instances of infection caused by Delftia spp. that were found in literature sources. Most of these infections were caused by Delftia acidovorans (153 instances – 87.4 %), other infections were due to Delftia lacustris (7 instances – 4 %), Delftia tsuruhatensis (13 instance – 7.4 %) and Delftia sp (2 instance – 1 %.). Many of the cases of Delftia acidovorans come from two large scale retrospective studies carried out by Højgaard et al. (2002–2022) [43] and Lu and Huang (2014–2022) [44].
132 (75.9 %) of the patients were found to have either one or more prior health conditions (either chronic or acute). Seventeen (9.8 %) of the patients were found to have no prior health conditions and for 25 patients (14.4 %) no information was provided/available. Sixty-Seven patients had one prior medical condition, and all other patients had two or more. By far the biggest pre-existing medical conditions were various different types of cancer (in 46 patients – 26.4 %), cardiovascular disease (in 33 patients – 19 %), Diabetes mellitus (in 13 patients – 7.5 %), HIV (in 3 patients – 1.7 %) and intravenous drug use (in 3 patients – 4.3 %). A full list of pre-existing medical conditions can be seen in Table 2, Table 3, Table 4, Table 5 Multiple different infection types were caused by the different Delftia species including pneumonia, bacteraemia, sepsis/septic shock, endocarditis and ocular infections.
The majority of cases were successfully treated with antibiotics and completed full recovery, 10 cases (14.5 %) either had no antibiotic usage or no recorded antibiotic usage and had a complete recovery, 11 patients (11.6 %) died, one patient with keratitis had to have the infected eye eviscerated. Patients who died due to Delftia spp. infection (Sepsis, pneumonia, empyema and endocarditis) had at least one pre-existing medical condition bar one patient (discussed below). No pseudo-outbreaks have been so far found associated with Delftia spp.
Mortality associated with Delftia spp. infection
3.2
Eleven instances of death associated with Delftia spp. infection have been recorded in the literature. Nine cases were linked to D. acidovorans (Table 2), one to D. tsuruhatensis (Table 4) and one to an unidentified Delftia spp (Table 5). No deaths have been associated with D. lacustris (Table 3). The first instance of death was recorded by Horowitz, et al., the patient in this case was an intravenous drug user and alcoholic [25]. The patient a 42-year-old female contacted D. acidovorans related endocarditis and later died. A second death was recorded in a 4-year-old female patient. She died of D. acidovorans related septic shock [45]. The D. acidovorans infection was related to an indwelling device*.* The third death was associated with D. acidovorans was a a case of sepsis in a 4 month female. She suffered from congenital heart disease. The fourth case of death assocatied with D. acidovorans was sepsis in a 29 year old female paitent undergoing chemotherapy for breast cancer. The fifth case was in a newborn male who contracted bacteremia [46]. The sixth case of death associated with D.acidovroans was in a 78 year old woman who died of pneumonia. She has multiple underlying conditions (Peripheral Artery Disease, Type 2 Diabetes, Hypertension). The infection was catheter related [47]. Three death were found in the retrospective study carried out by Lu and Huang. All three patients had cancer and death due to UTI, bacteremia and pneumonia [44]. Several deaths occurred in the study carried out by Højgaard et al. however these could not be linked directly to Delftia acidovornas infection [43]. Ranc et al., recorded a death due to ventilator-associated pneumonia; assoicated with D. tsuruhatensis in a 6 month old female who had been born prematurely [27]. A case of death due to severe pneumonia has also been linked to Delftia sp 670 in a 33 year old HIV Positive male [48].
