Diaphragmatic Musculophrenic Vessel Injury Following Ultrasound-Guided Pigtail Catheter Insertion: A Rare Case
Jenna A Almannaei, Amena F Almubarak, Qasim A Alnahawi, Raja Nadeem, Ghassan Salman

TL;DR
A rare case of diaphragmatic artery injury after pigtail catheter insertion is reported, highlighting the potential risks of this procedure.
Contribution
This paper presents a rare complication of musculophrenic artery injury following ultrasound-guided pigtail catheter insertion.
Findings
A 39-year-old patient developed severe complications after pigtail catheter insertion, including hydropneumothorax and arterial injury.
Intraoperative findings confirmed musculophrenic artery injury at the diaphragmatic surface.
Prompt recognition and surgical intervention led to successful recovery.
Abstract
Pigtail catheters are widely used as a minimally invasive substitute to large-bore chest tubes for the management of pleural effusion. Although it is considered safe, serious complications may occur. We report a rare case of diaphragmatic musculophrenic artery injury following ultrasound-guided pigtail catheter insertion. A 39-year-old female with multiple comorbidities was admitted with an impression of pleural effusion. She underwent ultrasound-guided pigtail catheter insertion, with drainage of hemorrhagic exudative fluid. Within one hour, she developed severe dyspnea and chest pain. Imaging revealed a hydropneumothorax, necessitating urgent intercostal chest drain placement. Despite initial clinical improvement, she rapidly deteriorated, prompting emergency thoracotomy. Intraoperative findings revealed a bleeding musculophrenic artery at the diaphragmatic surface, likely injured…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
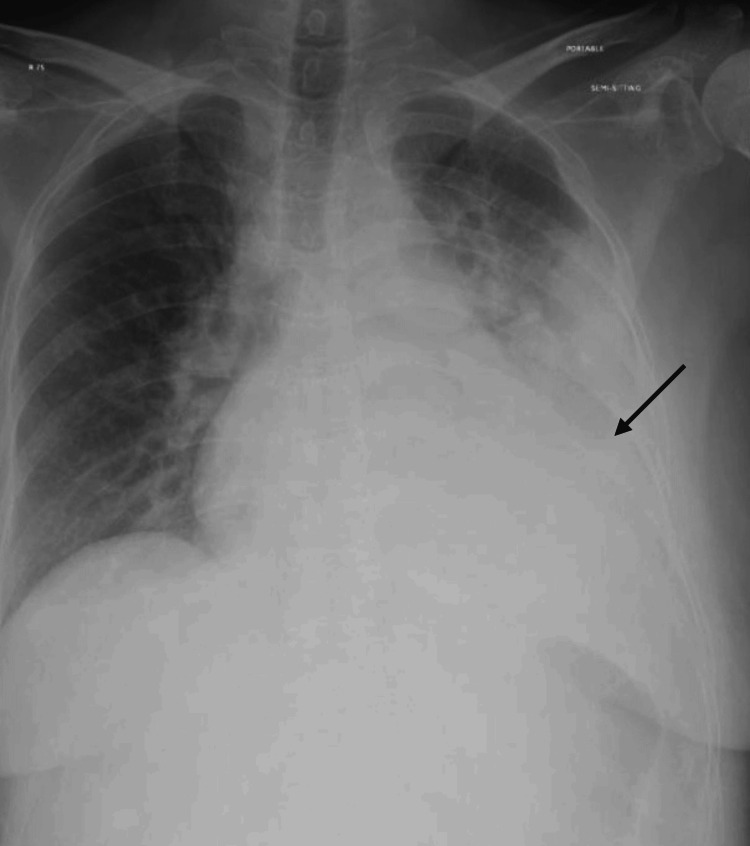 Figure 1
Figure 1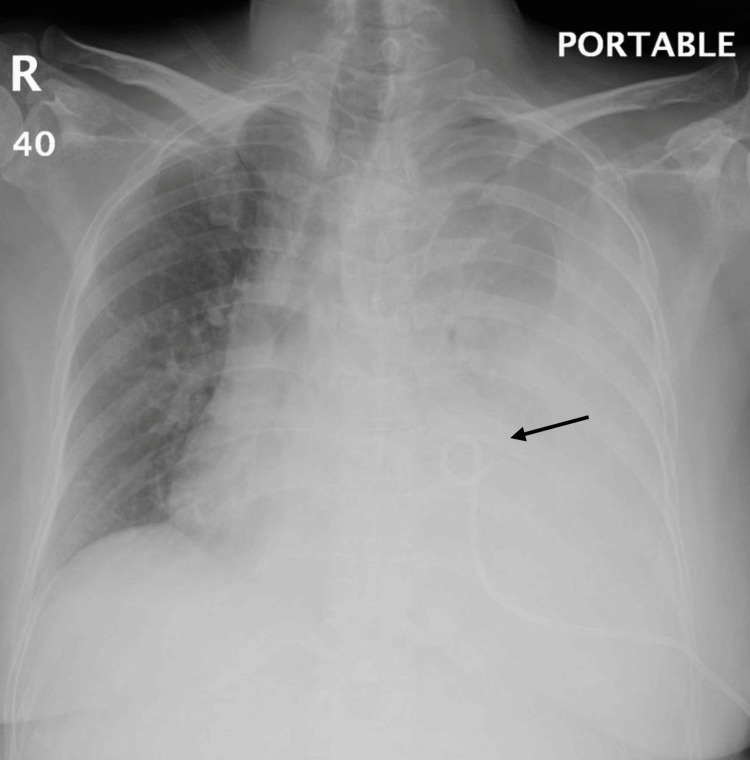 Figure 2
Figure 2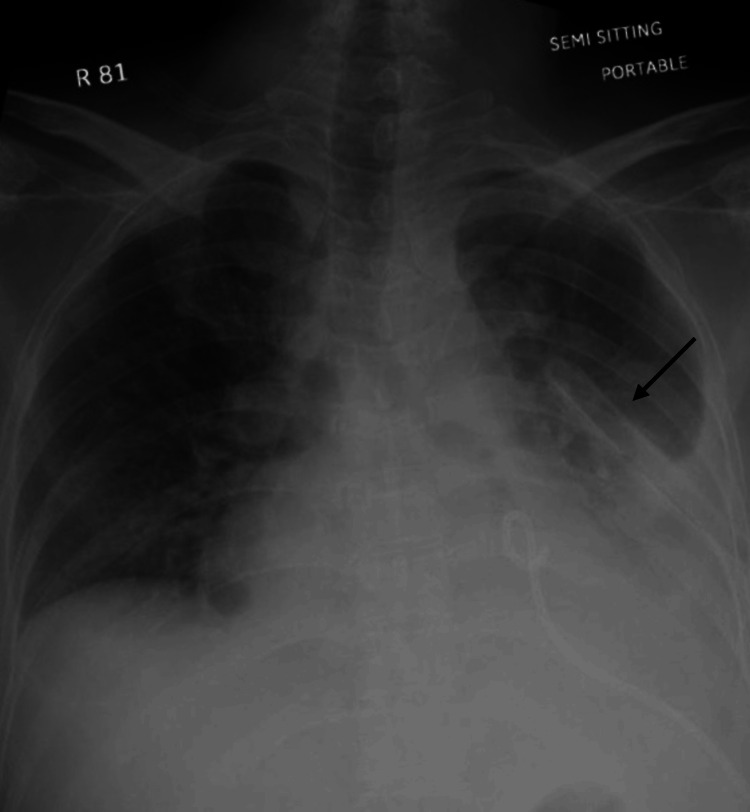 Figure 3
Figure 3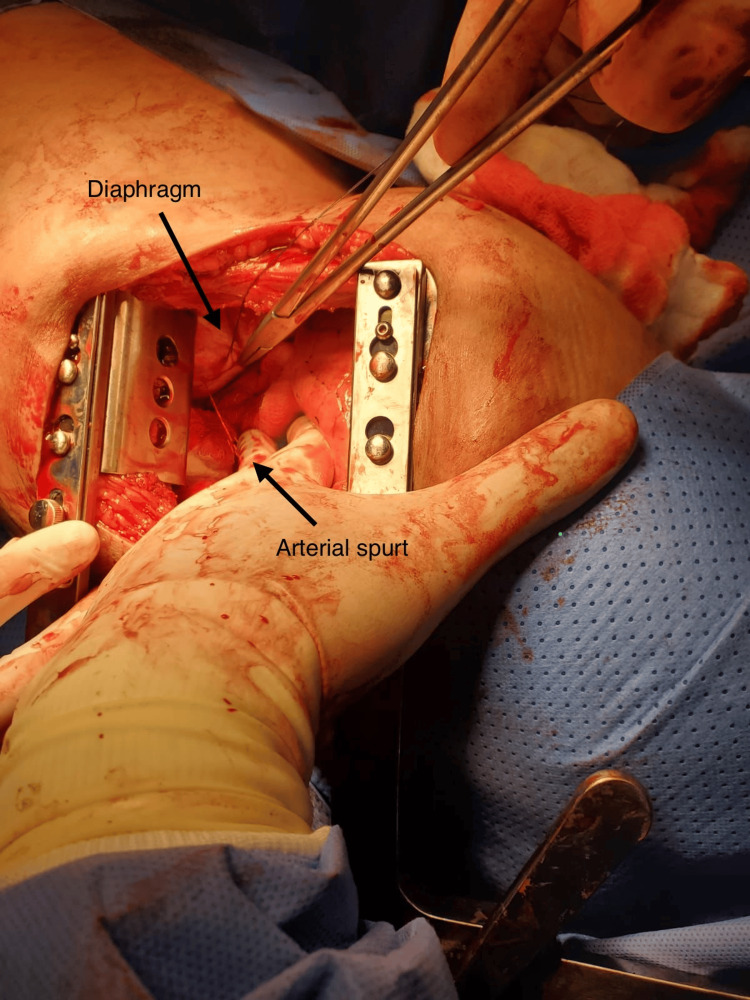 Figure 4
Figure 4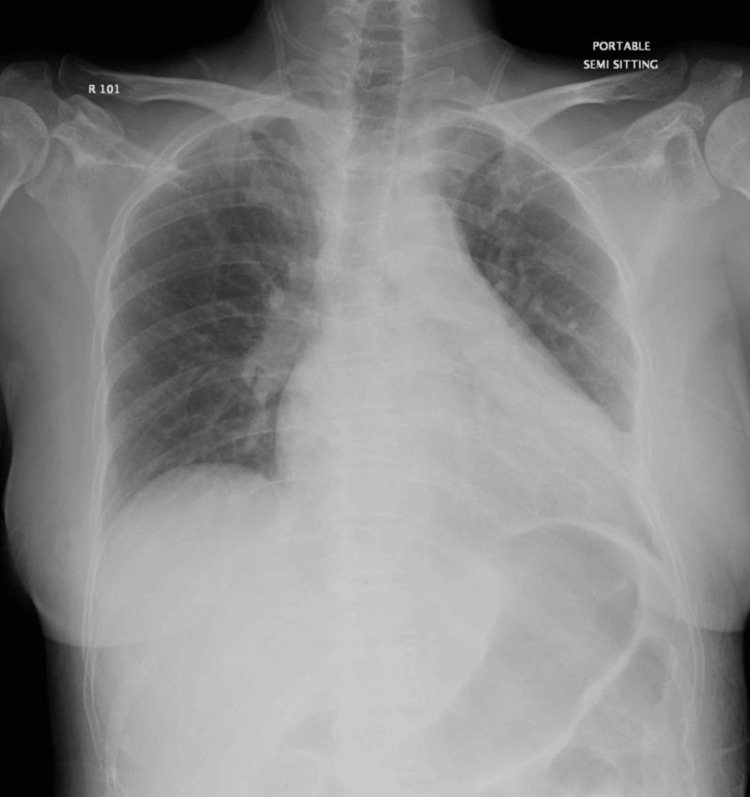 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPleural and Pulmonary Diseases · Trauma Management and Diagnosis · Ultrasound in Clinical Applications
Introduction
Pigtail catheters are widely used as a minimally invasive substitute to large-bore chest tubes for the management of pleural effusion and are generally well tolerated by patients. It is a small flexible tube used to drain collections from the pleural space in a minimally invasive approach. Pigtail catheters are inserted under ultrasound or CT guidance and are particularly used in draining pleural fluid with less trauma to tissues and less pain compared to traditional large-bore chest tubes. In a clinical setting, pigtail catheters are used for symptomatic pleural effusions, parapneumonic effusions, malignant pleural effusions, tuberculous effusions, and selected cases of pneumothorax, especially spontaneous or iatrogenic. Patients generally tolerate pigtail catheters well. These catheters allow continuous drainage while improving respiratory symptoms. However, due to their small diameter, they are not suitable for thick pus, clotted blood, or massive hemothorax. Complications are usually minor, including pain at the insertion site, catheter blockage, inadequate drainage, pneumothorax, and infection; however, more serious problems can occur, such as organ injury. Despite these risks, when used in appropriately selected patients and inserted under image guidance, including ultrasound with Doppler to avoid vascular injuries, pigtail catheters may be used for pleural drainage, with success and complications varying according to the clinical context. We report a rare case of musculoskeletal-phrenic artery injury following ultrasound-guided pigtail catheter insertion, highlighting that significant vascular injury can still occur when image guidance is used [1-3].
