Aspergillus Serology Predicts Relapse in Chronic Pulmonary Aspergillosis: Implications for Personalised Follow‐Up Strategies
Annabel Choyce, Stefano Colombo, Cyrin Cyriac, Abdulrazaq Alasfour, Wai Kien Ng, Lauren Amphlett, Chris Kosmidis

TL;DR
This study shows that blood tests for Aspergillus can predict if patients with lung aspergillosis will relapse after treatment, suggesting personalized follow-up strategies.
Contribution
The study identifies Aspergillus-specific IgE and IgG as novel predictors of relapse in chronic pulmonary aspergillosis.
Findings
Aspergillus sensitization and elevated IgG levels were independently linked to relapse.
No relapses occurred in patients with IgG levels below 40 mg/L.
Underlying lung disease or treatment duration did not predict relapse.
Abstract
Relapses occur in up to 40% of patients after prolonged courses of antifungal treatment for chronic pulmonary aspergillosis (CPA). The factors predisposing to relapse remain poorly defined. We conducted a retrospective study of adults treated for ≥ 6 months with oral azoles for CPA. Patients who completed antifungal therapy and were deemed not to require further treatment were included. Demographic, clinical, radiological and serological data at treatment completion were collected. CPA relapse was defined as symptomatic and radiological deterioration leading to re‐initiation of antifungal therapy. Cox regression and Kaplan–Meier analyses were used to identify predictors of relapse and mortality. Among 125 patients (56% male; mean age 61 years), median treatment duration was 36 months. Thirty‐two (26%) developed relapse; relapse rate at 1 year was 16%. Aspergillus sensitisation…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
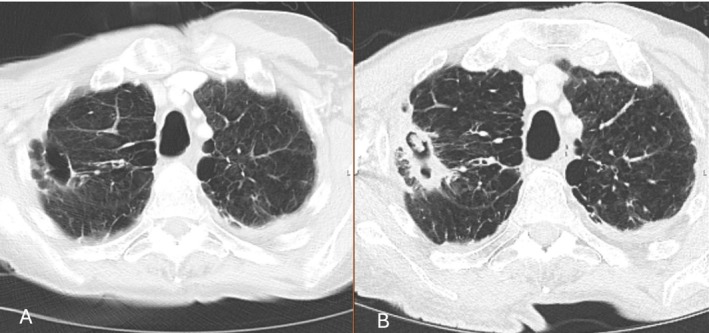 FIGURE 1
FIGURE 1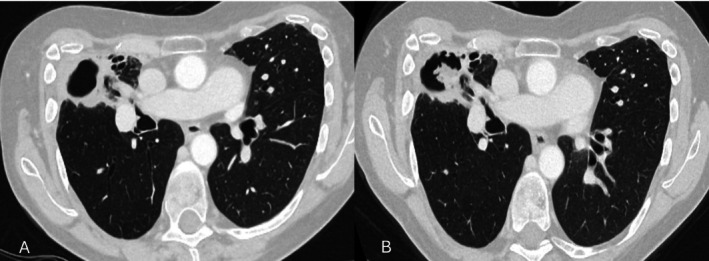 FIGURE 2
FIGURE 2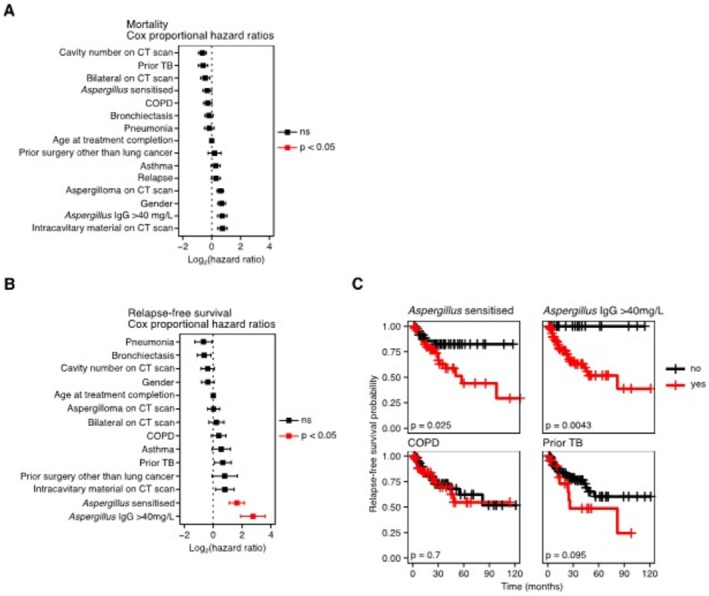 FIGURE 3
FIGURE 3|
| |
|---|---|
| Underlying disease predisposing to CPA | |
| COPD | 55 (44) |
| Bronchiectasis | 47 (38) |
| Asthma | 24 (19) |
| Prior tuberculosis | 23 (18) |
| Prior pneumonia | 21 (17) |
| Prior chest surgery | 16 (13) |
| Prior cancer | 13 (10) |
| Sarcoid | 10 (8) |
| Pneumothorax | 10 (8) |
| ABPA | 8 (6) |
| Prior NTM‐PD | 8 (6) |
| Rheumatoid arthritis | 8 (6) |
| Interstitial lung disease | 4 (3) |
| Ankylosing spondylitis | 1 (1) |
| Other conditions | |
| Diabetes | 9 (7) |
| Heart failure | 8 (6) |
| Renal failure | 3 (2) |
| First antifungal agent | |
| Voriconazole | 57 (46) |
| Itraconazole | 51 (41) |
| Posaconazole | 15 (12) |
| Isavuconazole | 2 (2) |
|
| 84 (7–1187) |
| Total IgE, median (range), IU/mL | 89 (2–13285) |
|
| 50 (48%) |
| Features on CT scan at treatment completion | 47 (38) |
| Bilateral disease | |
| Presence of cavity | |
| None | 12 (10) |
| One | 70 (56) |
| More than one | 43 (34) |
| Presence of aspergilloma | |
| None | 65 (52) |
| One | 48 (38) |
| More than one | 12 (10) |
| Radiological change |
|
|---|---|
| Increase in cavity wall thickness | 10 (31) |
| Enlargement of existing cavity | 9 (28) |
| Progression of peri‐cavitary consolidation | 9 (28) |
| Increase in aspergilloma size | 8 (25) |