Treatment of Delftia spp. infections
3.3
Delftia species have been shown to be resistant to many of the major antibiotic groups [[49], [50], [51]] (Cho et al., 2021; Cheng et al., 2021). This can cause complications when attempting to treat infections with this genus. Antibiotic treatment on Delftia spp. must be based on in vitro susceptibility testing carried on the infectious isolates. A wide array of antibiotics has been used to treat Delftia spp. infections. In most cases, Delftia spp. are susceptible to ceftazidime, ciprofloxacin and imipenem (based on Antibiotic Susceptibility testing data from the literature see Table 2, Table 3, Table 4, Table 5). Multiple isolates showed resistance to gentamicin so this should be avoided in treating Delftia infections. These results broadly agreed with the results of a major retrospective study carried out by Højgaard et al., on D. acidovorans that examined 18 years' worth of infections at a tertiary referral hospital in Copenhagen, Denmark, and the results of another retrospective study carried out by Lu and Huang that examined eight years' worth of infections in a hospital in a Taiwanese hospital [43,44]. Højgaard et al., found that meropenem or ceftazidime were the most effective antibiotics against D. acidovorans with ciprofloxacin and imipenem also proving to be effective and that the majority of isolates tested were resistant to gentamicin [43]. Lu and Huang found similar results with most isolates susceptible to meropenem and ceftazidime along with piperacillin-tazobactam and resistant to gentamicin. However, a major difference can be seen when it comes to ciprofloxacin where they found most of the isolate's resistance to the antibiotic [44].
The genetic basis for antibiotic resistance in Delftia sp Genome analysis of a D. tsuruhatensis pathogenic isolate identified 17 resistance genes including aminocyclitols (aadA2b), fluoroquinolone (aac(6′)-Ib-cr), aminoglycosides (aph(3′')-Ib, aph(6)-Id aac(6′)-Ib3, aac(6′)-Ib-cr, and aadA2b), folate pathway antagonist (sul1, sul2, and dfrA16), tetracycline (tet(G)), and phenicol (cmx and floR) [39], however resistance was not found in all strains supporting the conclusion of these strains evolving and adapting via horizontal gene transfer and adaption. A strain of D. tsuruhatensis MR-6/3H from cow milk was found to be resistant to 19 antibiotics of 23 tested. This included all aminoglycosides, phenicols, to trimethoprim-sulfamethoxazole and most β-lactams. Comparative genomic analysis revealed putative antimicrobial resistance genes mostly associated with antibiotic efflux systems [40]. The emergence of resistant determinants in these Delftia species may thus have clinical relevance for this species.
Infection prevention
3.4
Infections caused by Delftia species, are sporadic but are medically significant as they are primarily healthcare-associated. Nosocomial cases are normally associated with environmental reservoirs and indwelling medical devices reflecting the ability of Delftia species to persist in aqueous environments and form biofilms [41,42]. Hospital water systems, and contaminated fluids or equipment have all been shown as potential sources of infection [52]. Due to this infection prevention in healthcare settings should prioritise water system management, strict aseptic technique during catheter insertion and maintenance, and the removal of unnecessary intravascular lines. Isolation of Delftia spp from sterile sites should not be dismissed as contamination, as delayed recognition may inhibit correct infection-control interventions.
Community-acquired Delftia infections are uncommon and normally occur in individuals that have underlying medical conditions. Prevention outside healthcare settings depends on more general control measures, such as good personal hygiene, proper wound care, and safe handling of water in home-care or outpatient medical settings, instead of organism-specific public health strategies.
Surveillance and epidemiology of delftia species
3.5
Epidemiological data on Delftia species is highly limited. The data that is available comes mostly from descriptions in medical case reports and form retrospective laboratory analyses (Table 2, Table 3, Table 4, Table 5) rather than from surveillance programmes. Delftia spp are not commonly included in national or international surveillance programmes. They are usually included with other non-fermenting Gram-negative bacteria, which may lead to underestimation of incidences and of clinical significance [27,53]. The use of MALDI-TOF MS and whole-genome sequencing (WGS) has significantly improved identification of non-fermenting Gram-negative bacteria including Delftia spp, aiding to more regular identification of clinically relevant isolates in recent years [[54], [55], [56]].