Case presentation
A 39-year-old female with a known diagnosis of multiple myeloma with several medical comorbidities was admitted with an impression of pleural effusion. She was afebrile and maintaining oxygen saturation of 97% on room air. On physical examination, decreased breath sounds were noted at the base of the left lung. Chest X-ray confirmed a moderate left-sided pleural effusion (Figure 1).
Chest X-ray showing moderate left-sided pleural effusion.
Subsequently, she underwent ultrasound-guided pigtail catheter insertion by the interventional radiology team at the level of the left fifth intercostal space, anterior axillary line. Approximately 600 mL of hemorrhagic pleural fluid was drained gradually.
Within one hour post-insertion, the patient developed sudden-onset dyspnea and severe left-sided chest pain. Vital signs indicated early hemodynamic compromise. Repeated chest X-ray revealed a newly developed pneumothorax with re-accumulation of pleural fluid consistent with a hydropneumothorax (Figure 2).
Chest X-ray showing left-sided hydropneumothorax after pigtail insertion.
An emergency 28-French intercostal chest drain was placed at the level of the fourth intercostal space mid-axillary line under local anesthesia, with immediate drainage of 1,900 mL of mixed fresh and clotted blood. Chest radiograph confirmed correct positioning of the intercostal chest drain (Figure 3). The patient initially stabilized and showed improvement in symptoms.
Chest X-ray after the insertion of left-sided intercostal chest drain.
However, approximately 15 minutes later, she experienced acute hemodynamic deterioration. The thoracic surgery team was urgently consulted, and the patient was taken to the operating room for emergency left thoracotomy for bleeding control. Intraoperatively, approximately 600 mL of clotted blood was evacuated. A spurting arterial bleeder was identified on the diaphragmatic surface, suspected to be an injured musculophrenic artery (Figure 4). Hemostasis was achieved surgically.
Intraoperative image showing a spurting arterial bleeder on the diaphragmatic surface.
The patient recovered uneventfully postoperatively and was discharged from thoracic surgery care after approximately one week (Figure 5).
Postoperative chest X-ray showing resolved hemothorax, expanded left lung, and absence of pneumothorax. Chest tube has been removed.
Discussion
Pigtail catheters, due to their small caliber, flexible nature, and enhanced patient comfort, are increasingly used in clinical practice. Despite their overall safety, complications such as pneumothorax, hemothorax, infection, and misplacement may still occur [1-3]. In particular, injuries to intercostal vessels or the diaphragmatic surface are considered exceedingly rare but potentially fatal [2,4]. In our case, the guidewire or catheter most likely penetrated the diaphragm and injured a diaphragmatic intercostal artery, resulting in hemothorax and hemodynamic instability.
Rare cases involving a similar mechanism of injury have been reported. Park and Lee described a case of massive hemothorax due to intercostal arterial bleeding after pigtail removal [4]. Likewise, Casper et al. reported a pseudoaneurysm of the intercostal artery after thoracentesis requiring coil embolization [5]. These reports, along with ours, illustrate the risk posed to vascular structures in the thoracoabdominal junction, especially when insertion is performed close to the diaphragm.
Standard ultrasound-guided thoracostomy significantly reduces complications by enabling visualization of adjacent structures; however, it cannot eliminate them entirely. Studies have shown that using color Doppler ultrasound adds another layer of safety by identifying intercostal vessels, especially when accessing lower intercostal spaces (e.g., below the eighth rib) [1,6,7]. Techniques such as lowering the pulse repetition frequency and adjusting imaging depth improve Doppler sensitivity, enhancing visualization of vascular flow in small intercostal branches [1,7,8]. Unfortunately, color Doppler remains underutilized in bedside procedures despite its demonstrated utility [1,6].