| New aspergilloma | 7 (22) |
| New cavity | 4 (13) |
| Increase in pleural thickening | 2 (6) |
| New nodules | 2 (6) |
| Progressive fibrosis | 2 (6) |
| Enlarging nodules | 1 (3) |
| New fluid level | 1 (3) |
| Invasion of pulmonary artery | 1 (3) |
| Characteristics | Relapse ( | No relapse ( |
| OR (95% CI) |
|---|---|---|---|---|
| Age, mean ± SD | 59.8 ± 11.8 | 61.4 ± 11.7 | 0.494 | |
| Male | 16 (23) | 54 (77) | 0.536 | 0.72 (0.32–1.62) |
| Female | 16 (29) | 39 (71) | ||
| COPD | 14 (26) | 41 (75) | 0.974 | 0.99 (0.44–2.22) |
| Prior tuberculosis | 9 (39) | 14 (61) | 0.116 | 2.21 (0.85–5.76) |
| Asthma | 7 (29) | 17 (71) | 0.795 | 1.25 (0.47–3.37) |
| Bronchiectasis | 10 (21) | 37 (79) | 0.526 | 0.69 (0.29–1.62) |
| Prior pneumonia | 6 (29) | 15 (71) | 0.786 | 1.2 (0.42–3.41) |
| Aspergillus IgG at completion, mg/L, median (IQR) | 101 (89) | 76 (86) |
| |
|
| ||||
| < 40 | 0 (0) | 21 (100) |
| |
| > 40 | 31 (32) | 65 (68) | ||
| > 60 | 25 (32) | 53 (68) | 0.075 | 2.59 (0.96–6.99) |
| > 100 | 16 (35) | 30 (65) | 0.134 | 1.99 (0.87–4.58) |
|
| 18 (36) | 32 (64) |
| 3.3 (1.28–8.51) |
| Total IgE, IU/mL, median (IQR) | 172 (661) | 71 (275) | 0.083 | |
| Presence of aspergilloma on CT scan | 14 (24) | 45 (76) | 0.684 | 0.81 (0.36–1.82) |
| Bilateral disease on CT scan | 13 (28) | 34 (72) | 0.833 | 1.17 (0.51–2.66) |
| Cavity on CT scan | ||||
| No cavity | 1 (8) | 11 (92) | 0.225 | |
| One cavity | 17 (25) | 52 (75) | ||
| More than one cavity | 14 (33) | 29 (67) | ||
| Treatment duration | ||||
| 12 months or more | 26 (26) | 75 (74) | 0.940 | 1.04 (0.37–2.90) |
| < 12 months | 5 (25) | 18 (75) | ||
| Duration of treatment, months, median | 39.5 | 35 | 0.903 | |
| First treatment | ||||
| Itraconazole | 15 (29) | 36 (71) | 0.724 | |
| Voriconazole | 13 (23) | 44 (77) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntifungal resistance and susceptibility · Fungal Infections and Studies · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
1
Chronic pulmonary aspergillosis (CPA) is a progressive, indolent fungal infection that requires prolonged antifungal therapy. Standard management typically involves long‐term triazole treatment, as clinical improvement is often slow. Current guidelines recommend at least 6 months of therapy, followed by clinical, radiological and serological reassessment of treatment response [1]. In patients who demonstrate significant improvement, antifungal therapy may be discontinued, whereas others require extended or even indefinite treatment [1]. In patients who deteriorate despite antifungal treatment, emergence of azole resistance, subtherapeutic drug levels or alternative pathology need to be considered.
Despite these prolonged treatment courses, relapse is common, with reported rates ranging from 21% to 39% [2, 3, 4, 5, 6, 7]. Relapse is most often defined as clinical and radiological deterioration after completing at least 6 months of antifungal therapy, although some studies have also incorporated serological or microbiological criteria [6]. Management of relapse is particularly challenging due to the risk of azole resistance, further progression of lung disease and the impact of declining respiratory reserve and frailty. Moreover, relapses may go undetected in patients who are lost to follow‐up once treatment is discontinued.