With no Delftia-specific surveillance frameworks, approaches that have been developed for other opportunistic non-fermenting Gram-negative bacteria such as Pseudomonas aeruginosa, Acinetobacter baumannii, and the Burkholderia cepacia complex maybe appropriate. These include laboratory-based surveillance linked to clinical data, separation of community-acquired and healthcare-associated infections, and environmental surveillance of hospital water systems and medical devices [57,58]. Such methodologies are particularly appropriate given Delftia's environmental persistence.
Conclusions
4
Although Delftia species are not thought of as major human pathogens, the evidence indicates that they represent rare opportunistic causes of infection, with approximately 175 cases reported across the global over several decades. This support the view that Delftia spp. are uncommon, generally low-virulence organisms. The clinical outcomes in cases of Delftia infection are in most cases good with patients recovering completely. Delftia spp are usually susceptible to several different antimicrobial classes, including carbapenems and fluoroquinolones. This indicates that issues posed by Delftia spp infections should be dealt with in the context of surveillance of non-fermenting Gram-negative bacteria generally, rather than be seen as a concern in and of itself in infection control. Overall, the available evidence supports the view of Delftia as rare, (usually) treatable opportunistic pathogens.
CRediT authorship contribution statement
Michael P. Ryan: Writing – review & editing, Writing – original draft, Investigation, Data curation, Conceptualization. J. Tony Pembroke: Writing – review & editing, Writing – original draft, Data curation, Conceptualization.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Di Pilato V.Willison E.Marchese A.The microbiology and pathogenesis of nonfermenting Gram-negative infections Curr Opin Infect Dis 36202310.1097/QCO.0000000000000969 PMC 1062440337732777 · doi ↗ · pubmed ↗
- 2Lipuma J.J.Currie B.J.Peacock S.J.Vandamme P.A.R.Burkholderia, stenotrophomonas, ralstonia, cupriavidus, pandoraea brevundimonas, comamonas, delftia, and acidovorax Manual of Clinical Microbiology 201510.1128/9781555817381.ch 43 · doi ↗
- 3Carraturo F.Carmela D.G.Compagnone M.Libralato G.Toscanesi M.Trifuoggi M.Evaluation of microbial communities of bottled mineral waters and preliminary traceability analysis using ngs microbial fingerprints Water (Switzerland)13202110.3390/w 13202824 · doi ↗
- 4Handschuh H.Ryan M.P.O'Dwyer J.Adley C.C.Assessment of the bacterial diversity of aircraft water: identification of the frequent fliers P Lo S One 12201710.1371/journal.pone.0170567 PMC 525695828114359 · doi ↗ · pubmed ↗
- 5Penna V.T.C.Martins S.A.M.Mazzola P.G.Identification of bacteria in drinking and purified water during the monitoring of a typical water purification system BMC Public Health 2200210.1186/1471-2458-2-13PMC 12209212182763 · doi ↗ · pubmed ↗
- 6Vincenti S.Quaranta G.De Meo C.Bruno S.Ficarra M.G.Carovillano S.Non-fermentative gram-negative bacteria in hospital tap water and water used for haemodialysis and bronchoscope flushing: prevalence and distribution of antibiotic resistant strains Sci Total Environ 499201410.1016/j.scitotenv.2014.08.04125173861 · doi ↗ · pubmed ↗
- 7Ryan M.P.Adley C.C.The antibiotic susceptibility of water-based bacteria Ralstonia pickettii and Ralstonia insidiosa J Med Microbiol 62201310.1099/jmm.0.054759-023579396 · doi ↗ · pubmed ↗
- 8Thoma B.Straube E.Scholz H.C.Al Dahouk S.Zöller L.Pfeffer M.Identification and antimicrobial susceptibilities of ochrobactrum spp International Journal of Medical Microbiology 299200910.1016/j.ijmm.2008.06.00918755630 · doi ↗ · pubmed ↗