Furthermore, selecting an appropriate insertion site is another critical factor. Intercostal arteries typically run along the inferior margin of each rib and are more prominent and exposed in lower thoracic spaces. Literature suggests that higher intercostal thoracostomies (fourth to sixth spaces) are safer in terms of avoiding major structures [3,9,10]. Although lower intercostal tube insertions (seventh or below) may be necessary to access dependent fluid collections, they carry a higher risk of vascular and diaphragmatic injury [2,9].
In our case, the suspected injury to a diaphragmatic musculophrenic artery was likely caused by guidewire penetration beyond the pleural space into the diaphragm. This rare complication underscores the importance of procedural precision, the potential benefit of color Doppler imaging, and avoiding unnecessarily low punctures without clinical indication.
Prompt identification and immediate surgical intervention were lifesaving in our case. In previously reported cases, both coil embolization and thoracotomy have been successfully employed depending on the patient’s hemodynamic status and severity of bleeding [4,5,9].
It is equally essential to underscore the importance of vigilance during and after placement of the pigtail catheter in the early detection of complications and management accordingly. Confirming pleural entry before inflation of the pigtail balloon by aspirating can add another layer of safety and help prevent accidental penetration of non-pleural structures [11].
Close observation after the procedure remains vital. New symptoms such as chest pain, an increase in bloody output, unstable vital signs, and a sudden drop in hemoglobin level can be early signs of significant complications [12]. A preemptive approach by remaining alert for clinical deterioration and initiating prompt imaging and intervention when required is key to avoiding diagnostic delays and reducing potential harm to the patient [13,14].
Conclusions
This case highlights a rare but fatal complication following the placement of an ultrasound-guided pigtail catheter, namely, diaphragmatic musculophrenic artery injury. Clinicians should remain vigilant during and after interventions involving the thoracic cavity, particularly when anatomical proximity to major vascular structures exists. Emergency surgical intervention may be required to manage such events and prevent mortality.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1An easier and safe affair, pleural drainage with ultrasound in critical patient: a technical note Crit Ultrasound J Vetrugno L Guadagnin GM Orso D Boero E Bignami E Bove T 181020183006609810.1186/s 13089-018-0098-z PMC 6068051 · doi ↗ · pubmed ↗
- 2Tube thoracostomy: complications and its management Pulm Med Kesieme EB Dongo A Ezemba N Irekpita E Jebbin N Kesieme C 256878201220122202896310.1155/2012/256878 PMC 3195434 · doi ↗ · pubmed ↗
- 3Thoracostomy tubes: a comprehensive review of complications and related topics Int J Crit Illn Inj Sci Kwiatt M Tarbox A Seamon MJ 143155420142502494210.4103/2229-5151.134182 PMC 4093965 · doi ↗ · pubmed ↗
- 4Massive hemothorax due to intercostal arterial bleeding after percutaneous catheter removal in a multiple-trauma patient: a case report World J Clin Cases Park C Lee J 99429947920213487733410.12998/wjcc.v 9.i 32.9942 PMC 8610904 · doi ↗ · pubmed ↗
- 5Intercostal artery pseudoaneurysm following thoracentesis: multi-modal imaging and treatment BMC Med Imaging Casper KP Sanchirico PJ Pfeiffer DC 311920193102909410.1186/s 12880-019-0333-5PMC 6487039 · doi ↗ · pubmed ↗
- 6Ultrasound-guided pigtail catheters for drainage of various pleural diseases Am J Emerg Med Liu YH Lin YC Liang SJ 9159212820102082592410.1016/j.ajem.2009.04.041 · doi ↗ · pubmed ↗
- 7Transthoracic ultrasonography in predicting the outcome of small-bore catheter drainage in empyemas or complicated parapneumonic effusions Ultrasound Med Biol Chen CH Chen W Chen HJ Yu YH Lin YC Tu CY Hsu WH 146814743520091961636610.1016/j.ultrasmedbio.2009.04.021 · doi ↗ · pubmed ↗
- 8Is the trocar technique for tube thoracostomy safe in the current era?Interact Cardiovasc Thorac Surg John M Razi S Sainathan S 1251281920142464846810.1093/icvts/ivu 071 · doi ↗ · pubmed ↗