Although diagnostic and therapeutic strategies for CPA have advanced, the factors that predispose to relapse remain poorly understood. Duration of therapy, baseline disease burden and serological markers have each been proposed as potential contributors, but evidence is limited [3, 4, 5, 6, 7]. Better understanding of the risk factors for relapse could support a more personalised approach to CPA management by identifying patients who may benefit from closer surveillance or extended, potentially lifelong antifungal treatment.
In this study, we evaluate clinical, radiological and serological parameters at the time of treatment completion to identify predictors of relapse in CPA.
Materials and Methods
2
Patients
2.1
This was a retrospective study of adult patients who received at least 6 months of azole treatment for CPA at the National Aspergillosis Centre, Manchester.
Patients who finished a course of antifungal treatment of 6 months or longer and were deemed by the treating clinician not to require further antifungal treatment for CPA at that point were eligible. Patients who were switched from one antifungal agent to another, due to intolerance or resistance, were included as long as the treatment gap between the antifungal agents was < 6 weeks. This was allowed in order to account for the common real‐world situation when treatment is halted until side effects of treatment such as raised liver function tests return to baseline before a different azole is introduced as part of the same treatment course.
Data Collection and Definitions
2.2
The information collected involved demographics, pulmonary and other co‐morbidities, antifungal treatment (start and stop date), extent of disease on imaging at the time of treatment completion (unilateral vs. bilateral, number of cavities, presence of aspergillomas) and Aspergillus serology. As this was a real‐world study, the CT scan closest to the treatment completion date was selected, provided it was performed within 3 months of the date of treatment completion. Serum concentrations of Aspergillus IgG, total IgE and Aspergillus‐specific IgE were recorded if they were available within 3 months of the date of treatment completion. Patients were defined as Aspergillus‐sensitised when Aspergillus‐specific serum IgE concentration was > 0.35 IU/mL. Aspergillus‐specific IgG and IgE were measured using the ImmunoCAP assay (Thermo Fisher Scientific).
CPA relapse was defined as: (a) symptoms suggestive of CPA as assessed in contemporaneous clinical notes, prompting a chest CT scan, (b) CT scan findings suggestive of CPA relapse, (c) reasonable exclusion of alternative diagnoses by the clinical team and (d) a clinical decision to re‐initiate antifungal treatment. CT scan features deemed suggestive of CPA relapse included a new or enlarging aspergilloma, a new or enlarging cavity, increased cavity wall thickness, increased pleural thickening and increasing consolidation surrounding a preexisting cavity.
The date of documented relapse or the time of the last clinical follow up or death were recorded.
This retrospective study analysed anonymised data collected during routine clinical care. No additional procedures were performed, and all data were anonymised prior to analysis; formal research ethics committee approval and individual patient consent were not required.
Statistical Analysis
2.3
Statistical analysis was performed using R version 4.4.1. For analysis of risk factors associated with mortality the period of assessment was defined as from the date of initial diagnosis of CPA to the date of outcome (death or censor). For analysis of relapse‐free survival the period of assessment was defined as from the date of treatment ending to the date of relapse assessment. Clinical characteristics (Table 1) present in > 10% of the cohort were selected for risk‐factor analysis. Multivariate Cox proportional hazards regression models were fitted to the data using the ‘survival’ package, version 3.6‐4. Kaplan–Meier plots were generated using the ‘survival’ package. Univariate statistical comparisons were calculated via log‐rank test using the ‘survminer’ package, version 0.4.9.
Results
3
125 patients completed at least 6 months of azole treatment for CPA and were followed for relapse. Seventy (56%) were male and mean age at completion of treatment was 61 years (range 25–83). Median duration of antifungal treatment was 36 months (range 6–216 months). Patient characteristics are presented in Table 1.
Thirty‐two (26%) patients had a relapse. The radiological features of relapse are described in Table 2. An example of a case of relapse based on CT imaging, which shows a new cavity with aspergilloma formation is shown in Figure 1. A further case with a new aspergilloma within a preexisting cavity is shown in Figure 2. Among 100 patients who had follow up data for more than 12 months, 16 (16%) had a relapse within a year after completing the antifungal treatment. The characteristics of patients with and without a relapse are presented in Table 3. Patients with prior TB had a median Aspergillus IgG of 121.5 mg/L compared to 82 mg/L for those without TB (p = 0.090). There were no significant differences in the rates of Aspergillus sensitisation between patients with prior TB or COPD.
Follow‐up chest imaging of a 75‐year‐old man with COPD. (A) CT scan at end of antifungal treatment. (B) One year after stopping antifungal therapy, the scan shows reappearance of a fungal ball within the cavity, thickening of the cavity wall, and adjacent pulmonary consolidation.
56‐year‐old woman with a past medical history of asthma, bronchiectasis and previous thoracic surgery for pectus excavatum. She was previously treated with voriconazole for 2 years and discontinued therapy due to clinical stability. (A) CT scan at end of treatment. (B) One year after stopping antifungal treatment, she reported worsening dyspnoea and a productive cough. A CT scan demonstrates a new fungal ball within the right upper lobe cavity.
Twenty‐one patients (17%) were dead at the time of the last follow up. Cox regression analysis of risk factors associated with mortality did not identify any variables to be significantly associated with mortality (Figure 3A). However, Cox regression analysis of the risk factors associated with relapse identified Aspergillus‐sensitization and an anti‐Aspergillus serum IgG concentration > 40 mg/L to be associated with a greater probability of relapse (Figure 3B). This was confirmed by Kaplan–Meier analysis with univariate log‐rank testing (Figure 3C). Notably, COPD and a prior history of TB were not significantly associated with an increased probability of relapse (Figure 3C).
Anti‐Aspergillus serum IgE and IgG is associated with relapse. (A, B) Dot plots representing the results of a multi‐variate Cox regression analyses of (A) risk factors for mortality in CPA and (B) risk factors for relapse. Points indicate Log2 transformed hazard ratios. Error bars indicate the standard error. Black points indicate non‐statistically significant factors. Red points indicate risk factors where p < 0.05 as calculated by Cox proportional hazards regression. (C) Kaplan–Meier curves of selected risk factors for relapse‐free survival. Vertical lines indicate where patients were censored. Black lines indicate where the risk factor was not present. Red lines indicate presence of the risk factor. p values were calculated by univariate log‐rank test.
Discussion
4
In this retrospective analysis we assessed factors associated with post‐treatment relapse in CPA. Our results demonstrate that the presence of Aspergillus sensitization and of a higher Aspergillus‐specific IgG titre at completion of antifungal treatment were independently associated with the risk of subsequent relapse. Therefore, we propose that these markers can be used to identify patients who would benefit from a more frequent or more prolonged follow‐up after treatment. In contrast, we did not find a statistically significant link between relapse and underlying lung conditions such as COPD or prior TB. This suggests that the fungal burden in the airways may be a more important determinant of the risk of CPA relapse than the underlying medical background of the host. However, we did observe a trend for more frequent relapse in patients with prior TB. As only 23 of the patients included in this study had a prior history of TB (9 of whom relapsed) it is possible that our analysis of this co‐morbidity was underpowered and further analysis with a larger sample size may identify a significant association between this risk factor and relapse.
The Aspergillus‐specific IgG titre is used both in diagnosis and in the monitoring of CPA on and off treatment. While it is expected and desirable to most clinicians that the titre should reduce on treatment, there is no universally accepted practice on its interpretation to guide treatment decisions. In a consensus statement by CPAnet, a clinical research group, it was not recommended that Aspergillus‐specific IgG be used to assess treatment response [8]. Furthermore, it is not currently used as a test of cure or as a prognostic marker. Occasionally, the titre falls below the laboratory determined cutoff (< 40 mg/L with the ImmunoCAP assay in our laboratory) which may provide reassurance that the burden of disease is so low that treatment can be safely discontinued. We found that no patient with a titre < 40 mg/L after at least 6 months of antifungal treatment had a relapse, supporting this assumption. Therefore, a higher Aspergillus IgG level at treatment completion may necessitate the need for a closer follow up for relapse. However, the relationship between airway fungal burden and Aspergillus‐specific IgG titres is not defined. The Aspergillus‐specific IgG titre may reflect the humoral response maintained by long‐lived plasma cells, or may fluctuate more short‐term based on ongoing antigenic stimulation in the airways. More likely, both mechanisms may contribute: *Aspergillus‐*specific IgG tends to fall with antifungal treatment, suggesting a response to the reducing fungal airway burden, whereas in most cases an elevated titre remains even after improvement of symptoms and cessation of antifungal therapy, suggesting long‐term memory.
Aspergillus sensitisation is common in CPA and seen in almost half of our cohort, although very few had a diagnosis of allergic bronchopulmonary aspergillosis (ABPA). Aspergillus sensitisation appears to be a feature of CPA independent of the presence of chronic airways disease, as Sehgal et al. [5] reported it in 40% of patients in their CPA cohort after excluding all patients with asthma and COPD. We found that Aspergillus‐sensitised patients were 3 times more likely to develop CPA relapse compared to the non‐*Aspergillus‐*sensitised. Sehgal et al. [5] also reported an association between Aspergillus sensitisation and relapse. This may be due to an increased predisposition in these patients for recurrent colonisation with Aspergillus and inability to effectively clear it, triggering an exaggerated Th2 response which may manifest as progressive symptoms and radiological findings. Such patients should receive closer follow up for relapse.
Unlike other studies, we did not find an association between the extent of disease and relapse. In a previous study, Bongomin et al. [6] identified bilateral disease as a risk factor for relapse. However, in that study not all patients had radiological confirmation or relapse. Similarly, Koyama et al. [7] identified multilobal involvement as linked with relapse. However that study used precipitin positivity rather than a specific IgG titre with one of the newer immunoassays and did not evaluate Aspergillus sensitisation.
Patients with CPA may have a number of different underlying diseases which in theory could affect the risk of relapse, such as COPD or asthma, possibly due to the use of inhaled or oral steroids. Neither we nor others have demonstrated significantly higher relapse rates according to a specific underlying disease. Interestingly, patients with prior TB exhibited a trend for higher relapse rates, although this did not reach statistical significance. This may be linked with the higher Aspergillus IgG observed in these patients on treatment completion compared to those without a history of TB. It is possible that the cavitary changes caused by prior TB may be more prone to fungal colonisation compared to cavities of a different causation.
We did not find an association between treatment duration and risk of relapse. However, we acknowledge that this study was not designed to assess the impact of treatment duration on the relapse risk, as a RCT would be required to adequately address this question. Sehgal et al. [4] showed that patients who were randomised to receive 12 months of treatment had fewer relapses within the follow up period. In this study, patients received treatment for longer periods compared to other reported cohorts, reflecting different treatment practices, most likely due to concern by the treating clinician about the relapse risk. Despite these more prolonged regimens, 1 in 4 patients developed relapse, similar to what has been reported in cohorts treated for shorter periods [2, 3, 4, 5, 6, 7]. Therefore, it is possible that long‐term azole treatments may still not reduce the risk of relapse in patients with risk factors such as Aspergillus sensitisation or a high Aspergillus IgG. Different approaches like combination antifungal therapies should be explored in clinical trials for such patients.
In conclusion, we find that Aspergillus sensitisation and a higher Aspergillus‐specific serum IgG concentration on completion of treatment were predictive of relapse in CPA, whereas underlying conditions or extent of disease on imaging were not. We suggest that patients with these serological parameters be followed closely after treatment completion and counselled about the risk of relapse to inform decisions about therapy discontinuation.
Author Contributions
Annabel Choyce: investigation, methodology, validation, writing – original draft. Stefano Colombo: methodology, software, formal analysis, writing – original draft. Cyrin Cyriac: investigation, data curation, visualisation. Abdulrazaq Alasfour: investigation, data curation, visualisation. Wai Kien Ng: investigation, data curation, visualisation. Lauren Amphlett: project administration, resources, visualisation. Chris Kosmidis: conceptualization, writing – original draft, writing – review and editing, formal analysis, supervision, methodology.
Funding
The authors have nothing to report.
Conflicts of Interest
Chris Kosmidis has received speaker's fees from Pfizer and consultation fees from Mundipharma and Shionogi Europe. The other authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1D. W. Denning , J. Cadranel , C. Beigelman‐Aubry , et al., “Chronic Pulmonary Aspergillosis: Rationale and Clinical Guidelines for Diagnosis and Management,” European Respiratory Journal 47 (2016): 45–68.26699723 10.1183/13993003.00583-2015 · doi ↗ · pubmed ↗
- 2Y. Niu , J. Li , W. Shui , et al., “Clinical Features and Outcome of Patients With Chronic Pulmonary Aspergillosis in China: A Retrospective, Observational Study,” Journal of Medical Mycology 30 (2020): 101041.32950379 10.1016/j.mycmed.2020.101041 · doi ↗ · pubmed ↗
- 3Y. Im , B. W. Jhun , E. S. Kang , W. J. Koh , and K. Jeon , “Impact of Treatment Duration on Recurrence of Chronic Pulmonary Aspergillosis,” Journal of Infection 83 (2021): 490–495.34332020 10.1016/j.jinf.2021.07.030 · doi ↗ · pubmed ↗
- 4I. S. Sehgal , S. Dhooria , V. Muthu , et al., “Efficacy of 12‐Months Oral Itraconazole Versus 6‐Months Oral Itraconazole to Prevent Relapses of Chronic Pulmonary Aspergillosis: An Open‐Label, Randomised Controlled Trial in India,” Lancet Infectious Diseases 22 (2022): 1052–1061.35429465 10.1016/S 1473-3099(22)00057-3 · doi ↗ · pubmed ↗
- 5I. S. Sehgal , S. Dhooria , V. Muthu , et al., “Clinical Significance of Aspergillus Sensitisation in Chronic Pulmonary Aspergillosis,” Mycoses 67 (2024): e 70002.39613720 10.1111/myc.70002 · doi ↗ · pubmed ↗
- 6F. Bongomin , A. Otu , C. Harris , P. Foden , C. Kosmidis , and D. W. Denning , “Risk Factors for Relapse of Chronic Pulmonary Aspergillosis After Discontinuation of Antifungal Therapy,” Clinical Infection in Practice 5 (2020): 100015.
- 7K. Koyama , N. Ohshima , J. Suzuki , et al., “Recurrence of Chronic Pulmonary Aspergillosis After Discontinuation of Maintenance Treatment by Antifungal Triazoles,” Journal of Infection and Chemotherapy 20 (2014): 375–379.24679654 10.1016/j.jiac.2014.02.003 · doi ↗ · pubmed ↗
- 8E. Van Braeckel , I. Page , J. R. Davidsen , et al., “Treatment Outcome Definitions in Chronic Pulmonary Aspergillosis: A CP Anet Consensus Statement,” European Respiratory Journal 59 (2022): 2102950, 10.1183/13993003.02950-2021.35236726 · doi ↗ · pubmed ↗